Page 1 of 20
FM5.1 | Types & Classification of Mechanical Injuries — SDL Guide
Learning Objectives
- Define and classify mechanical injuries into blunt force and sharp force categories
- Describe the pathological and macroscopic features distinguishing abrasion, contusion, laceration, incised wound, stab wound, and chop wound
- Explain the medico-legal significance of tissue bridges, wound margins, and wound dimensions in determining the causative weapon
- Identify defence wounds, self-inflicted wounds, and fabricated injuries and interpret their medico-legal implications
INSTRUCTIONS
In forensic medicine, the accurate characterisation of a wound is not merely a clinical description — it is a legal opinion. The difference between a laceration and an incised wound, or between a stab wound and a chop wound, determines whether a weapon was blunt or sharp, which directly informs the legal charge. A forensic physician who blurs these distinctions can inadvertently mislead an investigation or a court. This module establishes the rigorous definitional framework for all major mechanical wound types, grounded in the pathological mechanisms that produce them, and links each type to its medico-legal significance under the Bharatiya Nyay Sanhita.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 32-year-old man is brought to the casualty with a wound on his left forearm. The police constable accompanying him insists the wound was inflicted by a knife during a robbery. On examination, the wound measures 4 cm in length, 0.5 cm in depth, has clean, well-defined margins with no tissue bridges, and tapers at both ends. A second wound, 3 cm long, is found on the dorsum of the left hand. The accused is in custody but claims he was carrying only a lathi. Your MLC report will determine whether the magistrate charges him with simple hurt, grievous hurt, or attempt to murder. Which wound type are you looking at — and does the physical evidence support the constable's version or contradict it?
WHY THIS MATTERS
The classification of mechanical injuries is the foundational skill of clinical forensic medicine. Every other medico-legal inference — the nature of the weapon, the circumstances of an assault, whether injuries are ante-mortem or post-mortem, whether they are self-inflicted or homicidal — depends on correctly identifying the wound type first. Under the Bharatiya Nyay Sanhita (BNS), the categories of hurt (simple, grievous, dangerous) and the possible charges (assault, culpable homicide, murder) are shaped by wound characteristics that you, as the examining doctor, document. A wrong classification is not just an academic error; it is a potential miscarriage of justice. Understanding the precise pathological basis of each wound type is therefore inseparable from understanding your role as a medico-legal expert.
RECALL
Before proceeding, bring to mind the layers of skin from anatomy: epidermis → dermis → subcutaneous tissue → deep fascia → muscle. Different wound types violate different layers and activate different repair cascades studied in physiology and pathology. Recall that mechanical force can be delivered as a blunt impact (diffuse energy over a broad area) or as a sharp edge/point (concentrated energy along a line or point). The physics of force delivery — area over which it is distributed — is the primary determinant of the wound type produced. You will also recall the concept of a tissue bridge from your pathology classes: strands of connective tissue and small vessels that span a wound gap when tissue is torn rather than cut cleanly.
The Medico-legal Significance of Wound Classification
When a forensic physician examines an injured person and writes a medico-legal certificate (MLC), the document serves simultaneously as a medical record and a piece of legal evidence. The courts and investigating agencies rely on the MLC to reconstruct the assault: what type of weapon was used, how much force was applied, and whether the injury is consistent with the version of events narrated by the parties. The classification of a wound type is therefore a medico-legal opinion, not merely a clinical description, and it carries the weight of expert testimony.
Consider the scenario above. A wound with clean margins, tapering ends, greater length than depth, and no tissue bridges is an incised wound — produced by a sharp-edged weapon. This is inconsistent with a lathi, which would produce a laceration or a contusion. The second wound on the dorsum of the hand, in this context, is consistent with a defence wound — an injury sustained while the victim raised their hand to ward off a blow. Together, these findings corroborate the victim's account and contradict the accused's. The medico-legal certificate thus becomes the centrepiece of the prosecution.
The inverse is equally important. A wound described vaguely as a 'cut' or 'injury' without specifying its type has no discriminatory legal value. Indian courts have repeatedly held that a forensic opinion is only as useful as its factual foundation — and that foundation is the precise morphological characterisation of the wound. For this reason, the terminology used in this module — abrasion, contusion, laceration, incised wound, stab wound, chop wound — must be used with precision and never interchanged loosely.
