Page 11 of 20
FM7.1 | Regional Injuries: Head, Neck, Trunk, Limbs & Spine — SDL Guide (Part 3)
Clinical Examination and Systematic Injury Documentation
A forensic injury examination that cannot withstand cross-examination has no medico-legal value. The quality of the written report — its completeness, precision, and use of exact measurements — is what determines whether the physician's opinion survives challenge in court. The examination protocol must be head-to-toe, systematic, and reproducible.
Provided image
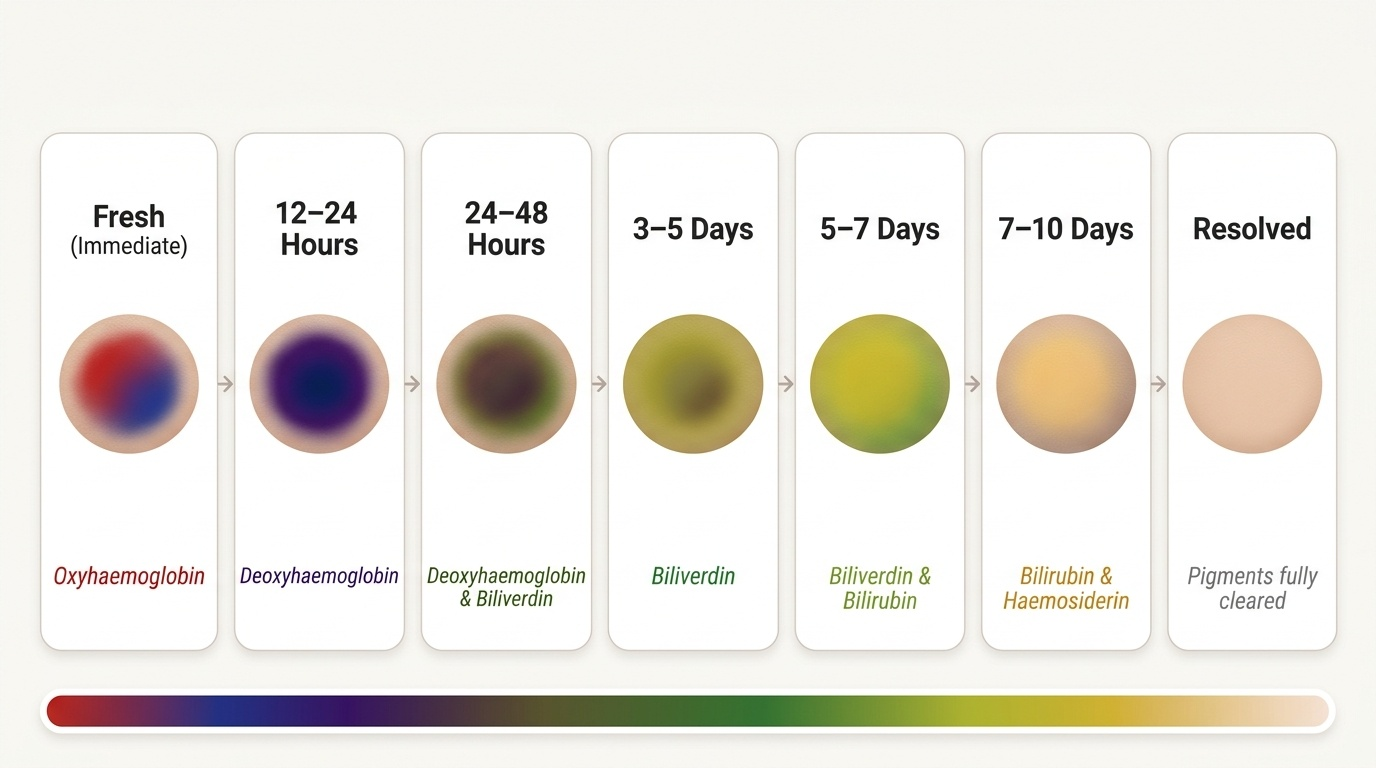
For each injury, document in the order: anatomical location (body region, distance from bony landmarks, side); dimensions (length × breadth for elongated injuries; diameter for circular ones); shape (contusion: irregular/round/patterned; laceration: stellate/linear; abrasion: linear/grouped); margins (contusion: ill-defined diffuse; laceration: irregular torn; incised: clean); depth (superficial = epidermis only; deep = dermis + subcutaneous; perforating = through structures); colour (fresh = red/blue; 12–24 h = dark purple; 24–48 h = brownish-green edges; 4–7 days = yellow-green; older = yellow/brown — age estimation requires caution as colour changes depend on skin tone, injury size, and overlying haematoma). Age estimation of injuries from colour is inherently uncertain and should be reported as a range.
Patterned injuries — injuries whose shape reproduces the contacting surface — are particularly valuable: a stellate laceration corresponding to a hammerhead, a linear parallel bruise corresponding to a belt buckle, a curved contusion from a boot heel. These must be measured, photographed with a scale ruler, and compared with any weapon seized by police.
Multiple injuries at different stages of healing indicate repeated assaults — a classic finding in domestic violence cases and child abuse. Document each stage with its colour, location, and estimated age range. Compare the injury ages with the reported history.
In fatal cases, the post-mortem examination extends the clinical documentation: intracranial injuries are exposed by calvaria removal and systematic examination of the brain surfaces; thoracic injuries by sternum and costal cartilage removal; abdominal organs weighed and sectioned. Histology of contusions (haemosiderin and siderophage appearance) can refine injury age estimates.
