Page 4 of 9
FM12.3 | Cyber Forensics & Privacy of Medical Documents — SDL Guide
Learning Objectives
- Define cyber forensics and describe its application in the context of medical records and electronic health information (FM12.3)
- Explain the legal framework governing electronic records in India, including the Information Technology Act 2000 (amended 2008) and the Section 65B certificate requirement for admissibility
- Describe how electronic medical records are examined for authenticity, alteration, and chain of custody
- Apply the legal principles governing privacy of medical documents — ownership, retention, disclosure, and the consequences of unauthorised disclosure
- Identify the circumstances under which medical records may and must be disclosed
INSTRUCTIONS
The digital transformation of medical records has created a new frontier in forensic medicine: cases involving disputed clinical records, tampered laboratory reports, forged prescriptions, and unauthorised disclosure of patient data are now reaching courts. As a future clinician, you will maintain electronic health records throughout your career. Understanding the legal status of those records — how they can be authenticated, what protects them from tampering, when their disclosure is mandated vs prohibited, and how forensic analysis is applied to electronic documents — is essential both for practising lawfully and for participating in the legal processes that depend on medical documentation.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A medical negligence case reaches court. The plaintiff claims the hospital altered the patient's clinical records after the adverse event to conceal the error. The hospital produces the electronic medical record (EMR) from their hospital management software, showing the record was entered on the day of the event. The plaintiff's legal team questions: was the entry made at the stated time, or was it backdated? Was the record modified after the event? The answer lies in cyber forensics — the analysis of metadata, access logs, hash verification, and digital audit trails in the EMR system. The forensic medical officer must understand how to examine this evidence, how to authenticate it, and how to present it under the Section 65B certificate framework that governs electronic records in Indian courts.
WHY THIS MATTERS
Within the next decade, virtually all clinical documentation will be electronic — EMRs, e-prescriptions, digital imaging (DICOM files for radiology and pathology), telemedicine consultations, and wearable device data. Every one of these is a potential forensic exhibit. As a clinician, you are simultaneously the creator, custodian, and subject of medical records. You create records that may be subpoenaed, tampered with, or scrutinised for authenticity years later. You have legal obligations to maintain their confidentiality and to produce them lawfully on demand. Understanding cyber forensics in the medical context protects your patients, protects you professionally, and ensures that justice is served when medical records enter the legal arena.
RECALL
From earlier Forensic Medicine sessions, recall:
- Doctor-patient confidentiality — the obligation to protect patient information from unauthorised disclosure; this obligation persists even after the patient's death in most circumstances.
- Circumstances of lawful disclosure — police requisition, court order, notifiable disease reporting, public safety — situations where disclosure is legally permitted or mandated despite the general confidentiality obligation.
- Medicolegal report standards (from lab2-professionalism) — the documentation principles that apply equally to electronic reports: accuracy, completeness, objectivity, clear distinction of findings from opinion.
- Chain of custody — the principle that the integrity of an exhibit must be demonstrable from collection to court. For a physical biological specimen, this involves sealed containers and signature logs. For a digital exhibit, the equivalent is metadata, hash values, and audit trails.
The Medicolegal Significance of Electronic Medical Records
Electronic medical records (EMRs) have become central to medicolegal proceedings across a wide range of case types — medical negligence, criminal investigations, insurance disputes, employment cases, and professional conduct hearings. Their significance as forensic evidence derives from three properties that they share with physical exhibits: they contain information relevant to legal questions, they can be authenticated (or their authenticity challenged), and they can be subjected to forensic analysis to detect alteration, tampering, or unauthorised access.

Provided image
The categories of medicolegal scenario in which EMR forensics becomes critical include:
• Medical negligence litigation: One of the most common uses — was the clinical record created contemporaneously with the events it documents, or was it backdated after the adverse outcome? Were entries modified, added, or deleted after the date shown? In clinical negligence, the timing and completeness of documentation can be outcome-determinative.
• Criminal investigations involving healthcare workers: Cases of deliberate patient harm (poisoning by a healthcare worker, fraudulent certification), criminal abortion, insurance fraud using falsified clinical records, and registration fraud using altered qualifications all involve electronic records that may have been created or modified for criminal purposes.
