Page 2 of 9
FM12.4-5 | Professionalism in Trace-Evidence Handling & Reporting — SDL Guide
Learning Objectives
- Demonstrate professional standards when sending biological and trace evidence to the FSL, including specifying required tests and objectives of preservation (FM12.4)
- Explain how to interpret FSL findings and discuss them in the context of the medicolegal case (FM12.4)
- Prepare a medicolegal report that documents examination findings, collection/preservation/dispatch of evidence, interpretation, and a defensible opinion/inference (FM12.5)
- Distinguish between factual findings and opinion/inference in a medicolegal report
- Apply the principle that the forensic medical officer's duty runs to the court, not to the referring party
INSTRUCTIONS
The forensic medical officer's greatest professional test lies not in the laboratory but in the report. A forensic examination is only as valuable as the documentation produced from it. A report that confuses findings with opinion, omits critical negative findings, or uses ambiguous language can be dismantled in cross-examination and may result in a miscarriage of justice. This module teaches the professional standards that govern both the submission of evidence to the FSL and the production of medicolegal reports — from the covering letter that directs laboratory analysis to the opinion paragraph that a judge may read from the bench.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 19-year-old sexual assault survivor presents at a government hospital. The attending doctor examines her, collects swabs, and prepares the Sexual Assault Examination Report (SAER). But when the case comes to trial, the defence counsel cross-examines the doctor: "Did you record whether the patient reported the incident voluntarily?" "Did your report distinguish between the findings and your opinion?" "Your letter to the FSL requested general STI testing — did you specifically request DNA profiling of the swabs?" The doctor answers uncertainly. The cross-examination erodes the report's credibility. The case becomes difficult to prosecute — not because the examination was wrong, but because the documentation and FSL submission did not meet professional standards. This module ensures you never face that cross-examination unprepared.
WHY THIS MATTERS
Every forensic medical report you produce during your career may one day be read in a courtroom. The standard is not your comfort with language or report writing — it is the court's standard of admissible, unambiguous, objective documentation. This matters in both criminal proceedings (where your report may help convict or exonerate a person) and civil/quasi-judicial matters (insurance disputes, disability claims, professional negligence panels). Understanding how to write a professional report also protects you: a well-documented, clearly structured, opinion-separate-from-findings report is the best defence against allegations of bias or incompetence. Professionalism in forensic medicine is simultaneously a service to justice and a form of professional self-protection.
RECALL
Before exploring professional standards, recall the foundational knowledge from earlier in this cluster:
- Chain of custody principles (from lab1-specimens): the continuous documented record of specimen possession — how it applies when transferring specimens to the FSL.
- Specimen labelling requirements: case number, exhibit number, specimen type, date/time, collector's signature, investigating officer counter-signature, wax seal.
- The distinction between a witness of fact (who testifies to what they personally observed) and an expert witness (who gives an opinion based on their professional expertise in a specialised field) — the forensic medical officer typically functions as an expert witness.
- The role of the FSL Director as the head of the institution that receives, processes, and reports on forensic evidence submitted by investigators.
Legal and Professional Context of Forensic Medical Practice
The forensic medical officer occupies a unique position in the Indian legal system: they are simultaneously a licensed medical practitioner bound by professional ethics and a quasi-judicial functionary bound by obligations to the court. Understanding this dual role is the starting point for all professional conduct in forensic practice. When a forensic medical officer examines a victim of crime, conducts an autopsy, or handles biological evidence, their primary obligation in the medico-legal context runs to the court and to justice — not to the police, the prosecution, the defence, or the patient in the ordinary clinical sense.
