Page 10 of 20
FM7.1 | Regional Injuries: Head, Neck, Trunk, Limbs & Spine — SDL Guide (Part 2)
Neck Injuries: Vascular, Airway and Soft Tissue
Neck injuries are of disproportionate forensic importance because vital structures — the carotid arteries, internal jugular veins, trachea, oesophagus, and spinal cord — are packed into a small, relatively unprotected space. Blunt or penetrating neck injuries can cause death rapidly through exsanguination, airway obstruction, or neurological disruption, and their forensic interpretation depends on understanding these mechanisms.
Vascular injuries of the neck encompass injury to the common carotid, internal carotid, external carotid, and vertebral arteries, and to the internal jugular, external jugular, and subclavian veins. Arterial injuries cause massive haemorrhage and carotid injury may also produce cerebral ischaemia by disrupting blood supply to the brain. Venous air embolism is a specific complication of large neck vein injuries — when the jugular vein is torn and lies above the level of the right heart (as when the neck is extended), air can be sucked into the venous system with each inspiratory effort, accumulating in the right heart and pulmonary artery to produce lethal obstruction of pulmonary circulation. Post-mortem, air embolism is suspected when the heart chambers contain foamy, gas-mixed blood and confirmed by submerging the heart and cutting it under water to observe bubbles.
Laryngotracheal injuries from blunt neck trauma (throttling, impact, manual strangulation) include thyroid cartilage fracture (the most common laryngeal injury in adults), hyoid bone fracture (important in strangulation — discussed in manual strangulation module), and tracheal rupture. Airway injuries cause asphyxia through swelling, haematoma, or direct disruption. Subcutaneous emphysema (surgical emphysema) over the neck from tracheal disruption is a clinical and post-mortem finding.
Penetrating neck injuries from stab wounds, firearm wounds, or foreign bodies require systematic assessment in the three anatomical neck zones (Zone I: clavicle to cricoid; Zone II: cricoid to angle of mandible; Zone III: above angle of mandible) — the zone determines which vessels and structures are at risk and guides surgical approach. Forensically, the zone of a penetrating wound helps reconstruct the weapon's angle and depth of penetration.
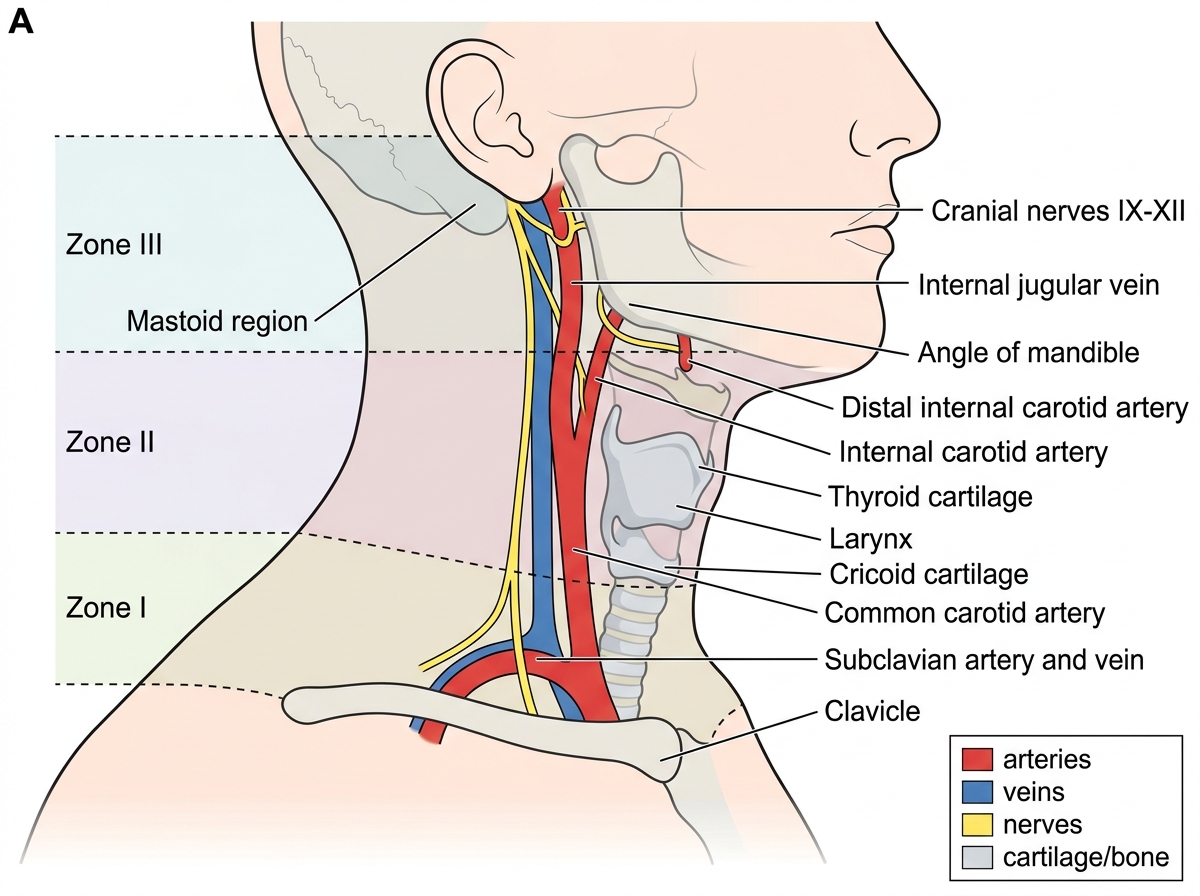
Surgical Zones of the Neck
Chest and Abdominal Injuries