Medicolegal Inference: IPC Categorisation and Court Testimony
The forensic physician translates physical injury findings into a medico-legal opinion that maps onto the Indian Penal Code categories — this is the final step that gives the clinical findings their legal weight. Without this step, a perfectly documented post-mortem is of limited use to the prosecution or defence.
IPC Section 319 — Hurt: whoever causes bodily pain, disease, or infirmity to any person. No degree of severity required. Any injury documented by the forensic physician may constitute hurt.
IPC Section 320 — Grievous Hurt: eight categories specified, including: (1) emasculation; (2) permanent privation of sight of either eye; (3) permanent privation of hearing of either ear; (4) privation of any member or joint; (5) destruction/permanent impairing of powers of any member or joint; (6) permanent disfiguration of head or face; (7) fracture or dislocation of bone or tooth; (8) any hurt that endangers life or causes severe bodily pain for 20 days or more with inability to follow ordinary pursuits. The forensic physician must explicitly state whether a documented injury falls into any of these eight categories.
IPC Section 299 — Culpable Homicide: causing death by act done with the intention of causing death, or with the intention of causing such bodily injury as is likely to cause death, or with the knowledge that the act is likely to cause death. IPC Section 300 — Murder: culpable homicide becomes murder under four specified circumstances (knowledge that the act will in all probability cause death; intention to cause bodily injury known to be sufficient to cause death in the ordinary course of nature; intention to cause bodily injury and that injury is sufficient in the ordinary course of nature to cause death; act eminently dangerous to human life without excuse). For head injuries causing death, the forensic physician must express the opinion on: (a) whether the head injury was 'sufficient in the ordinary course of nature to cause death' — if yes, this grounds IPC 300 (murder); (b) whether death was the direct and proximate result of the injury or whether a pre-existing disease or medical intervention contributed.
Court testimony: the physician appears as an expert witness, whose function is to assist the court with technical knowledge — not to advocate for either side. Opinions must be stated in plain language, acknowledged as opinions rather than certainties, and their scientific basis explained. When cross-examined, acknowledge uncertainty honestly; do not overstate the precision of injury age estimates or range categories. The judge ultimately determines the legal categorisation based on the totality of evidence; the physician provides the medical facts and their scientific interpretation.
SELF-CHECK
A 45-year-old man is found dead with multiple injuries. One injury is described as: a 3 cm linear wound on the right temporal scalp with irregular margins, tissue bridges visible on cleaning, no sharp edges, and contusion of adjacent scalp. Which wound type is this, and what does the presence of tissue bridges indicate?
A. Incised wound from a sharp object; tissue bridges are artifactual and do not affect classification
B. Abrasion; the linear pattern indicates a tangential blunt force
C. Laceration from blunt force; tissue bridges across the wound confirm the tear was caused by blunt force, distinguishing it from an incised wound
D. Contact gunshot wound; the irregular margins and central blackening are characteristic
Reveal Answer
Answer: C. Laceration from blunt force; tissue bridges across the wound confirm the tear was caused by blunt force, distinguishing it from an incised wound
Tissue bridges — thin strands of dermis crossing the wound gap — are the key distinguishing feature of a laceration versus an incised wound. Lacerations result from blunt force tearing the skin; the dermis does not cut cleanly, leaving connective tissue strands bridging the wound margins. Incised wounds, produced by sharp-edged weapons, cut the dermis cleanly with no bridges. This distinction is critical in IPC injury categorisation and in inferring the type of weapon used.
Self-Assessment
Test your understanding with these self-check questions:
Q1. A 35-year-old man is struck on the left temporal region. Post-mortem shows left temporal scalp laceration, left temporal linear skull fracture, left temporal epidural haematoma (45 mL), and right frontal lobe contusion. Label each finding as coup or contre-coup and explain the mechanism for each.
Answer: Left temporal scalp laceration and linear fracture = coup (at site of impact). Left temporal EDH = coup complication (middle meningeal artery torn at the fracture site, same side as impact). Right frontal lobe contusion = contre-coup (brain inertially moves to the right when the head decelerates on the left, impacting the right side of the anterior cranial fossa). This combination — coup fracture + contre-coup brain contusion — is characteristic of a head struck by a moving object while the head is stationary.
Q2. Differentiate epidural from subdural haematoma on three criteria: source vessel, CT appearance, and the significance of the lucid interval.
Answer: EDH: source = middle meningeal artery (arterial, rapid); CT = biconvex lens-shaped, bounded by sutures; lucid interval = classic (arterial pressure drives rapid expansion after brief recovery). SDH: source = bridging veins (venous, slower in subacute/chronic); CT = crescent-shaped, follows brain contour, crosses sutures; lucid interval = not classical (acute SDH may deteriorate rapidly without lucid interval; chronic SDH presents with progressive decline over days-weeks).
Q3. List the eight categories of grievous hurt under IPC Section 320 and give one forensic injury finding that would place a case into each category.
Answer: (1) Emasculation — traumatic avulsion of the penis or testes; (2) Permanent privation of sight — optic nerve injury at orbital apex or cortical visual area injury with permanent blindness; (3) Permanent privation of hearing — temporal bone fracture with cochlear disruption; (4) Privation of any member or joint — traumatic amputation; (5) Destruction/permanent impairing of powers of any member or joint — severe brachial plexus injury causing permanent paralysis; (6) Permanent disfiguration of head or face — extensive acid burns, keloid scarring, or facial bone comminution; (7) Fracture or dislocation of bone or tooth — any documented fracture on X-ray, including tooth root fracture; (8) Hurt endangering life or causing severe bodily pain for ≥20 days — penetrating abdominal wound with bowel perforation and peritonitis.