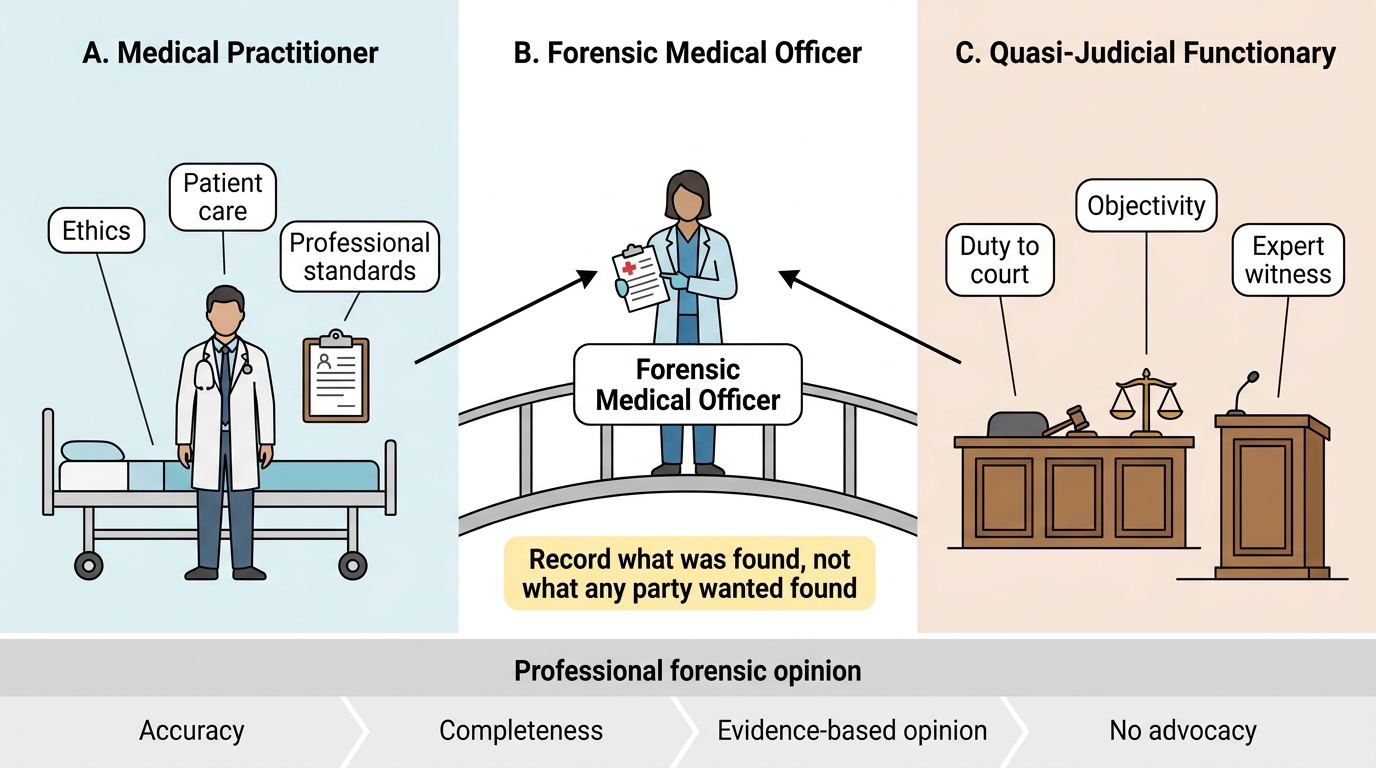
Dual Role of the Forensic Medical Officer
This principle is operationalised in Indian law through the provisions governing expert evidence under the Indian Evidence Act. An expert witness is a person specially skilled in a particular science, art, trade, or technical matter, whose opinion the court may take into account. The forensic medical officer giving evidence about the cause of death, the nature of injuries, or the interpretation of toxicology results is functioning as an expert witness. This carries a professional obligation to express only those opinions that can be defended on the basis of medical knowledge and examination findings — not speculation, not advocacy, and not conclusions that overreach the evidence.
Professionalism in this context encompasses four non-negotiable attributes:
• Accuracy — findings recorded exactly as observed, with precise anatomical descriptions and measurements
• Completeness — all relevant positive AND negative findings must be documented; the absence of an expected finding (e.g. no evidence of injury) is as medically significant as its presence
• Objectivity — the report's conclusions must be the same regardless of which party requested the examination
• Reproducibility — another competent forensic medical officer reviewing the same examination findings should reach the same or a reconcilable opinion
The legal framework governing forensic medical practice in India includes the provisions of the Code of Criminal Procedure (CrPC) (now largely superseded by the Bharatiya Nagarik Suraksha Sanhita, BNSS 2023) on medical examination of persons arrested, the Indian Evidence Act on expert testimony, and specific legislation such as the POCSO Act 2012 for child victims and the Protection of Women from Domestic Violence Act 2005 for domestic violence cases. The forensic medical officer must be aware of which legislative framework applies to the case at hand, as it determines the examination protocol and the format of required documentation.