Thoracoabdominal injuries are a major cause of death in blunt and penetrating trauma. Their forensic significance lies in identifying the mechanism (blunt vs penetrating), the specific structures damaged, and whether death was immediate (unsurvivable) or potentially treatable (survivable with prompt intervention — which can affect the IPC charge when negligence or withholding of treatment is alleged).
Rib fractures are the most common thoracic skeletal injury in blunt trauma. A flail chest results from multiple adjacent rib fractures in two places on each rib, creating a free-floating segment that moves paradoxically (inward on inspiration, outward on expiration) — this dramatically impairs ventilation. Rib fractures in the elderly can result from relatively minor forces because of osteoporosis; this has forensic implications when distinguishing assault from a 'trivial' fall. The site of rib fractures — anterior vs posterior, number of ribs, bilateral vs unilateral — helps reconstruct the direction and force of impact.
Pneumothorax (air in the pleural cavity) and haemothorax (blood in the pleural cavity) complicate rib fractures and penetrating chest wounds. A tension pneumothorax is a life-threatening emergency where air enters the pleural space but cannot exit; progressive accumulation shifts the mediastinum and compresses the contralateral lung and great vessels. Forensically, bilateral pneumothorax suggests bilateral chest compression (e.g., a vehicle running over the thorax).
Cardiac tamponade occurs when blood accumulates in the pericardial sac (which is inextensible), compressing the heart and preventing adequate filling — leading to cardiogenic shock and death. As little as 150–200 mL of blood in the pericardium can be fatal. At post-mortem, pericardial tamponade is found when the pericardial sac is opened and blood is found under pressure (the classic 'chicken-fat clot' over a yellow 'buffy coat' on longer-standing effusions).
Abdominal solid organ injuries — particularly hepatic and splenic lacerations — are major sources of haemoperitoneum and death. The liver is the largest abdominal solid organ and the most commonly injured in blunt trauma; it may 'burst' from sudden compression. The spleen is particularly prone to injury from left-sided rib fractures (ribs 9–11) and causes delayed splenic rupture in some cases (an initial injury that seems trivial, followed by capsule rupture hours or days later). The mesentery can be torn by deceleration, causing haemorrhage and intestinal ischaemia. Hollow viscus injuries (small bowel perforation, bladder rupture) may be delayed in their presentation.
