Page 2 of 20
FM5.1 | Types & Classification of Mechanical Injuries — SDL Guide (Part 2)
Examination Findings and Documentation of Wound Type
The medico-legal examination of a wound follows a systematic protocol designed to capture every feature that a court may later enquire about. The examining physician must record findings in contemporaneous notes that are detailed, accurate, and free of legal conclusions — those are inferred from the facts, not stated in place of them. The standard approach follows the mnemonic SSSMD: Site, Size, Shape, Surroundings, and Margin/Depth characteristics.
Site: recorded in relation to fixed anatomical landmarks, with distance from the midline and from the nearest joint or bone prominence. The site of a wound is relevant to determining whether it is in an accessible location (for self-infliction) and whether it is consistent with the described mechanism.
Size: measured in two dimensions (length × width), with depth noted separately for stab and chop wounds. A wound that is measured only approximately (e.g. 'about 3 cm') loses discriminatory forensic value. Photographs with a scale marker are standard in modern practice.
Shape: the geometric form of the wound — linear, triangular, stellate, circular, Y-shaped, or irregular. Shape is often weapon-specific. A stellate (star-shaped) laceration over the scalp suggests a circular or spherical blunt instrument; a Y-shaped laceration suggests a horseshoe or ring-shaped object.
Surroundings: the presence of bruising, abrasion collars (in firearm wounds), tattooing, soiling, ligature marks, or other secondary findings around the wound that contextualise the injury.
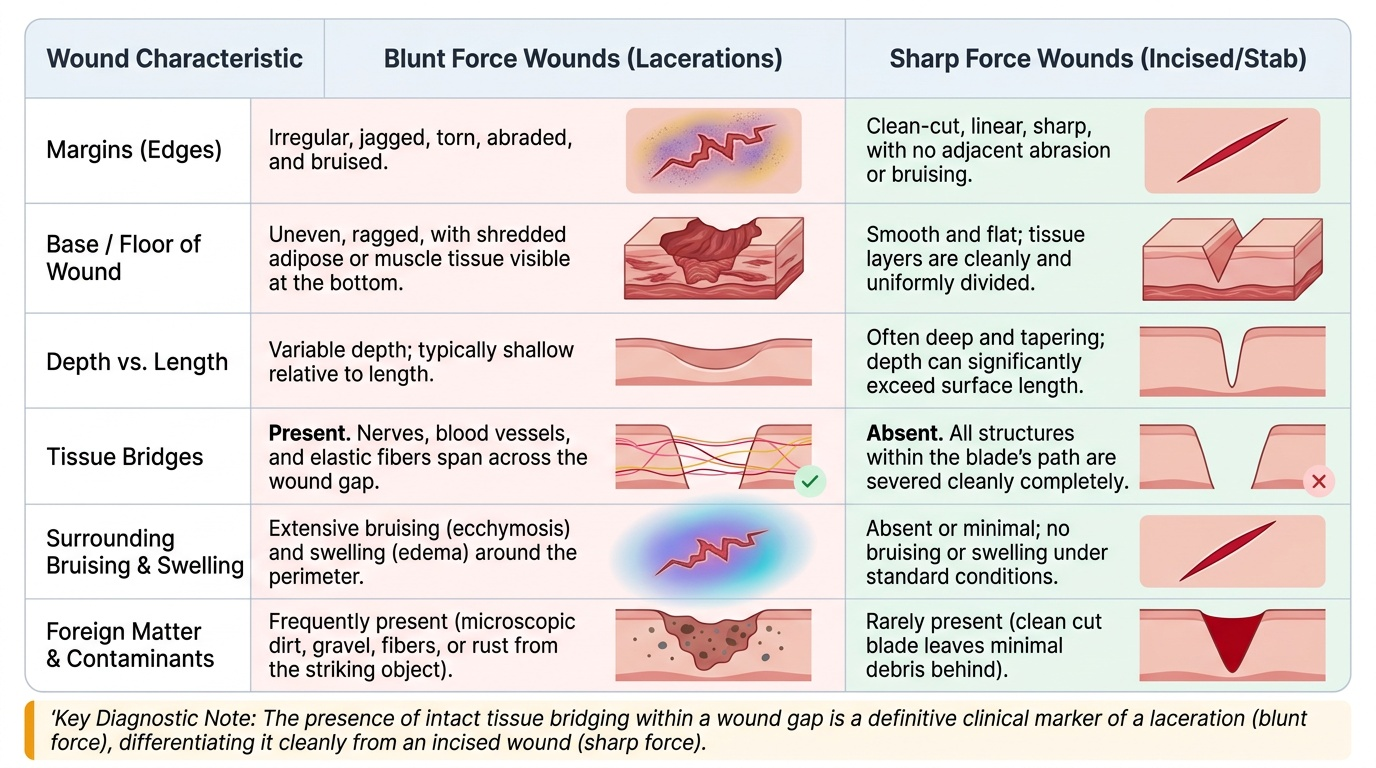
Margins and base: the most critical examination step for wound classification. Clean vs ragged margins, presence or absence of tissue bridges, depth pattern (uniform vs tapering), and the nature of the wound floor (muscle, bone, fat) must all be recorded. Additionally, the presence or absence of vital reaction (bleeding, inflammation) informs ante-mortem vs post-mortem status.