SELF-CHECK
A forensic medical officer is examining an alleged sexual assault survivor. The investigating police officer requests that the report be written to support the victim's account. The correct professional response is to:
A. Comply, as the police officer has investigative authority over the case
B. Decline and write an objective report documenting only examination findings and a defensible opinion, because the duty runs to the court
C. Consult with the victim before finalising the report to ensure it reflects her experience
D. Refer the case to a senior forensic medical officer to avoid conflict with the police
Reveal Answer
Answer: B. Decline and write an objective report documenting only examination findings and a defensible opinion, because the duty runs to the court
The forensic medical officer's professional duty in the medicolegal context runs to the court and to justice — not to the police, prosecution, or patient in the clinical sense. The report must record findings objectively and express only defensible medical opinions. Complying with a request to write a biased report (option A) is professional misconduct. Consulting the victim for report content (option C) conflates history-taking with report finalisation — the victim's account is the history; the report is based on findings. Referral (option D) does not resolve the professional obligation to be objective.
Governing Principles for FSL Submissions — Specifying Tests and Objectives
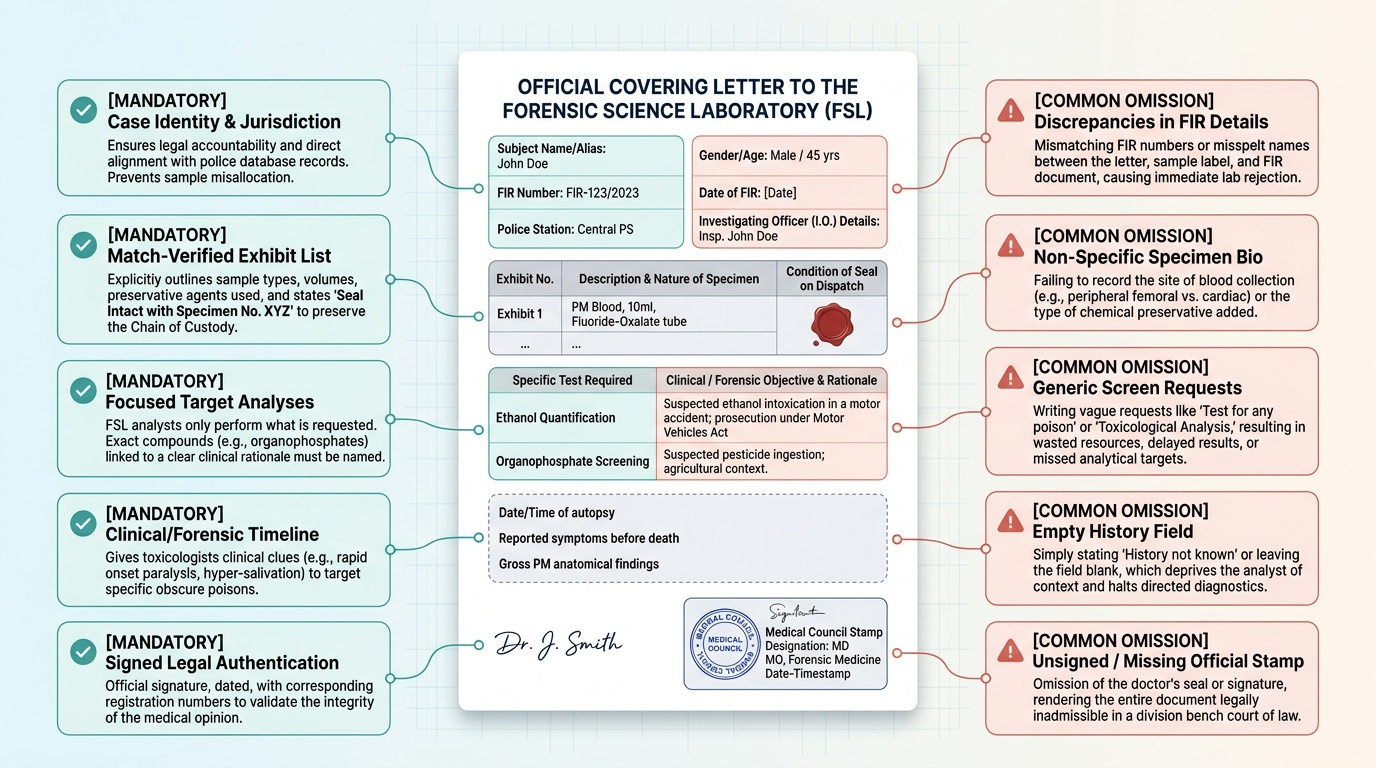
The covering letter accompanying specimens dispatched to the FSL is not a formality — it is the scientific and legal interface between the examining doctor and the analyst. A poorly written covering letter leads to an incomplete or misdirected analysis; the analyst can only test what they are asked to test, or apply a general screening panel if no specific tests are requested. The result is either unnecessary expenditure of time and resources on irrelevant tests, or — more critically — a missed analysis that should have been the primary inquiry.