• Drug prescription fraud: Electronic prescriptions, e-stamps, and prescription database systems can be forensically examined to detect forgery, duplication, and unauthorised prescription generation.
• Telemedicine and digital consultation disputes: As telemedicine expands, disputes about what advice was given, when, and to whom will increasingly rely on electronic communication records — emails, chat logs, video consultation recordings, and audio files.
• Wearable and IoT medical data: Data from implanted cardiac devices, glucometers, wearable pulse oximeters, and activity monitors can be relevant in personal injury claims, insurance disputes, and criminal investigations. This data constitutes electronic medical records under the broad IT Act definition.
In each of these scenarios, the forensic medical officer must understand not only the clinical content of the record but also its technical provenance — where it was created, by whom, at what time, and whether it has been modified since creation. These questions are answered by cyber forensics, the branch of forensic science that analyses digital evidence.
Scientific and Legal Basis of Cyber Forensics in Medicine
Cyber forensics (also called digital forensics) is the application of scientific methods to identify, preserve, examine, and present digital evidence in a form that is legally admissible. In the medical context, the digital evidence of interest includes: EMR entries and their modification history, DICOM imaging files, laboratory information system (LIS) records, pharmacy dispensing records, electronic prescriptions, hospital management system (HMS) access logs, and communications (email, messaging) between healthcare workers.
The scientific basis of cyber forensics rests on two foundational concepts:
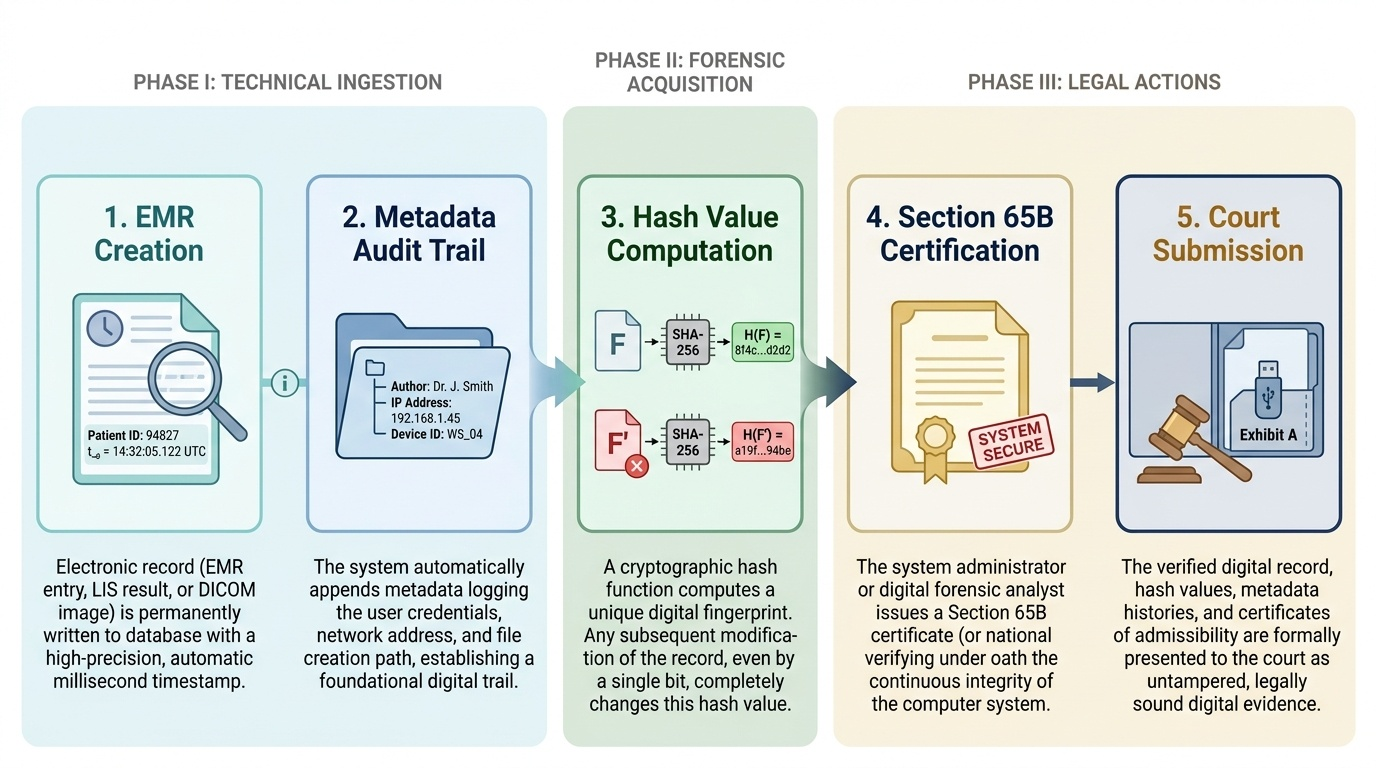
1. Metadata — the 'data about the data':
Every digital file contains metadata — information recorded automatically by the creating system about the file's properties. For a document or EMR entry, this includes: creation date and time (with timestamp precision to the second or millisecond), last-modified date and time, the user account under which the entry was made, the computer's IP address, and sometimes the geographic location of the creating device. Critically, metadata is not easily falsified without specialised tools, and forensic examination can often detect metadata manipulation because the file's internal metadata and the filesystem's metadata may not be consistent after tampering. In the medical negligence scenario from the hook, metadata examination might reveal that an EMR entry dated on the day of the adverse event was actually last modified two days later — consistent with backdating.
2. Hash verification — the digital fingerprint:
A cryptographic hash function (such as MD5, SHA-1, or SHA-256) generates a fixed-length string ('hash value' or 'checksum') from an input file. The critical property is that even a single-bit change in the file produces a completely different hash value — this is called the avalanche effect. By computing and recording the hash value of a digital file at the time of lawful acquisition (e.g. when the hospital is ordered to produce records for court), and verifying that the hash remains unchanged when the file is later examined or presented in evidence, forensic examiners can prove — or disprove — that the file has been modified in transit.
Provided image
The legal framework — Information Technology Act 2000 (IT Act) and Section 65B:
The Information Technology Act 2000 (amended significantly in 2008) is India's primary legislation governing electronic records, electronic contracts, digital signatures, and cybercrimes. For the forensic medical context, the most important provisions are:
• Section 43: penalties for unauthorised access to, damage to, or downloading of computer system data — directly applicable to unauthorised access to EMR systems
• Section 66: computer-related offences (criminal forms of Section 43 acts) — applicable to deliberate data theft or destruction of medical records
• Section 66E: violation of privacy by capturing or publishing private images without consent — relevant to unauthorised sharing of patient images or case photographs
• Section 72A: disclosure of information in breach of lawful contract — applicable to healthcare data breaches
However, the most practically significant legal provision for medical record admissibility is Section 65B of the Indian Evidence Act, 1872 (not the IT Act itself, but cross-referenced through IT Act provisions). Section 65B governs the admissibility of computer-generated electronic records in court. A printout or other output from a computer (including an EMR) is admissible as evidence only if:
1. The computer was used regularly to store or process information of the kind in the printout
2. The computer was functioning properly at the relevant time
3. The information was supplied in the ordinary course of activities
4. A Section 65B certificate is provided — a formal declaration from the person responsible for the computer confirming the above conditions and attesting to the authenticity of the output
Without a valid Section 65B certificate, a printout of an EMR is not admissible as primary electronic evidence — it may only be admitted as secondary evidence with additional corroboration. The Supreme Court reaffirmed this requirement in Arjun Panditrao Khotkar v Kailash Kushanrao Gorantyal (2020), holding that the Section 65B certificate is mandatory, not optional, for electronic evidence admissibility.
SELF-CHECK
A hospital is ordered by a court to produce a patient's electronic medical record as evidence in a negligence case. The hospital prints out the record and submits it. Under Indian evidence law, what is required for this printout to be admissible as primary electronic evidence?
