Page 14 of 18
FM10.{10,13-15} | Communication, Social Aspects & Managing Pressure in MLCs — SDL Guide
Learning Objectives
- Describe the roles and responsibilities of doctors in communication with patients, colleagues, media, and the public
- Identify the social and psychological needs of MLC case survivors — assault, rape, attempted suicide, domestic violence
- Apply a structured framework for managing the communication challenges in medico-legal cases
- Define pressure in the medico-legal context and classify its types, causes, and sources
- Demonstrate skills in conflict resolution, boundary maintenance, and handling institutional/family/media pressure in MLC management
INSTRUCTIONS
The forensic and legal dimensions of medicine are only part of the medico-legal clinician's challenge. The other dimension — managing communications with patients, families, media, and institutional hierarchies while under pressure — is rarely taught systematically but accounts for many of the professional breakdowns seen in practice. FM10.10, FM10.13, FM10.14, and FM10.15 together address the human and organisational dimensions of MLC management.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 2 AM. The emergency department is managing three simultaneous medico-legal cases: (1) a survivor of a gang assault, terrified and refusing to have the police called; (2) a young woman brought in following an attempted suicide by medication overdose, asking to be discharged immediately; (3) a rape survivor in extreme distress, accompanied by a male relative who is demanding information about 'what happened.' A television news van is parked outside. The medical superintendent calls to ask that all media enquiries be referred to the hospital's PR team and no information is given. Three nursing staff are asking you what to say to the families in the waiting area.
How do you prioritise your communication obligations? What do you tell the assault survivor, the attempted suicide patient, the rape survivor's relative, the media, and the nursing staff? And how do you manage the institutional and family pressure you are facing simultaneously?
WHY THIS MATTERS
Communication failures in medico-legal cases cause harm at every level: they re-traumatise survivors, undermine trust in the medical system, lead to false or misleading public information, generate professional complaints, and sometimes obstruct justice. Yet medical education gives minimal time to the how of these communications. FM10.10–FM10.15 operationalise the skills needed: what to say and what not to say to a rape survivor's family; how to decline media comment without creating legal exposure; how to resist institutional pressure to alter an MLC record; and how to recognise when one's own stress response is compromising clinical judgment.
RECALL
Recall from prior FM and ethics learning:
- Confidentiality — the fundamental obligation to protect patient information; has specific applications in MLC cases.
- Informed consent and capacity — particularly relevant for the attempted suicide case: a patient expressing intent to self-discharge after overdose may lack capacity.
- Medico-legal case (MLC) — definition and mandatory obligations (documentation, police intimation) covered in earlier SDLs.
- IPC 375–376 — rape defined and penalised; 2013 Criminal Law Amendment Act expanded definitions significantly.
- Mental Healthcare Act 2017 — decriminalised attempt to suicide under IPC 309 (decriminalised as a rebuttable presumption); created obligations for the State to provide care.
- Right to silence and media — no legal obligation on a clinician to speak to the media; the hospital's communications policy governs this.
Communication Between Doctors, Public, and Media: Legal and Professional Context
Medical communication in the context of medico-legal cases operates within a framework of competing obligations — the duty of confidentiality to the patient, the public's right to information about health matters, the media's constitutional right to free speech, and the clinician's own professional rights and limitations. Getting this balance right is both a professional obligation and a practical survival skill.
Communications with patients in MLC settings:
The primary communication obligation is always to the patient. In an MLC context, the communication must be structured to: (a) create a safe, private environment; (b) avoid re-traumatisation through careless questioning or presence of witnesses; (c) provide accurate information about what the medico-legal examination involves and why; and (d) obtain informed consent for each step of the examination, particularly in sexual assault cases. Patients in MLC settings are frequently in states of acute psychological distress — the clinician's communication style has a direct therapeutic effect in addition to its legal documentation function.
Communication with the media:
The NMC Code of Ethics and hospital governance policies generally require that individual clinicians do not communicate with the media about individual patient cases — this would breach confidentiality. The correct approach is:
- All media enquiries about specific patients or cases must be directed to the designated hospital spokesperson or the hospital's public relations officer.
- A clinician may communicate with the media about general health matters, public health campaigns, or medical knowledge in their area of expertise — this is permissible and in the public interest.
- A clinician must NEVER provide a patient's name, diagnosis, identity, or case details to any media without the patient's explicit written consent.
- In high-profile cases (road accidents, mass casualty incidents, high-profile persons), the pressure from media can be intense; the clinician must maintain confidentiality regardless of the public interest argument being advanced.