Provided image
SELF-CHECK
A wound on the left anterior chest measures 2 cm in length on the skin surface. The wound track extends 8 cm deep into the thoracic cavity, entering the lung. Which wound type is this and what is the correct medico-legal classification?
A. Laceration — blunt force injury
B. Incised wound — sharp force injury, length > depth
C. Stab wound — sharp force injury, depth > length
D. Chop wound — heavy sharp weapon injury
Reveal Answer
Answer: C. Stab wound — sharp force injury, depth > length
This is a stab wound. The defining dimensional criterion for a stab wound is that depth exceeds length (2 cm surface entry, 8 cm depth). The skin entry is produced by a sharp point. Compare with an incised wound where length exceeds depth. The entry into the thoracic cavity and lung confirms penetrating injury, which is the typical danger of stab wounds — their surface appearance grossly underestimates their internal damage.
Defence Wounds, Self-inflicted Wounds, and Fabricated Injuries
Beyond simple wound type identification, forensic medicine requires interpretation of wound patterns in the context of the reported circumstances. Three special categories — defence wounds, self-inflicted wounds, and fabricated injuries — are frequently encountered in medico-legal practice and require specific recognition criteria that go beyond individual wound morphology.
Defence wounds are injuries sustained by a victim who attempts to ward off an attack. They are most commonly found on the ulnar border of the forearm and the dorsum of the hand (raised to block blows), the palm (gripping a blade), and occasionally the outer legs and feet (in victims lying on the ground). Defence wounds are typically multiple, parallel, and on the non-dominant arm (right-handed victims raise their left arm). In a homicidal attack with a sharp weapon, finding multiple incised wounds on the hands and forearms alongside the primary fatal wound strongly corroborates the victim's resistance and the homicidal nature of the assault. The absence of defence wounds in a purportedly violent homicidal assault may indicate that the victim was incapacitated (drugged, restrained, asleep, unconscious) before the attack.
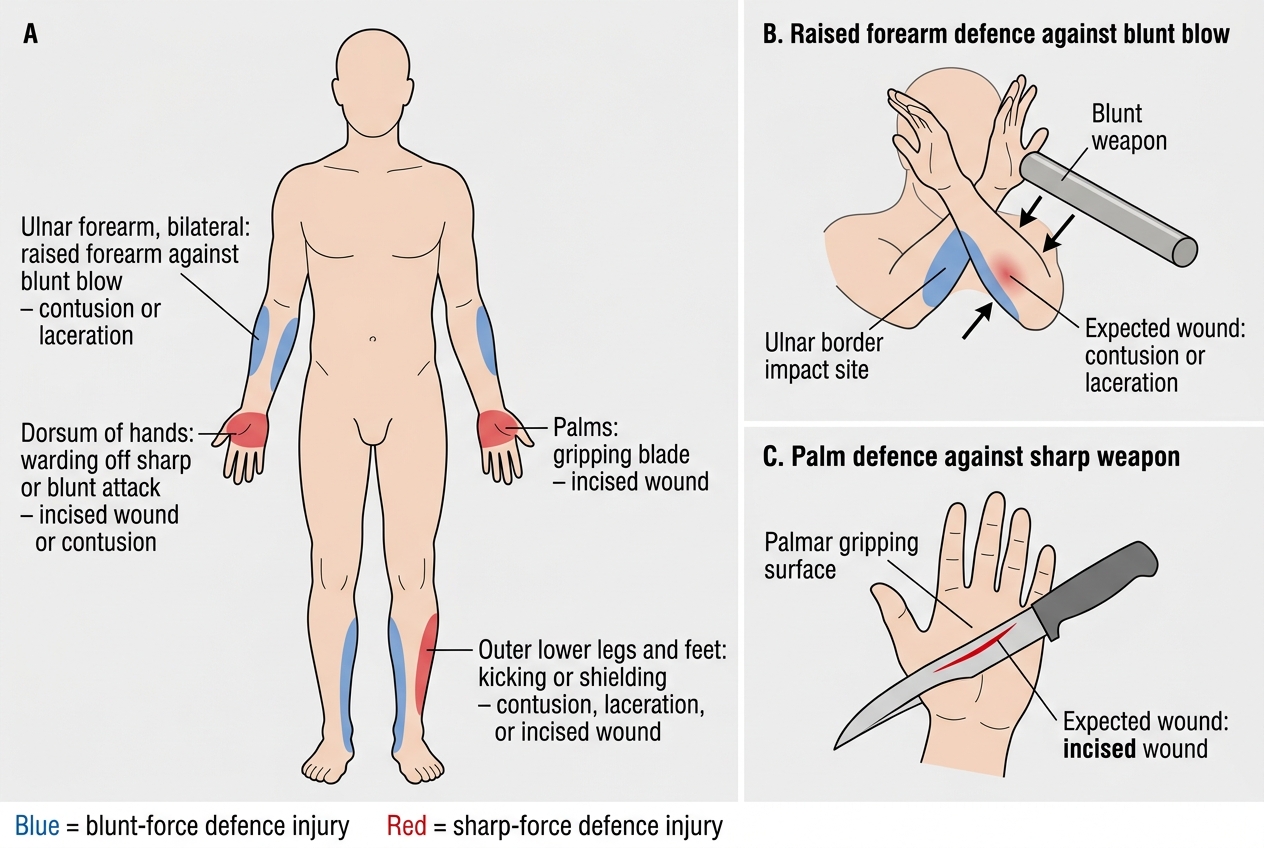
Typical Defence Wound Sites and Mechanisms
Self-inflicted wounds are intentionally produced by the individual, either as suicidal attempts or for purposes of deception (claiming assault). Genuine suicidal wounds have characteristic features: they are located on accessible sites (anterior wrist, neck, antecubital fossa), are typically of uniform depth and parallel orientation, and are often accompanied by hesitation marks (multiple shallow exploratory incisions alongside the main wound). Suicidal stab wounds are rare but typically involve the chest or abdomen in the midline. The individual can sustain self-inflicted wounds only in areas reachable by their own dominant hand — wounds on the back, the back of the neck, and the posterior lower limb cannot be self-inflicted.