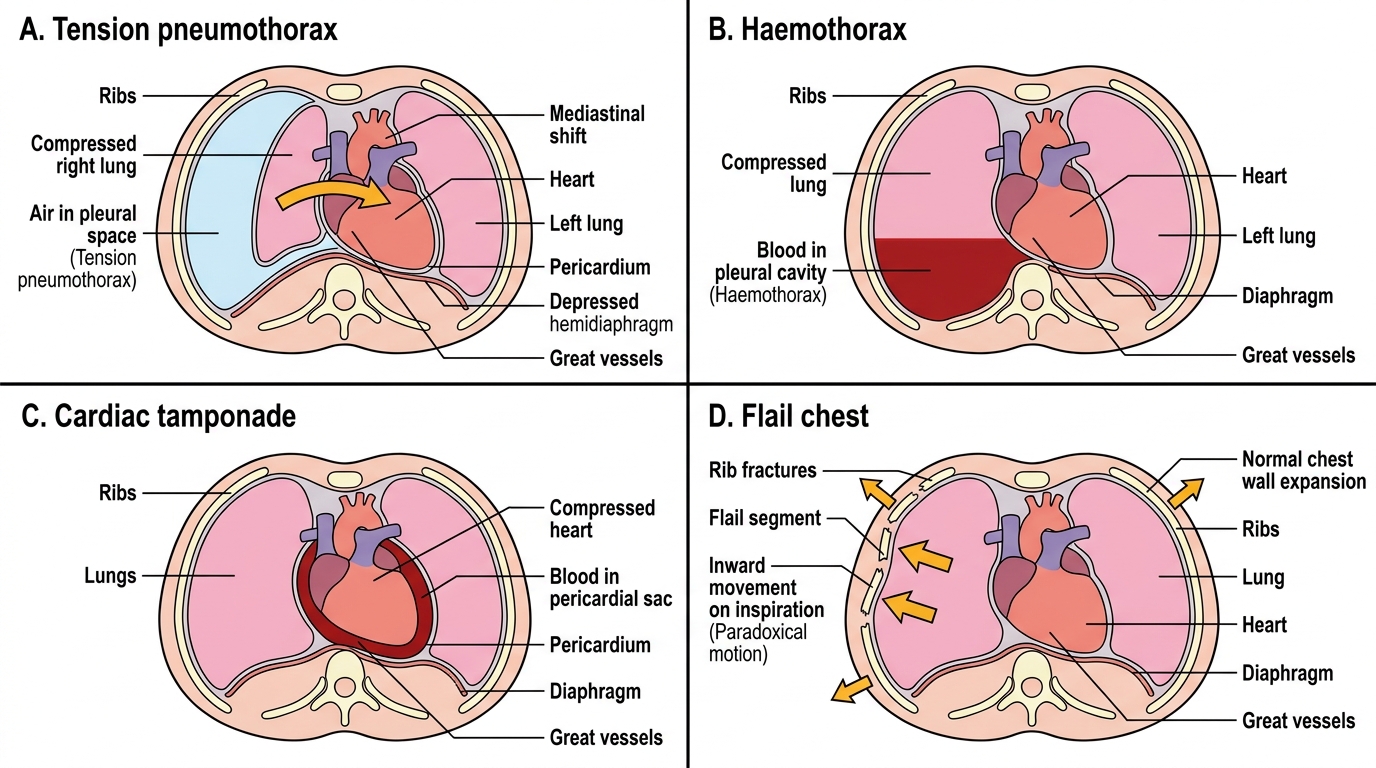
Life-Threatening Thoracic Injury Patterns
SELF-CHECK
A 25-year-old woman is found dead after being struck on the occiput (back of the head) with a blunt object. Post-mortem examination shows a scalp laceration and linear fracture at the occiput (coup), and brain contusions/lacerations at both frontal poles (contre-coup). The defence argues the brain injuries are 'inconsistent with the alleged blow' because they are distant from the fracture. How do you respond?