- Sub-judice rule: if a case is before a court, commenting publicly on the medical evidence or findings could be held in contempt of court. The clinician must be particularly careful in active criminal investigations.
Communication with law enforcement:
Doctors have a legal obligation under CrPC Section 39 to inform police of cognisable offences. When communicating with police, the clinician must:
- Share only the factual clinical findings, not interpretations beyond clinical expertise (e.g., do not opine on who caused the injury, only on the nature of the injury).
- Maintain the patient's right to confidentiality of non-relevant medical information.
- Produce medical certificates and records in response to court orders or police requisitions with appropriate legal authority.
- Not allow police to be present during the clinical examination without the patient's explicit consent.
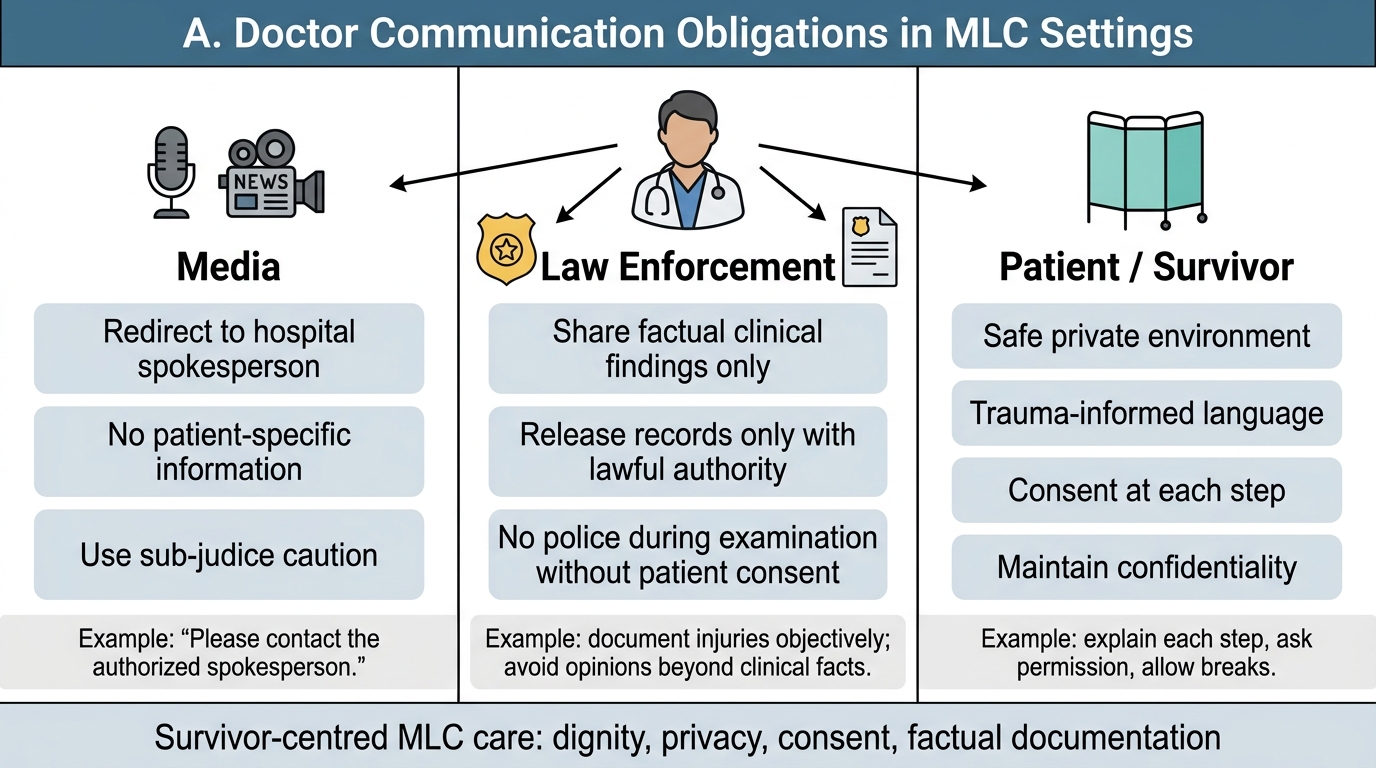
Doctor Communication Duties in MLC Settings
Social Aspects of MLC Cases: Survivor-Centred Principles
The social and psychological dimensions of medico-legal cases deserve the same rigorous attention as the forensic documentation. Survivors of assault, rape, attempted suicide, homicide (families), domestic violence, and dowry-related cases all present with specific psychosocial needs that the clinician must address alongside the clinical and legal obligations.