Fabricated injuries are wounds claimed by the individual but produced by themselves, or produced post-mortem and attributed to assault. Key features distinguishing fabricated from genuine assault wounds include: superficial depth (the fabricator unconsciously avoids pain); absence of vital reaction if inflicted post-mortem; accessible and unobstructed locations only; and the absence of defence wounds in a claimed violent assault. The medico-legal opinion in a case of suspected fabricated injury must be stated carefully: it should document the factual findings and opine that the injuries are 'consistent with self-infliction' or 'inconsistent with the described mechanism', rather than flatly accusing the complainant of fabrication.
The medicolegal inference from wound patterns is always probabilistic, not absolute. Convergence of multiple features (site pattern, accessibility, hesitation marks, absence of defence wounds) increases the confidence of the opinion.
SELF-CHECK
A woman presents claiming she was attacked by her husband with a knife. Examination reveals 6 superficial, parallel incised wounds on her left anterior wrist, all of uniform depth approximately 2 mm, with 3 shallow tentative marks alongside them. There are no wounds on her hands, forearms, or any other site. Which medico-legal opinion is MOST appropriate?
A. The injuries are consistent with a homicidal sharp force assault
B. The injuries are consistent with self-infliction; no defence wounds or evidence of struggle found
C. The injuries confirm fabrication and the complaint should be dismissed
D. The injuries are inconclusive as both homicidal and self-inflicted wounds can appear identical
Reveal Answer
Answer: B. The injuries are consistent with self-infliction; no defence wounds or evidence of struggle found
The constellation of features — anterior wrist location (accessible), parallel uniform-depth superficial wounds, hesitation marks, and complete absence of defence wounds — is the classic pattern of self-inflicted wounds. The medico-legal opinion should state that the injuries are 'consistent with self-infliction' and note the absence of features supportive of homicidal assault. Option C is incorrect: the doctor must NOT dismiss the complaint — that is for the court to decide. Option D is incorrect because these features are not equally consistent with homicidal attack.