Blunt Force Injuries: Abrasion, Contusion, and Laceration
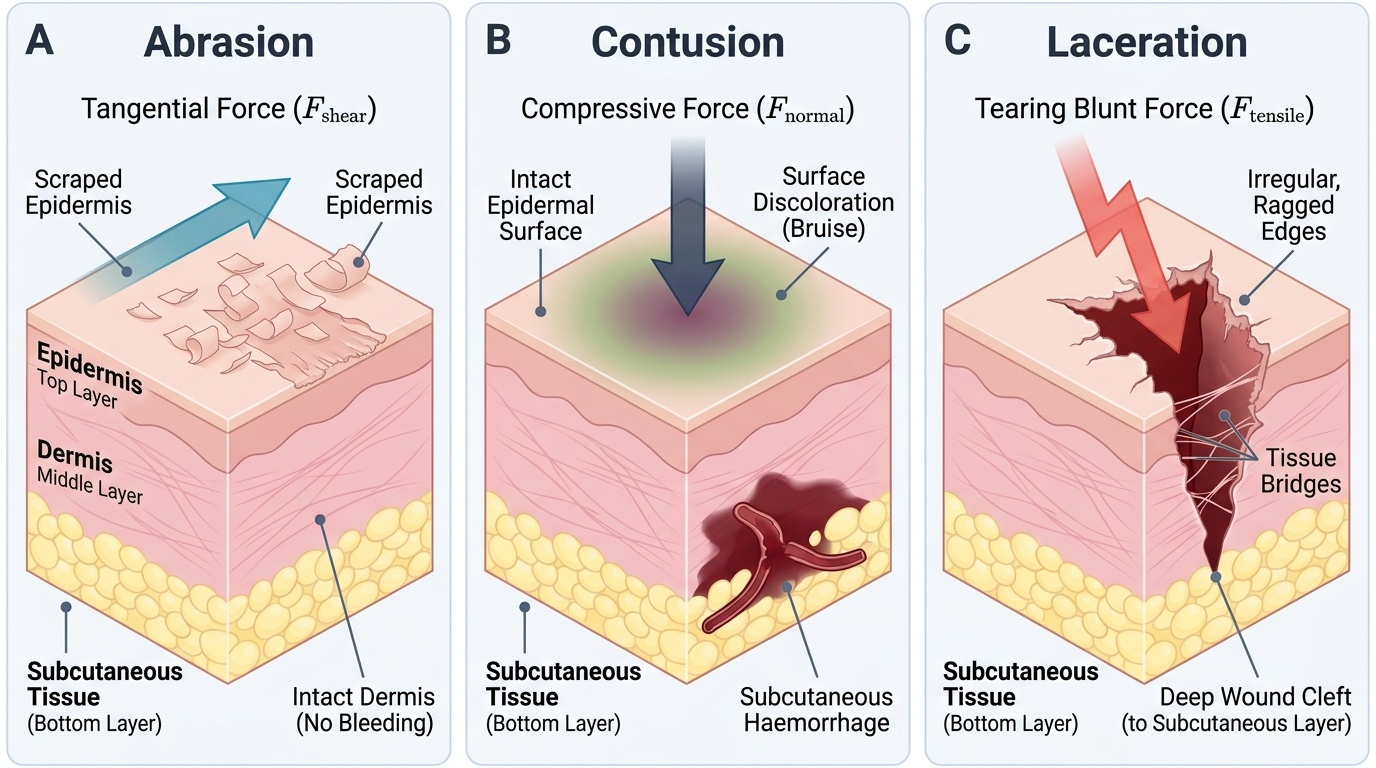
Blunt force injuries are produced when a surface with a relatively broad contact area strikes the body or the body strikes such a surface. The energy is distributed across the contact zone rather than being concentrated along an edge or point. Depending on the magnitude and direction of force, the skin and underlying tissues respond differently, producing three distinct wound types whose medico-legal significance differs substantially.
Abrasion is the most superficial mechanical injury, involving only the epidermis. It is produced by a tangential (scraping/sliding) or compressive force that disrupts the epidermal layers without creating a gap in the skin. By definition, an abrasion does not penetrate the dermis, produces no deep haemorrhage, and does not require suturing. Its medico-legal value lies in its ability to record the direction of force (through the pattern of dislodged epithelial cells and crust formation), indicate contact with a surface (road rash abrasions reflecting tarmac patterns), and confirm ante-mortem injury (vital reaction at the base). A post-mortem abrasion is dry, parchment-like, and yellow-brown, with no vital reaction.