Provided image
The covering letter must contain the following elements, in a structured format that mirrors the exhibit list:
1. Case particulars and legal reference:
Full name and description of the subject (deceased or living), FIR number, date of FIR, police station name, and investigating officer details. This identifies the legal case to which the exhibits belong and prevents mix-up with other cases.
2. Exhibit list with specimen details:
A numbered list of every exhibit being dispatched, with its exhibit number, nature of specimen (e.g. "Exhibit 1: Blood — left femoral vein, post-mortem, 10 mL, fluoride-oxalate tube, wax-sealed"), and the condition of the wax seal at dispatch. This establishes the baseline condition of each exhibit.
3. Specific tests requested and the clinical/forensic rationale:
This is the most professionally critical element. The forensic medical officer must specify:
• The EXACT tests required — not "general toxicology" but "screening for organophosphate compounds and quantification if positive" or "ABO and Rh blood grouping + DNA profiling" as appropriate
• The OBJECTIVE of each test — why this specimen, why this assay. For example: "Blood from femoral vein for ethanol quantification — suspected alcohol-related road accident; result required for Motor Vehicles Act proceedings"
• Any PREVIOUS results relevant to interpretation — if ante-mortem blood alcohol from a hospital was 160 mg/100 mL, the FSL analyst should know this when interpreting the post-mortem visceral alcohol
4. Brief relevant case history:
A concise factual narrative: circumstances of death or injury, time of discovery, relevant medical history, suspected cause, and what the investigation is trying to determine. This context is essential for the analyst to choose the appropriate detection method and interpret findings in context. An analyst who knows the case is a suspected paracetamol overdose will prioritise hepatic and blood paracetamol/NAPQI assay and check for N-acetylcysteine administration; without this history they may run a general screen and report "paracetamol detected at therapeutic levels" without recognising the significance of the exact concentration.
The principle of specificity in FSL submissions reflects a broader professional standard: the forensic medical officer must be the expert guide to the analysis, not merely a conduit for delivering boxes of specimens.
| Covering Letter Element | Required Content | Common Omission Error |
|---|---|---|
| Legal reference | FIR No., PS name, IO name | Missing FIR number |
| Exhibit list | Number, nature, container, seal status | Unlabelled or unnumbered exhibits |
| Specific tests | Named assays + indication | "General toxicology" without direction |
| Objectives | Why this test matters legally | Failing to state Motor Vehicles Act / POCSO context |
| Case history | Circumstances, time, suspicion | No history provided |
Method and Documentation for Medicolegal Reports
A medicolegal (ML) report is a formal medical document produced in response to a requisition from a legal authority (police, court, magistrate) and intended for use in legal proceedings. It differs from a clinical discharge summary or referral letter in one critical respect: it must function as a standalone document that can be understood by a non-medical reader (a judge or magistrate) while also withstanding expert cross-examination by a forensic medical specialist. Writing such a document requires deliberate structure and precise language.
The canonical structure of a medicolegal report follows these sections:
Heading and identification: Name of the doctor, qualifications, designation, institution; name and description of the subject; requisition authority (police station, case number, court order); date and time of examination.
History: The account provided by the subject or informant, recorded verbatim or in close paraphrase, with a statement of who provided the history. Critical: the history is the account given TO the doctor, not the doctor's assessment of its accuracy. Do NOT conflate the history with findings.