Survivors of sexual assault (rape):
The examination and management of rape survivors requires specialised sensitivity. Key principles grounded in survivor-centred care:
- The survivor must always be examined by a clinician of their preferred gender where possible — request and document this preference.
- The examination should be conducted in a private room, with only essential personnel present.
- The survivor controls the pace of the examination — no steps should proceed without ongoing consent.
- Never ask 'why didn't you resist' or 'why were you there' — these are victim-blaming questions that are harmful, unprofessional, and irrelevant to the clinical documentation.
- Document injuries meticulously; collect forensic evidence per standard protocol (DNA swabs, clothing preservation, nail clippings).
- Provide emergency contraception if requested and clinically indicated (within 72 hours of exposure).
- Offer and arrange post-exposure HIV prophylaxis if indicated.
- Arrange follow-up counselling and refer to designated support services.
Survivors of assault (non-sexual):
The social context of the assault (gang attack, road accident, politically motivated violence) shapes the survivor's needs. The clinician must: be alert to intimidation by accompanying individuals; ensure the patient can give history privately; and document the clinical findings accurately regardless of who accompanies the patient.
Patients with attempted suicide:
Attempted suicide is not a criminal offence in India — the Mental Healthcare Act 2017 effectively decriminalised it by creating a rebuttable presumption that a person who attempts suicide is under severe stress, relieving them of criminal liability under IPC 309. The clinician's obligations are:
- Provide immediate medical care.
- Assess and document the degree of medical risk from the overdose/method.
- Assess mental capacity: a patient requesting immediate discharge after a significant overdose may lack capacity — if so, the emergency exception to consent applies.
- Assess suicide risk: use a structured tool (e.g., Columbia Suicide Severity Rating Scale) to determine level of risk.
- Register as MLC and inform police, but do so with sensitivity — the criminal law implications are minimal post-MHC Act 2017.
- Arrange psychiatric evaluation before discharge; do not discharge a high-risk patient without mental health assessment.
Families of homicide victims:
The families of homicide victims frequently need accurate information about the post-mortem findings, the identification of the body, and the clinical circumstances of death. The clinician must: (a) provide factual information in a compassionate setting; (b) not speculate about circumstances beyond clinical findings; (c) not release the body without completion of medico-legal procedures and police clearance; (d) be alert to secondary trauma in family members and arrange bereavement support.
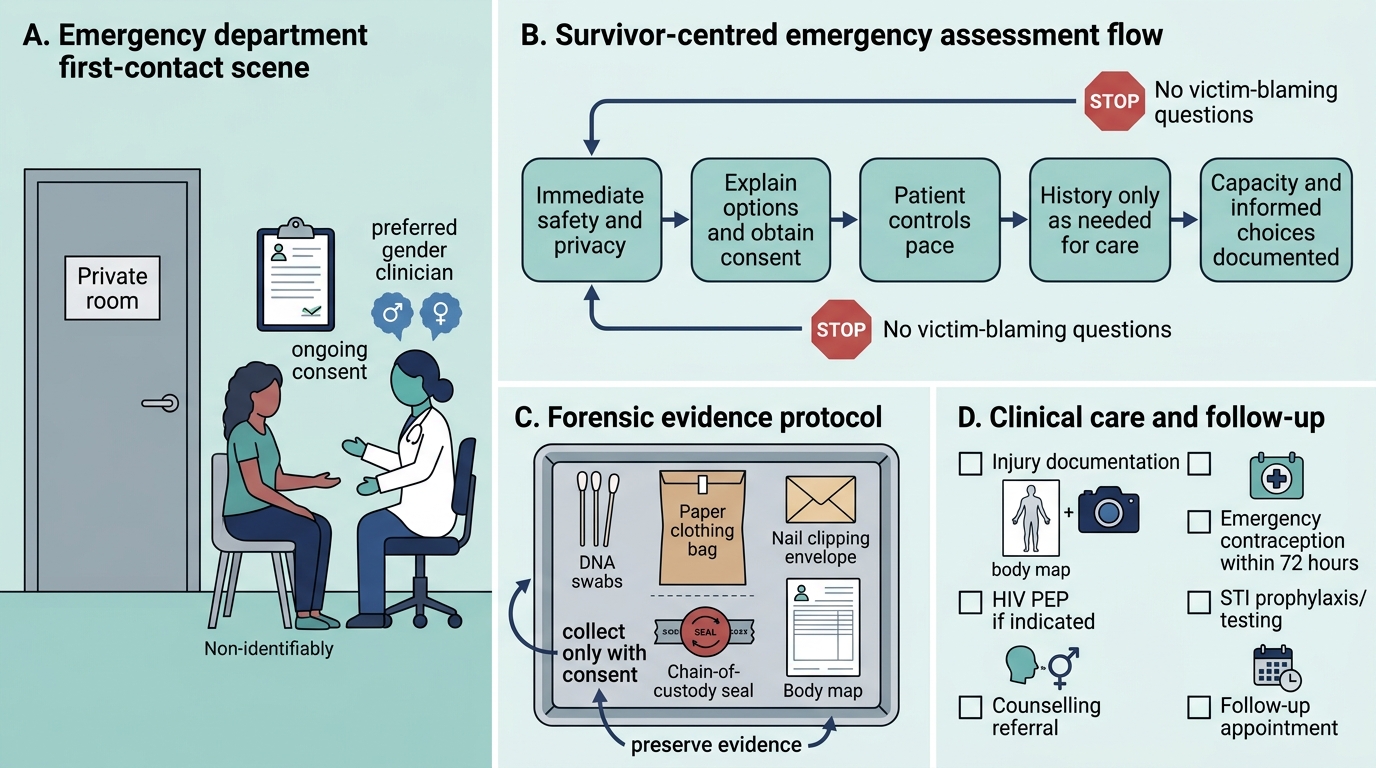
Survivor-Centred Emergency Assessment After Rape Presentation
SELF-CHECK
A 21-year-old woman is brought to the emergency department following an attempted suicide by paracetamol overdose. After receiving initial treatment, she is clear and insistent that she wishes to leave immediately and refuses further assessment. Her mother and the ward nurse agree she 'seems fine.' What is the CORRECT clinical and medico-legal response?