A. Agree — the brain injuries at the frontal poles indicate a separate blow to the forehead that was not documented at scene
B. Agree — frontal lobe injuries indicate the victim fell forward and struck her forehead, contradicting the allegation of a blow from behind
C. Disagree — frontal pole brain injuries from an occipital blow are the expected contre-coup mechanism; brain injury opposite to impact site is normal in deceleration-type head injury
D. Disagree — the contre-coup injuries indicate the victim was moving rapidly and hit a wall with the front of her head
Reveal Answer
Answer: C. Disagree — frontal pole brain injuries from an occipital blow are the expected contre-coup mechanism; brain injury opposite to impact site is normal in deceleration-type head injury
Frontal pole brain contusions/lacerations from an occipital impact are the textbook contre-coup mechanism: the skull impacts posteriorly, decelerates, and the brain continues moving forward by inertia, its anterior poles striking the rough floor of the anterior cranial fossa. This is entirely consistent with — and expected from — an occipital blow. The physician should explain the acceleration-deceleration mechanism clearly to the court and reject the defence argument that the brain injury location contradicts the alleged mechanism.
Limb, Genital and Spinal Cord Injuries
Limb injuries in forensic contexts range from patterned bruising (revealing the shape of the weapon) to complex fractures from high-energy trauma. Long bone fractures from blunt force show characteristic patterns based on force direction: transverse fractures from direct blows perpendicular to the bone axis; oblique or spiral fractures from torsional forces; comminuted fractures from high-energy impact. The butterfly fracture — a triangular bone fragment between two crack lines — indicates bending force with the apex of the triangle pointing in the direction of force application. These fracture patterns can help reconstruct the mechanism of injury and are relevant in both assault cases and road traffic accident investigations.
Genital organ injuries carry particular forensic significance because of their medico-legal implications in sexual assault cases and in assessment of grievous hurt (IPC 320(1) — emasculation). Blunt force to the external genitalia in males (kick, compression) produces severe contusion and haematoma, and rarely testicular rupture. Perineal injuries from blunt or penetrating trauma require careful documentation, including perianal abrasions and lacerations (relevant in anal penetration assessment). Any genital injury in a case with a history of sexual assault requires a full forensic sexual examination under the standard protocol.
Spinal cord injuries from trauma are classified into four grades that have direct bearing on prognosis and, in fatal cases, on the mechanism-of-death analysis:
Spinal cord concussion: Transient functional disturbance — complete loss of motor and sensory function below the injury level, lasting minutes to hours, with complete recovery. No structural damage visible on histopathology. Analogous to cerebral concussion. Important forensically because it explains the pattern of a victim who 'could not move' immediately after injury but recovered fully — the spine was not fractured.
Spinal cord contusion: Bruising of the cord substance — haemorrhage and oedema within the cord parenchyma — without complete anatomical disruption. Partial or incomplete recovery is possible.
Spinal cord laceration: Physical disruption of the cord parenchyma — permanent loss of function below the level. Complete or near-complete lesions produce spinal shock (flaccid paralysis, areflexia, autonomic instability) acutely, followed by spastic paraplegia if the victim survives.
Spinal cord haemorrhage (haematomyelia): Bleeding within the cord substance. May be associated with contusion or penetrating injury. Extent and level of haemorrhage determine prognosis.