General examination: Vital signs (if living), general appearance, cooperative or non-cooperative, conscious level, apparent age, nutritional status, signs of intoxication, clothing description and condition. In post-mortem examination: body identification, estimated post-mortem interval, state of preservation.
Systematic/specific examination: A structured, anatomically sequenced record of examination findings. In a wound examination, this means: site (anatomical location and measurements), dimensions (length × breadth × depth), margins, edges, base, surrounding tissues, and direction of force. Each wound or finding must be described in a separate, numbered paragraph. In a sexual assault examination, the genitalia, perianal region, and other sites of injury are described using standardised terminology from the national protocol.
Investigations: Results of specimens collected — blood type, toxicology screens, swabs, radiographs. State the specimens collected, how they were preserved and sealed, and the exhibit numbers assigned.
Opinion/Conclusion: This is the most legally significant section. The opinion must:
• Be clearly labelled as opinion, separated from factual findings
• Be expressed in measured, probabilistic language ("consistent with", "could have been caused by", "in my opinion", not "definitely caused by" unless certainty is justified)
• State the basis for the opinion in the findings
• Include relevant limitations ("Opinion is based on the examination findings alone; DNA and toxicology results not yet available")
Signature, date, and counter-signature of a senior colleague if required by the institution.
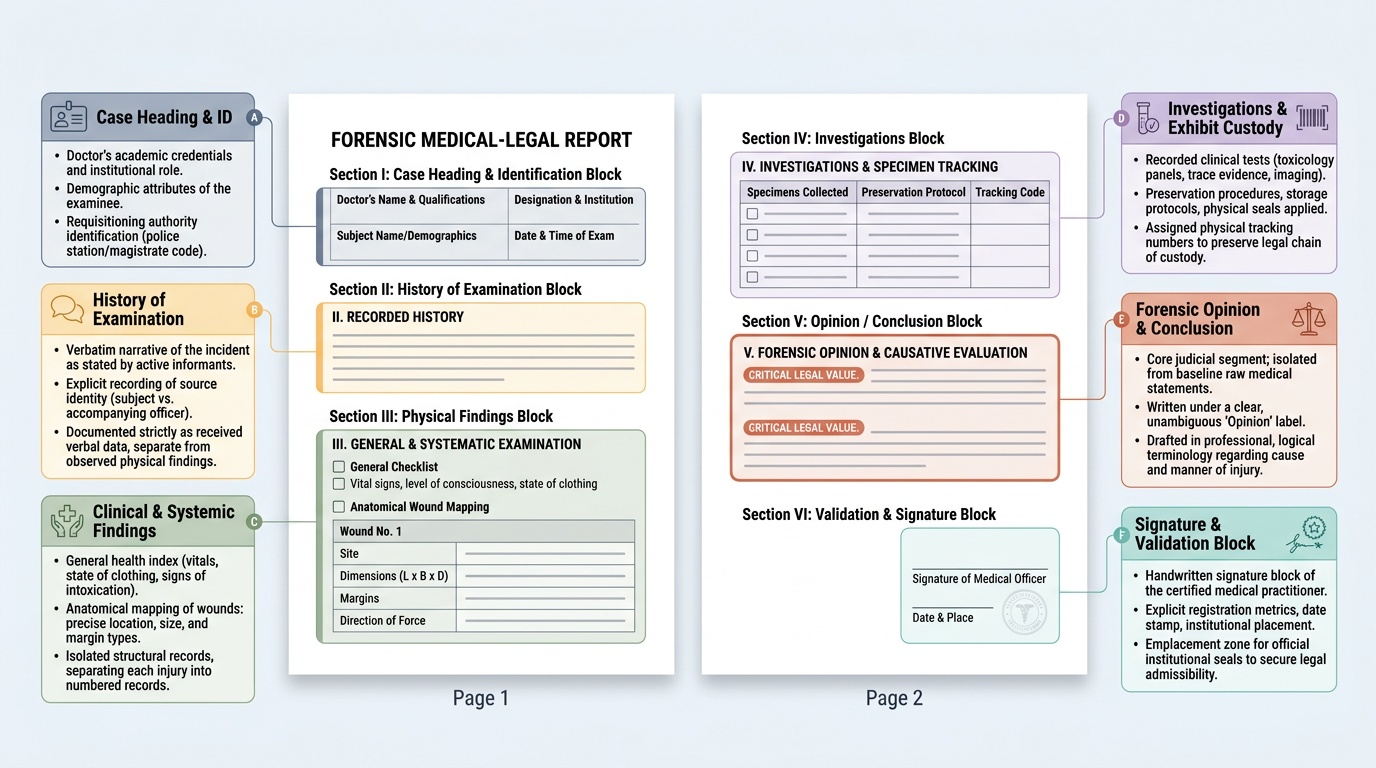
Provided image
The critical language discipline in ML reports is the distinction between findings and opinion. "There is a 3 cm incised wound over the left forearm" is a finding. "This wound is consistent with a self-inflicted injury" is an opinion. Mixing these in the findings section is a common and professionally serious error — it suggests the doctor is advocating a conclusion rather than reporting facts.