A. The printout must be certified by the hospital's Chief Medical Officer
B. The printout must be accompanied by a Section 65B certificate from the person responsible for the computer system, attesting to the record's authenticity and the computer's proper functioning
C. The printout automatically becomes admissible once produced by a government hospital
D. A notarised copy of the printout is sufficient for admissibility
Reveal Answer
Answer: B. The printout must be accompanied by a Section 65B certificate from the person responsible for the computer system, attesting to the record's authenticity and the computer's proper functioning
Under Section 65B of the Indian Evidence Act, a computer-generated output (including an EMR printout) is admissible as primary electronic evidence only when accompanied by a Section 65B certificate from the person responsible for the computer system. The certificate must attest that the computer was used regularly for that type of information, was functioning properly, that the information was supplied in the ordinary course of activities, and that the output is a true representation of the original data. The Supreme Court in Arjun Panditrao Khotkar v Kailash Kushanrao Gorantyal (2020) confirmed this certificate is mandatory. The CMO's certification (option A) is not the specific legal requirement; the certificate must come from the person responsible for the computer — typically the IT head or system administrator. Government hospital status (option C) does not create a presumption of admissibility. Notarisation (option D) is not the same as a Section 65B certificate.
Examining and Documenting Digital Evidence
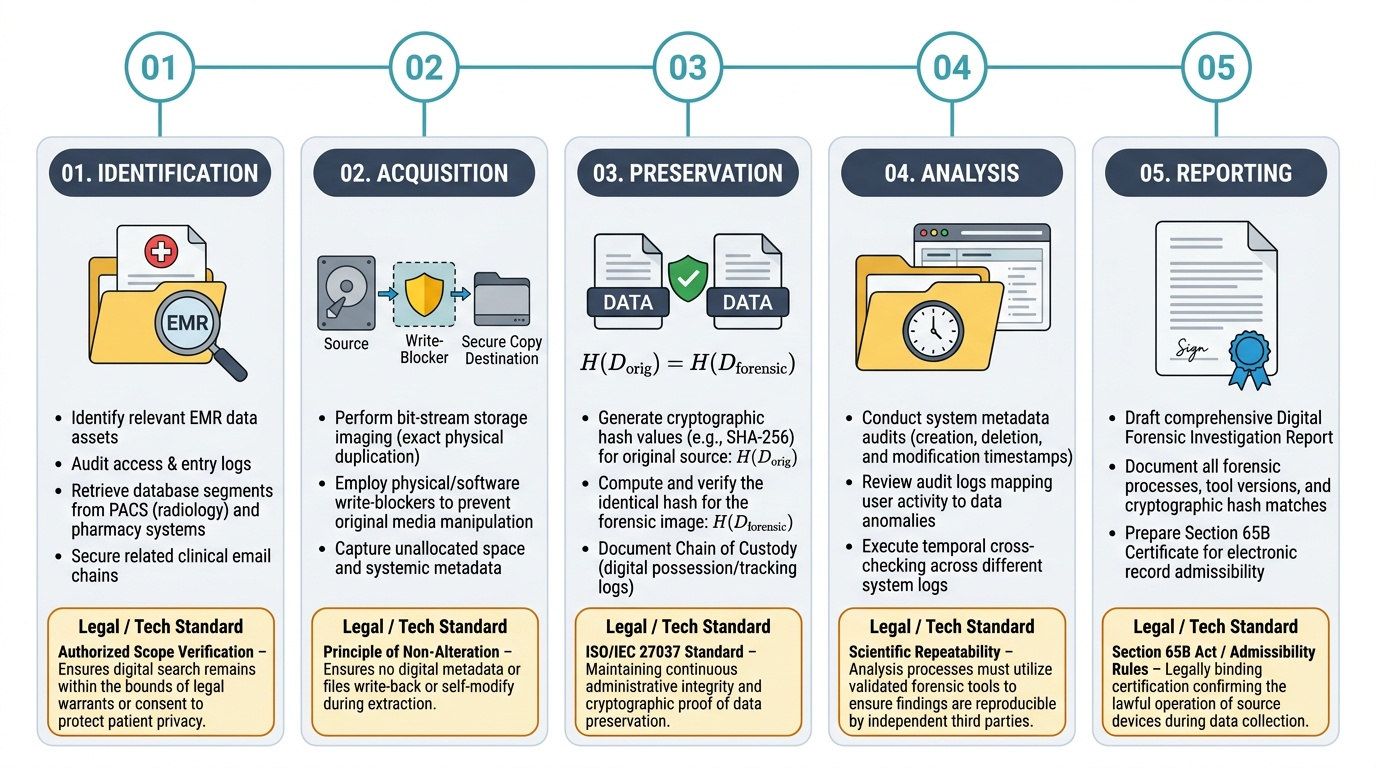
The forensic examination of digital medical evidence follows a process analogous to physical evidence collection: identification → acquisition → preservation → analysis → reporting. Each stage has specific technical and legal requirements that must be met for the evidence to remain admissible.