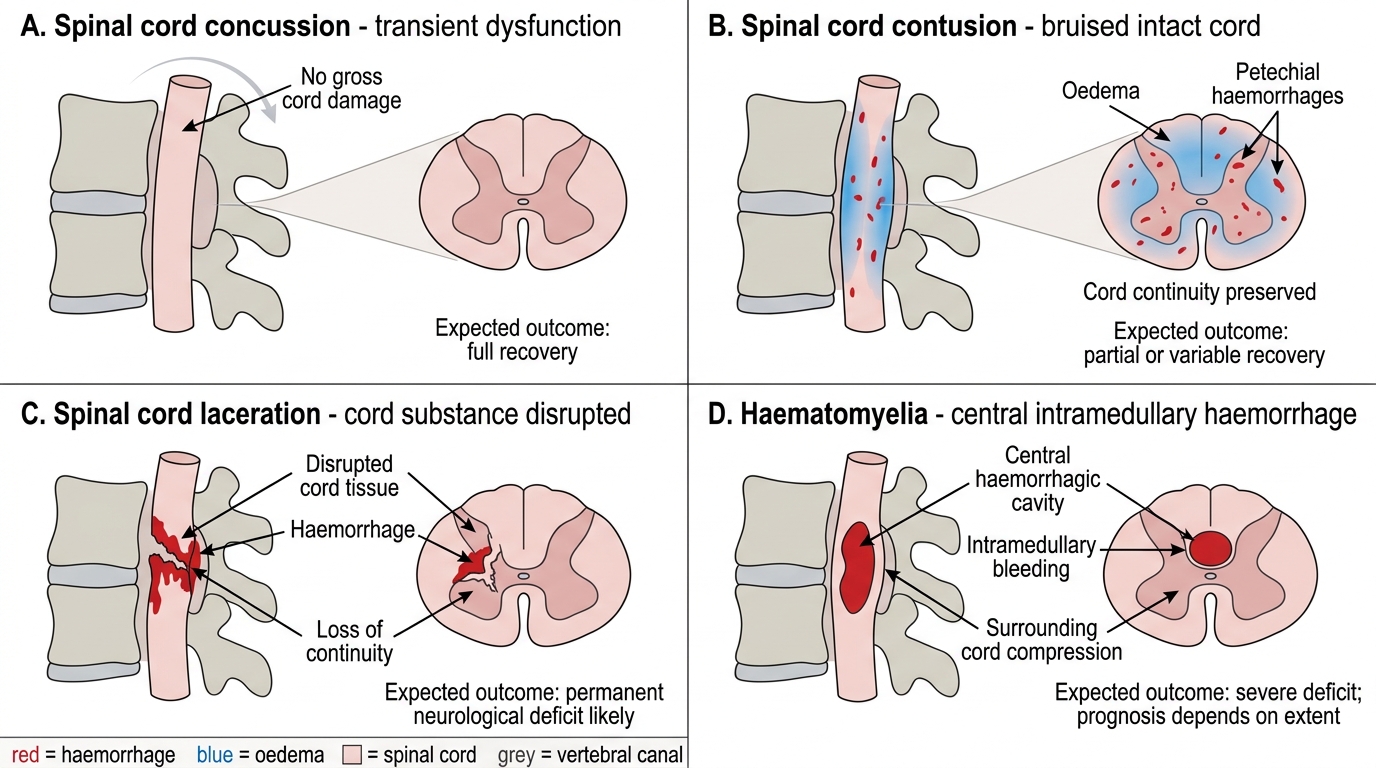
Grades of Spinal Cord Injury
CLINICAL PEARL
The lucid interval in epidural haematoma is a forensic trap. Defence counsel regularly argues that because the victim 'walked and talked' after the blow, the injury could not have been severe — implying the death resulted from medical negligence rather than the assault. The forensic physician must explain clearly that the lucid interval is a feature of the injury mechanism, not a sign that the injury was minor. An epidural haematoma from middle meningeal artery bleeding expands silently during the lucid interval, and transtentorial herniation — not the initial blow — is the mechanism of death. The blow was the but-for cause; the progression was the natural course of the injury. This is the foundation of the 'thin skull rule' in law: the attacker is responsible for the full consequences of the injury, including any unusual vulnerability of the victim, and the lucid interval does not sever the causal chain.