SELF-CHECK
In an ML wound report, the doctor writes in the 'Examination Findings' section: 'There is a 4 cm laceration over the right parietal region, which was most likely caused by a blunt rod.' Which is the correct professional assessment of this statement?
A. Correct — the cause should be stated alongside the finding for clarity
B. Incorrect — the cause of the wound is an opinion and must appear only in the 'Opinion/Conclusion' section, not in the findings
C. Partially correct — it is acceptable to state 'most likely' as it avoids absolute language
D. Correct, provided the doctor also photographs the wound to support the opinion
Reveal Answer
Answer: B. Incorrect — the cause of the wound is an opinion and must appear only in the 'Opinion/Conclusion' section, not in the findings
Stating the cause of a wound in the 'Examination Findings' section is a professional error because causation is a matter of opinion (inference from findings), not a direct observation. The findings section must contain only what was directly observed: site, dimensions, margins, depth, surrounding tissue changes. The opinion that the wound was caused by a blunt rod belongs in the 'Opinion/Conclusion' section, clearly labelled as the doctor's inference from the findings. Mixing opinion into the findings section makes the report vulnerable to cross-examination challenging the doctor's objectivity and methodology.
Applied Practice — Interpretation, Inference & Opinion
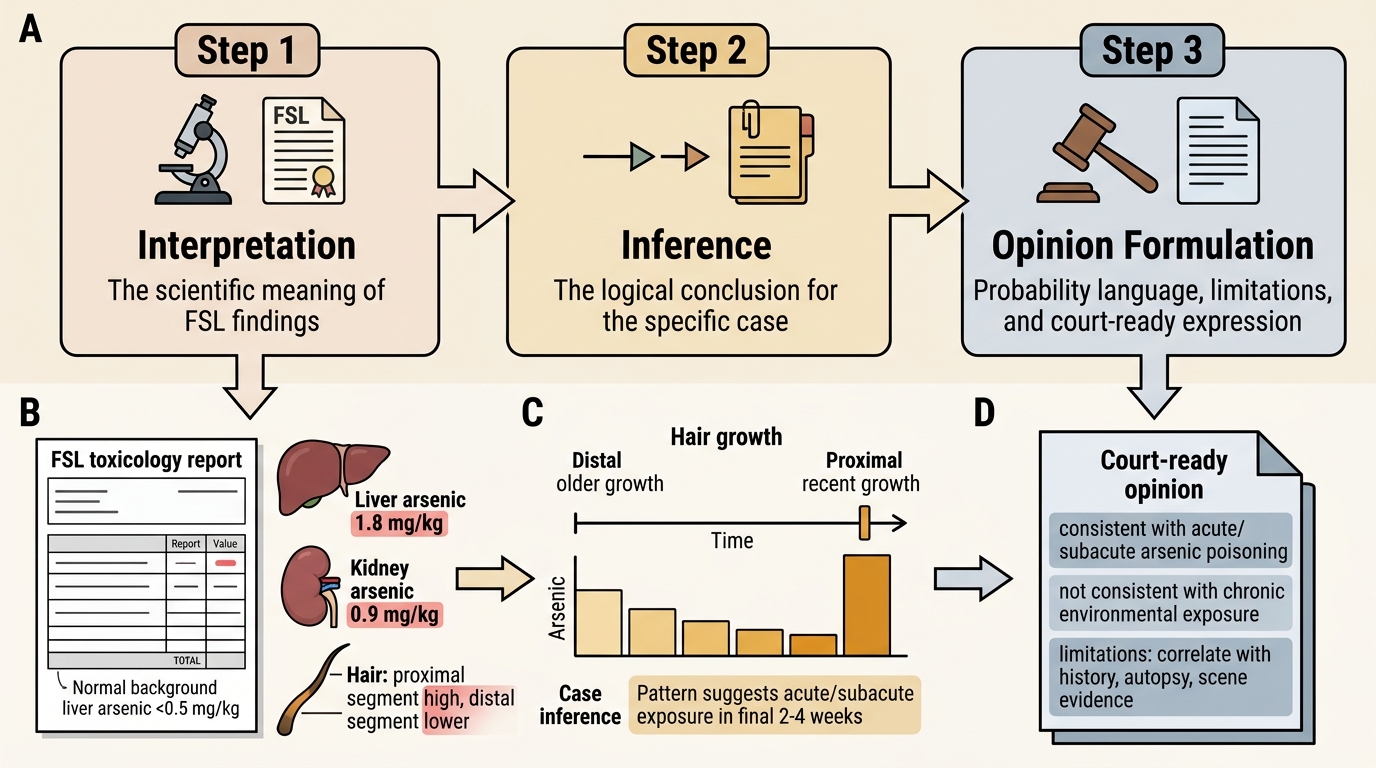
Translating forensic examination findings and laboratory results into a legally defensible opinion is the capstone skill of the forensic medical officer. The transition from raw findings to expressed opinion requires three intellectual steps: interpretation (what do these findings mean scientifically?), inference (what logical conclusion follows from this meaning in the specific case context?), and opinion formulation (how is this conclusion expressed appropriately for a legal audience, with its limitations acknowledged?).
Forensic Opinion Formulation in Arsenic Poisoning
Consider the interpretation of a FSL toxicology report in a suspected poisoning case. The FSL reports: "Arsenic detected in liver (1.8 mg/kg), kidney (0.9 mg/kg), and hair (high concentration in the proximal segment, decreasing distally)." The forensic medical officer's interpretation process should proceed as follows:
• What does this mean scientifically? Arsenic in liver at 1.8 mg/kg is above normal background levels (normal <0.5 mg/kg); the hair segmental analysis shows recent exposure (high concentration in proximal = recently grown) decreasing distally (older growth = earlier, lower or zero exposure) — consistent with acute or subacute poisoning rather than chronic environmental exposure.
• What inference follows in this case? The pattern is consistent with deliberate arsenic administration in the weeks preceding death; the peak in proximal hair segments points to exposure in the final 2-4 weeks.
• How is this expressed as an opinion? "In my opinion, the concentration of arsenic detected in the viscera and the segmental hair analysis pattern are consistent with acute/subacute arsenic poisoning and are not consistent with chronic environmental exposure. The precise timing of arsenic administration cannot be determined with certainty from these findings alone."
Several professional conventions govern the language of forensic opinion:
• Probability language is graduated: "Certain" (>99% scientific consensus), "probable" or "consistent with" (good scientific basis), "possible" (cannot exclude), "not consistent with" (contradicted by findings). The correct level of certainty must be used — overstating certainty is as professionally indefensible as understating it.
• Negative findings must be stated and their significance explained: "No defensive injuries were found" is not evidence that no assault occurred — it must be accompanied by the explanatory statement "Absence of defensive injuries does not exclude assault, as defensive injuries are not invariably present."
• Limitations of the opinion must be listed: Was DNA analysis pending? Was the examination conducted hours after the incident with potential evidence degradation? Is the opinion based on examination findings only, without FSL results? Each limitation narrows the scope of the opinion and must be stated.
• The opinion must be internally consistent: A doctor cannot opine that the wound was caused by a blunt object in one paragraph and describe clean-cut margins with no tissue bridges in the findings section — because clean margins with no tissue bridges describe an incised wound, not a laceration from blunt force. Internal inconsistency is the most effectively exploited cross-examination vulnerability.