Provided image
Identification of relevant digital evidence requires the forensic examiner to determine which digital assets are relevant to the investigation. In a medical context, this may include: the EMR system's entry log for a specific patient, the access log showing which user accounts viewed or modified the record, the imaging system (PACS — Picture Archiving and Communication System) for radiology files, the pharmacy system's dispensing records, and email communications between clinical staff about the case.
Acquisition and preservation — bit-stream imaging:
The gold standard for digital evidence preservation is the creation of a bit-stream forensic image — an exact, bit-for-bit copy of the original storage medium (hard drive, server partition, or database dump). This is distinct from a file copy, which does not preserve deleted files, unallocated space, or metadata associated with the filesystem. The forensic image is taken using specialised write-blocker hardware that prevents any data from being written to the original medium during copying, thereby preserving its original state. Hash values are computed for the original medium and the forensic image immediately after imaging; if the hashes match, the image is verified as an exact copy.
Chain of custody for digital exhibits follows the same documentation principle as physical evidence — a continuous signed record of who had possession of the storage medium or forensic image, when, and in what condition. Unlike physical exhibits, digital evidence can be transmitted electronically, and the chain of custody must account for every transmission, storage, and access event. The hash value serves as the electronic equivalent of the wax seal — if the hash of the file on receipt matches the hash at acquisition, the file has not been altered in transit.
Common indicators of EMR tampering that a forensic examination may reveal:
• Timestamp inconsistency: The claimed entry date in the medical record is earlier than the software installation date or earlier than the patient's first registration in the system.
• Metadata-record mismatch: The file's modification timestamp shows a later date than the date stated in the entry — consistent with post-event modification.
• Audit log deletion: Hospital EMR systems maintain automatic audit logs of every access and modification. A record that shows no audit trail for a claimed modification period is suspicious.
• Formatting anachronism: The record uses formatting conventions or software version features that did not exist at the claimed date of creation.
• Authorship attribution error: The logged user account making a specific entry is shown by audit logs to have been simultaneously active on a different ward or in a different session.
The findings from digital forensic examination are documented in a formal digital forensic report, which must meet the same professional standards as any medicolegal report: structured format, factual findings clearly separated from opinion, and an opinion section with probability language and stated limitations.
SELF-CHECK
A forensic examiner acquires a bit-stream image of a hospital server's patient records database. To verify that the forensic image is an exact copy of the original, the examiner should:
A. Compare the file sizes of the original and the image
B. Have the hospital's IT department certify that the copy is accurate
C. Compute cryptographic hash values (e.g. MD5 or SHA-256) of both the original and the image and confirm they are identical
D. Randomly check 10% of the records in the image against the original
Reveal Answer
Answer: C. Compute cryptographic hash values (e.g. MD5 or SHA-256) of both the original and the image and confirm they are identical
Cryptographic hash values provide definitive verification of digital evidence integrity. A hash function produces a unique fixed-length string ('fingerprint') from a file or storage volume; even a single-bit change produces a completely different hash. If the hash of the forensic image matches the hash of the original medium computed immediately after acquisition, the image is a verified exact copy. File size comparison (option A) is insufficient — two files can have the same size with different content. IT department certification (option B) is procedurally relevant for the Section 65B certificate but does not technically verify the copy's bit-level accuracy. Random sampling (option D) can miss alterations in the unsampled 90%.