Contusion (commonly termed a bruise) results from blunt compressive force applied to an area of skin, causing rupture of blood vessels beneath an intact skin surface. The haemorrhage extravasates into the subcutaneous tissue and deeper planes without breaching the skin. Contusions are clinically visible as discolouration that shifts from red-purple (acute) through blue-black to green and finally yellow-brown as haemoglobin is metabolised — a feature exploited in medicolegal age estimation of injuries (though individual variation and body site substantially affect colour change timing). Patterned contusions — where the bruise reproduces the shape of the causative object — are of particular forensic value (e.g. a belt buckle mark, a finger-grip bruise). Contusions may be absent at the time of examination if they have not yet surfaced, particularly in areas with thick subcutaneous fat.
Laceration is produced by blunt force tearing, bursting, or crushing the skin and underlying tissue. The defining hallmark of a laceration is its irregular, ragged edges and — most importantly for medico-legal purposes — the presence of tissue bridges: strands of connective tissue, nerve fibres, and small blood vessels that span the wound gap because tissue has been torn apart rather than cut cleanly. The wound floor often contains contamination (soil, grease, fibre) from the causative object. Lacerations may superficially resemble incised wounds when located over bony prominences (where the skin bursts cleanly under pressure from below), but even in these 'burst lacerations', examination with a hand lens will reveal tissue bridges and irregular depths.
The table below summarises the key distinguishing features:
| Wound type | Skin surface | Edges | Tissue bridges | Haemorrhage | Depth |
|---|---|---|---|---|---|
| Abrasion | Broken, no gap | N/A (no wound gap) | None | Superficial seepage only | Epidermis only |
| Contusion | Intact | N/A (no wound gap) | None | Subcutaneous, intact overlying skin | Subcutaneous+ |
| Laceration | Breached | Irregular, ragged | Present | Variable | Variable |
Provided image
SELF-CHECK
A 25-year-old male presents after a road traffic accident. Examination reveals a wound over the right shin measuring 3 cm × 2 cm with irregular margins, reddish strands of tissue spanning the wound gap, and grit embedded in the base. What type of wound is this?
A. Abrasion
B. Contusion
C. Laceration
D. Incised wound
Reveal Answer
Answer: C. Laceration
The hallmark features here are irregular margins and tissue bridges (the reddish strands spanning the wound gap) — these confirm a laceration. Abrasion involves only the epidermis with no wound gap. Contusion has intact overlying skin. Incised wounds have clean margins and no tissue bridges. The embedded grit is consistent with a blunt impact on tarmac, further supporting laceration.
Sharp Force Injuries: Incised Wound, Stab Wound, and Chop Wound
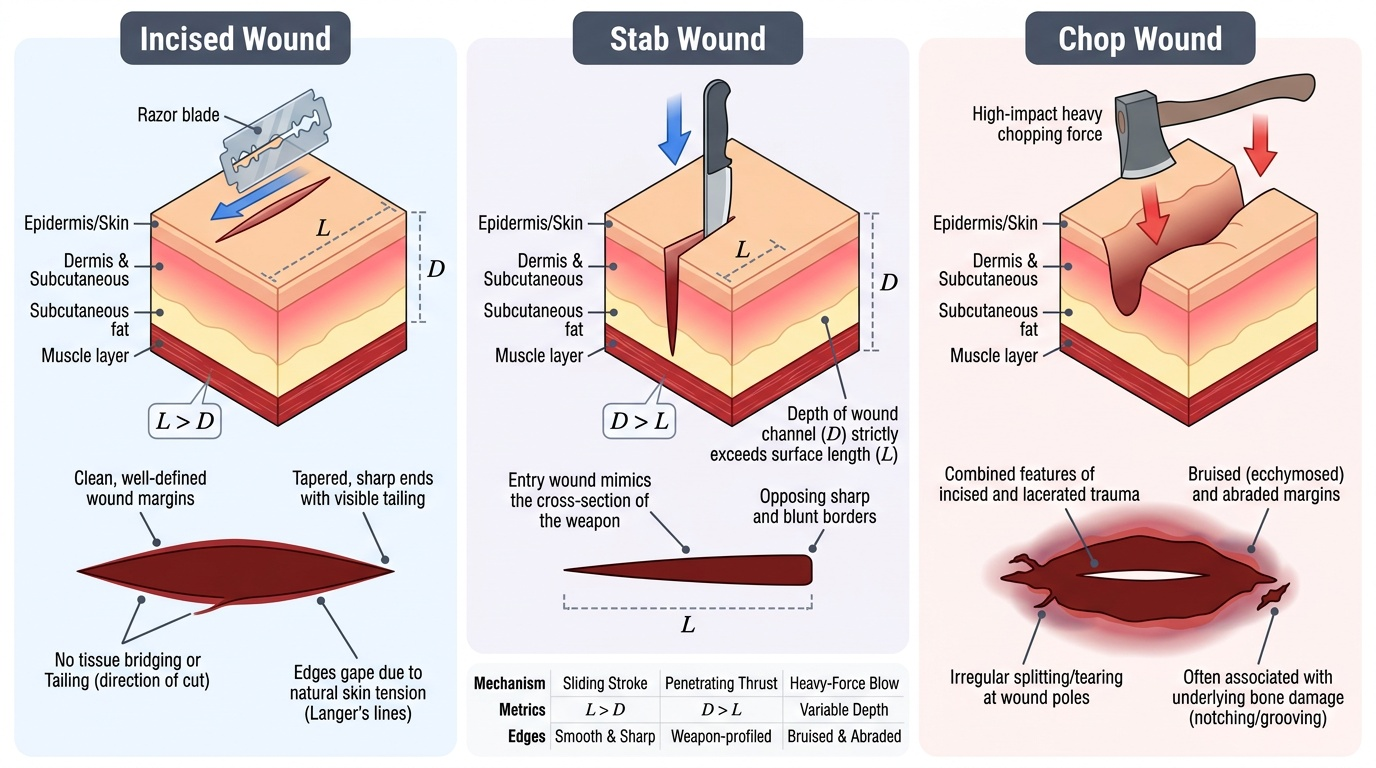