Professionalism in interpretation also means recognising and stating when the findings are equivocal. An opinion that acknowledges two possible explanations ("The findings are consistent with either X or Y; differentiation requires additional investigations including...") is more professionally credible than a forced conclusion that overreaches the evidence.
SELF-CHECK
An FSL toxicology report shows ethanol in post-mortem blood at 300 mg/100 mL (femoral vein) in a road accident fatality. The forensic medical officer must consider that this value:
A. Directly equates to the blood alcohol concentration at the time of the accident
B. May be inflated due to post-mortem redistribution and microbiological ethanol generation — and the femoral vein result is more reliable than cardiac blood for this reason
C. Is below the legal driving limit in India and therefore confirms the driver was not impaired
D. Should be reported without qualification as the definitive ante-mortem BAC
Reveal Answer
Answer: B. May be inflated due to post-mortem redistribution and microbiological ethanol generation — and the femoral vein result is more reliable than cardiac blood for this reason
Post-mortem blood alcohol concentrations may not accurately reflect ante-mortem concentrations. Microbiological activity (bacteria in the gut can generate ethanol after death), gastric re-diffusion into adjacent vessels, and redistribution from tissues all elevate post-mortem blood alcohol. Femoral or subclavian vein blood is preferred over cardiac blood because it is more peripheral and less subject to redistribution — but even femoral vein levels must be interpreted cautiously and reported with this qualification. The legal driving limit in India (Motor Vehicles Act) is 30 mg/100 mL (0.03%) — not relevant to the interpretation question here, and 300 mg/100 mL would far exceed it regardless.
CLINICAL PEARL
The 'findings vs opinion' fault line: In cross-examination, the most reliable way to discredit a forensic medical officer is to find a place in their report where factual findings and opinions are mixed — because it allows the defence to argue the doctor was forming conclusions before completing the examination, or was advocating for a party's position rather than reporting objectively. Develop the habit of reading every sentence you write in the 'Examination Findings' section and asking: 'Is this something I directly observed (dimension, location, colour, texture, temperature), or is this something I concluded?' If it is a conclusion, it goes in the 'Opinion' section. This discipline is not bureaucratic — it is the difference between a report that survives cross-examination and one that collapses in court.
KEY TAKEAWAYS
This module has addressed the professional standards governing two related forensic competencies:
Professionalism in FSL submissions (FM12.4):
• The covering letter is the scientific guide to the analysis — it must specify FIR details, a numbered exhibit list with specimen condition, specific tests requested with rationale, and relevant case history
• Requesting 'general toxicology' without direction is a professional failure that leads to missed or misdirected analysis
• Chain of custody documentation must accompany every exhibit, from collection to FSL receipt
Professionalism in ML report writing (FM12.5):
• A medicolegal report has a canonical structure: heading, history, general examination, specific examination, investigations, opinion/conclusion, signature
• Findings must be strictly separated from opinion — the opinion/conclusion section is where inference and causation belong
• Opinion language is graduated: 'consistent with', 'probable', 'possible', 'not consistent with' — matched to the level of scientific certainty the findings support
• Negative findings must be stated and their absence explained, not omitted
• Internal consistency is non-negotiable — findings and opinion must tell the same anatomical story
The forensic medical officer's duty: Runs to the court and to justice — not to police, prosecution, defence, or the clinical patient relationship. Objectivity, accuracy, completeness, and reproducibility are the professional pillars.
REFLECT
Read this scenario and reflect honestly:
A police officer delivers a requisition for a medicolegal examination of a 15-year-old boy who allegedly assaulted an adult. The officer tells you informally, before the examination, 'This boy is definitely guilty — just write it that way.' After the examination, you find some bruising on the boy's knuckles consistent with punching, but also an old healed scar on his wrist from a prior injury that could have caused the bruising.
- What is your professional obligation, and to whom does your duty run in this examination?
- How do you document the bruising and the old scar in your report — in findings or in opinion? What language do you use?
- The boy is 15 — does any specific legislation govern this examination and your documentation obligations?
- If you comply with the officer's informal request and write a report favouring guilt, what professional and legal consequences could follow for you personally?
- If you write an objective report that acknowledges the ambiguity in the findings, how does this serve the interests of justice better than a biased report, even if it makes the prosecution's case harder?