Privacy of Medical Documents — Legal Framework, Obligations & Violations
The privacy of medical records is governed in India by an intersecting framework of statutes, judicial pronouncements, and professional regulations. No single comprehensive medical privacy statute equivalent to the US HIPAA exists, but the combined effect of the Information Technology Act 2000 (IT Act, amended 2008), the Information Technology (Reasonable Security Practices and Procedures and Sensitive Personal Data or Information) Rules 2011, the common law doctrine of medical confidentiality, and theConsumer Protection Act 2019 creates substantial legal protection for electronic health information.
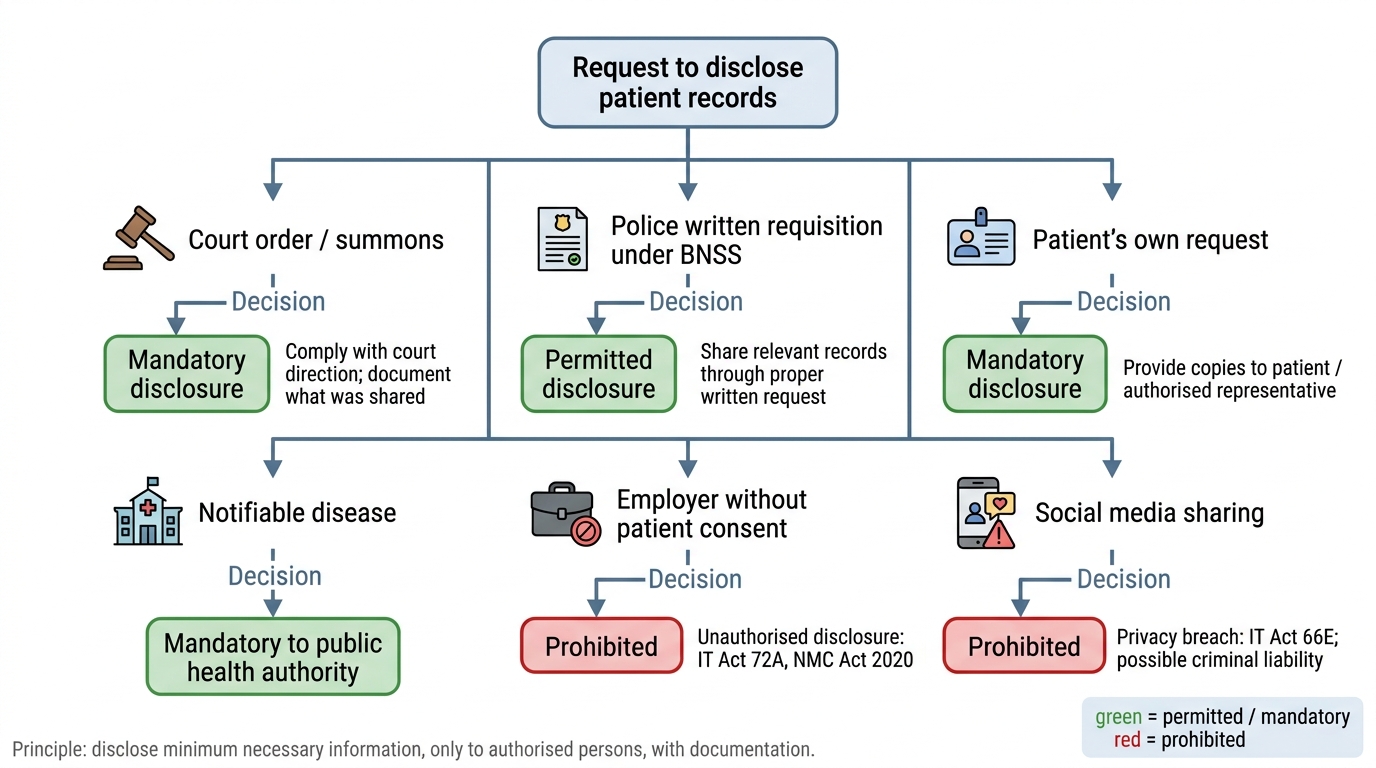
Decision Flowchart for Disclosure of Patient Medical Records
Ownership, custody, and access:
In Indian law, medical records are generally held to be the property of the institution that creates them (hospital or clinic), but the patient has a fundamental right to access and obtain copies of their own records. This right was affirmed by the Supreme Court in multiple rulings and is enshrined in the Medical Records Rules under the Clinical Establishments Act. A hospital cannot refuse to provide a patient (or, after death, their legal heirs) copies of their medical records without a lawful justification. Unjustified refusal may constitute:
• Deficiency of service under the Consumer Protection Act 2019 (note: the 1986 Act was repealed; always cite the 2019 Act)
• Obstruction of justice if records are suppressed in contemplation of legal proceedings
• Potential contempt of court if records are withheld after a court order for production
Retention requirements:
Medical records must be retained for a defined minimum period. Under CGHS (Central Government Health Scheme) guidelines, outpatient records must be retained for 3 years; inpatient records for 3-5 years. The Medical Council of India (now superseded by NMC under the NMC Act 2020) had advised 3 years as a minimum, but hospitals handling complex or high-risk cases routinely retain records for longer periods. Electronic records have no physical storage constraint, so retention periods are typically set by institutional policy in compliance with the minimum legal requirements.
Permitted disclosure (lawful exceptions to confidentiality):
The general obligation of medical confidentiality yields to disclosure in the following circumstances:
• Court order or summons — production of records in compliance with a court order is mandatory; refusal constitutes contempt.
• Police requisition under BNSS — a registered medical practitioner must produce records relevant to a criminal investigation under lawful requisition. However, a mere verbal request is insufficient; a formal written requisition from a competent officer is required.
• Notifiable disease reporting — certain communicable diseases require statutory notification to public health authorities.
• Public safety — a serious and specific threat to an identifiable third party may justify disclosure to prevent imminent harm (this is a narrow common law exception; not a broad licence for disclosure).
• Patient's own consent — explicit informed consent from the patient for disclosure to specified parties.
Prohibited disclosures and their consequences:
Unauthorised disclosure of a patient's medical records — whether by sharing with family members without consent, providing information to employers, or posting clinical images on social media — may constitute:
• Breach of contract (doctor-patient confidentiality as an implied contractual term)
• Violation of Section 72A of the IT Act 2000 (disclosure of information in breach of lawful contract)
• Violation of Section 66E (capturing or publishing private images without consent) if clinical images are involved
• Professional misconduct under the NMC Act 2020, potentially leading to suspension or erasure from the medical register
• Deficiency of service under the Consumer Protection Act 2019
| Disclosure Scenario | Permitted? | Legal Basis | Consequence of Improper Action |
|---|---|---|---|
| Court order/summons | Mandatory | CrPC/BNSS; Indian Evidence Act | Contempt of court if refused |
| Police written requisition | Permitted (with formal requisition) | BNSS Section 176 | Obstruction of justice if withheld |
| Patient's own request | Mandatory | Consumer Protection Act 2019; right to access | Deficiency of service if refused |
| Employer's request (without patient consent) | Prohibited | IT Act 2000, NMC Act 2020 | Professional misconduct |
| Social media sharing of patient images | Prohibited | IT Act 2000 Section 66E | Criminal liability + professional sanction |
| Research (without ethical approval and consent) | Prohibited | NMC ethics guidelines; ICMR guidelines | Institutional and professional sanction |
SELF-CHECK
A patient's employer contacts the hospital requesting the patient's blood test results without the patient's knowledge. The hospital shares the results to maintain a 'good relationship' with the employer. Under Indian law, this action by the hospital most likely constitutes:
A. A lawful disclosure because the employer has a legitimate interest in the employee's health
B. A violation of medical confidentiality and potentially Section 72A of the IT Act 2000, which prohibits disclosure of information in breach of a lawful contract
C. A permitted disclosure under the Consumer Protection Act 2019
D. A lawful disclosure if the test was a pre-employment medical examination
Reveal Answer
Answer: B. A violation of medical confidentiality and potentially Section 72A of the IT Act 2000, which prohibits disclosure of information in breach of a lawful contract
Sharing a patient's medical records with their employer without the patient's explicit consent is an unauthorised disclosure. The doctor-patient relationship creates an obligation of confidentiality that has contractual force, and disclosure to a third party without consent violates it. Section 72A of the IT Act 2000 specifically penalises disclosure of personal information in breach of a lawful contract, and the doctor-patient confidentiality obligation has been recognised as such a contract. This action could also constitute professional misconduct under the NMC Act 2020. Option A is incorrect — an employer's general interest in an employee's health does not constitute a lawful exception to medical confidentiality. Option C is incorrect — the Consumer Protection Act 2019 protects the patient's right of access, not the employer's. Option D is incorrect — even for pre-employment examinations, the results belong to the patient unless the employment contract specifically provides otherwise and the patient has consented.