Sharp force injuries are produced when a weapon with a fine edge or point concentrates mechanical energy along a line or at a point, respectively. Because energy is not diffused over a broad area, the skin is divided cleanly rather than torn. The three major types differ principally in the geometry of the weapon, the direction and depth of force application, and the resulting wound dimensions — differences that are central to forensic weapon identification.
Incised wound (also called a cut or slash wound) is produced by a sharp-edged weapon (knife, razor, broken glass, scalpel) drawn along or across the skin. The key dimensional rule, first enunciated by Reddy and codified in all standard FM texts, is that length exceeds depth — the weapon creates a longer surface defect than it penetrates. The wound has clean, well-defined margins that bleed freely; the cut ends (tailing) are typically sharp and tapering. Critically, tissue bridges are absent because tissue is divided rather than torn. The wound gapes because of the elasticity of skin — the gape is proportional to the tension lines of the skin at that site. Incised wounds on the neck that are suicidal are typically multiple, parallel, and tentative (hesitation cuts) at the margins of the main wound.
Stab wound is produced by a sharp-pointed weapon (knife, dagger, screwdriver, ice pick) thrust into the tissue, so that depth exceeds length. The entry wound's shape reflects the cross-sectional geometry of the weapon: a knife with one sharp edge and one blunt edge produces a wound with one pointed end and one squared/notched end; a double-edged blade (dagger) produces a wound with two tapering ends. The track of a stab wound through tissue provides information about the weapon length, direction of thrust, and angle of entry. Stab wounds are of particular medico-legal importance because they penetrate body cavities (thorax, abdomen) and are disproportionately dangerous relative to their small surface appearance. Internal examination is mandatory to determine whether a body cavity has been entered and which organs are injured.
Chop wound is produced by a heavy sharp weapon (axe, dao, gandasa, kripan) delivered with force. The combination of weight and sharpness means the wound exhibits features of both incised and lacerated wounds: the entry margins may be relatively clean (from the sharpness), but the deeper tissues show tearing and crushing (from the weight and force), and bone is often notched or fractured. Chop wounds are characteristically associated with homicide and are common in certain regional patterns of violence. They may result in complete amputation of limbs if the weapon is sufficiently heavy.
Provided image
CLINICAL PEARL
The single most important medico-legal distinction between a laceration and an incised wound is the tissue bridge. Both can occur on the scalp, the chin, or the eyebrow and may appear superficially similar, especially after bleeding. However, gently approximating the wound edges and examining the base with adequate light will reveal tissue bridges in a laceration but clean, empty wound edges in an incised wound. This one finding changes the weapon class from blunt to sharp, which is legally transformative. Never record a wound as a 'cut' without first confirming the absence of tissue bridges.