CLINICAL PEARL
The Section 65B certificate — the most commonly forgotten step: In India, nearly every medicolegal dispute involving electronic records ultimately requires a Section 65B certificate. Courts routinely reject electronic evidence without it. As a future clinician who will generate and manage digital records, you must know: if you are ever asked to produce electronic records as evidence, the legal officer of your institution must provide a Section 65B certificate from the person responsible for the computer system alongside the records. A plain printout of an EMR — without this certificate — is technically inadmissible as primary electronic evidence. This is not a technicality that courts overlook — the Supreme Court in Arjun Panditrao Khotkar (2020) expressly held it is mandatory. Ensure your institution's IT and legal departments understand this requirement.
KEY TAKEAWAYS
FM12.3 covers two interlinked domains:
Cyber forensics in medical practice:
• Digital evidence includes EMRs, imaging files, pharmacy records, access logs, and electronic communications
• Forensic examination uses metadata analysis, hash verification (MD5/SHA-256), bit-stream imaging, and audit-log review
• Common evidence of EMR tampering: timestamp inconsistencies, metadata-record mismatch, audit log deletion, formatting anachronisms
• Chain of custody for digital exhibits: hash value = electronic equivalent of a wax seal
Legal framework for electronic records:
• IT Act 2000 (amended 2008): governs electronic records, unauthorised access (Section 43), computer offences (Section 66), privacy violations (Section 66E), data disclosure in breach (Section 72A)
• Section 65B Indian Evidence Act: electronic records admissible only with a Section 65B certificate from the person responsible for the computer — mandatory, not optional (Arjun Panditrao Khotkar v Kailash Kushanrao Gorantyal, 2020)
Privacy of medical documents:
• Medical records: institutional property, but patient has a right of access
• Retention: minimum 3 years (CGHS); 3-5 years typically for inpatient records
• Lawful disclosures: court order, police written requisition (BNSS), notifiable disease reporting, public safety, patient consent
• Prohibited disclosures: employer without patient consent, social media posting (Section 66E IT Act), research without ethical approval
• Consequences of improper disclosure: IT Act criminal liability, Consumer Protection Act 2019 deficiency, NMC Act 2020 professional misconduct
REFLECT
Consider these scenarios and reflect on your obligations:
- You are the registrar in a hospital. The police arrive asking for the complete medical records of a patient who is a suspect in a murder investigation. They say it is urgent and verbal authority should be enough. What do you do, and what legal authority are you looking for before producing the records?
- A patient was treated for a drug overdose in your emergency department. His employer calls, identifies himself, and says he needs to know the test results for 'safety reasons.' How do you respond, and what legal provisions support your response?
- You discover that a junior colleague took a photograph of a patient's unusual skin lesion on their personal smartphone and posted it on a medical education social media group (with the face partially obscured but the room and name tag visible in the background). What are the potential legal consequences, and what should you advise?
- Your hospital is asked to produce a patient's EMR as evidence in a medical negligence case. The printout is ready. What additional document must accompany it for it to be admissible as primary electronic evidence in the Indian court?