A. Discharge the patient because she is insistent and appears lucid
B. Detain her under police custody because attempted suicide is a criminal offence
C. Assess her decision-making capacity formally; if capacity is intact, provide information about risk and document her informed refusal; if capacity is impaired, apply the doctrine of necessity to retain her for immediate risk assessment
D. Allow the mother to take her home on the mother's written consent
Reveal Answer
Answer: C. Assess her decision-making capacity formally; if capacity is intact, provide information about risk and document her informed refusal; if capacity is impaired, apply the doctrine of necessity to retain her for immediate risk assessment
The key steps are: (1) assess decision-making capacity — does she understand the medical risk of paracetamol overdose, that delayed liver failure can occur even when she feels well, and the consequences of declining assessment? (2) If capacity is intact, she retains the right to refuse — provide the information, document meticulously, and offer safe return. (3) If capacity is impaired (e.g., significant psychiatric disturbance, the effect of the ingested substance on judgment), she cannot give or withhold valid consent, and emergency assessment is permissible under the doctrine of necessity. The Mental Healthcare Act 2017 decriminalised attempted suicide — she cannot be detained on criminal grounds. Allowing her to leave simply on the mother's consent is inadequate — the mother cannot override the patient's own right to consent/refuse care.
Managing Challenges: Relationship Management and Conflict Resolution
The clinician managing medico-legal cases will regularly encounter structured and unstructured pressures from multiple directions: families demanding outcomes, senior clinicians applying peer pressure, institutional administrators concerned about reputation, police demanding expedited reports, and media seeking comment. Developing a framework for navigating these pressures is a core professional skill.
Relationship management with patients and families:
Establishing rapport and trust with a patient in a highly charged medico-legal situation requires:
- Active listening: allow the patient to tell their story without interruption; demonstrate attentiveness through posture, eye contact, and reflective statements.
- Empathic acknowledgment: 'I understand this has been very frightening' before moving to the clinical examination.
- Transparent explanation: explain what you are about to do and why before each step; this preserves consent, reduces anxiety, and maintains trust.
- Boundary clarity: the clinician's role in an MLC case is defined — clinical examiner, documentarian, and referrer to support services. The boundaries of that role should be explained clearly to both patient and family.
Managing family pressure:
Families in acute distress frequently place unreasonable demands on the treating clinician — demanding information before it is available, demanding a specific clinical finding, or demanding that the police not be called. The clinician's response must be:
- Consistent: apply the legal framework consistently regardless of pressure.
- Empathic but firm: acknowledge the family's distress without agreeing to deviate from clinical or legal obligations.
- Documented: document requests and the clinician's response in the case notes.
Conflict resolution principles:
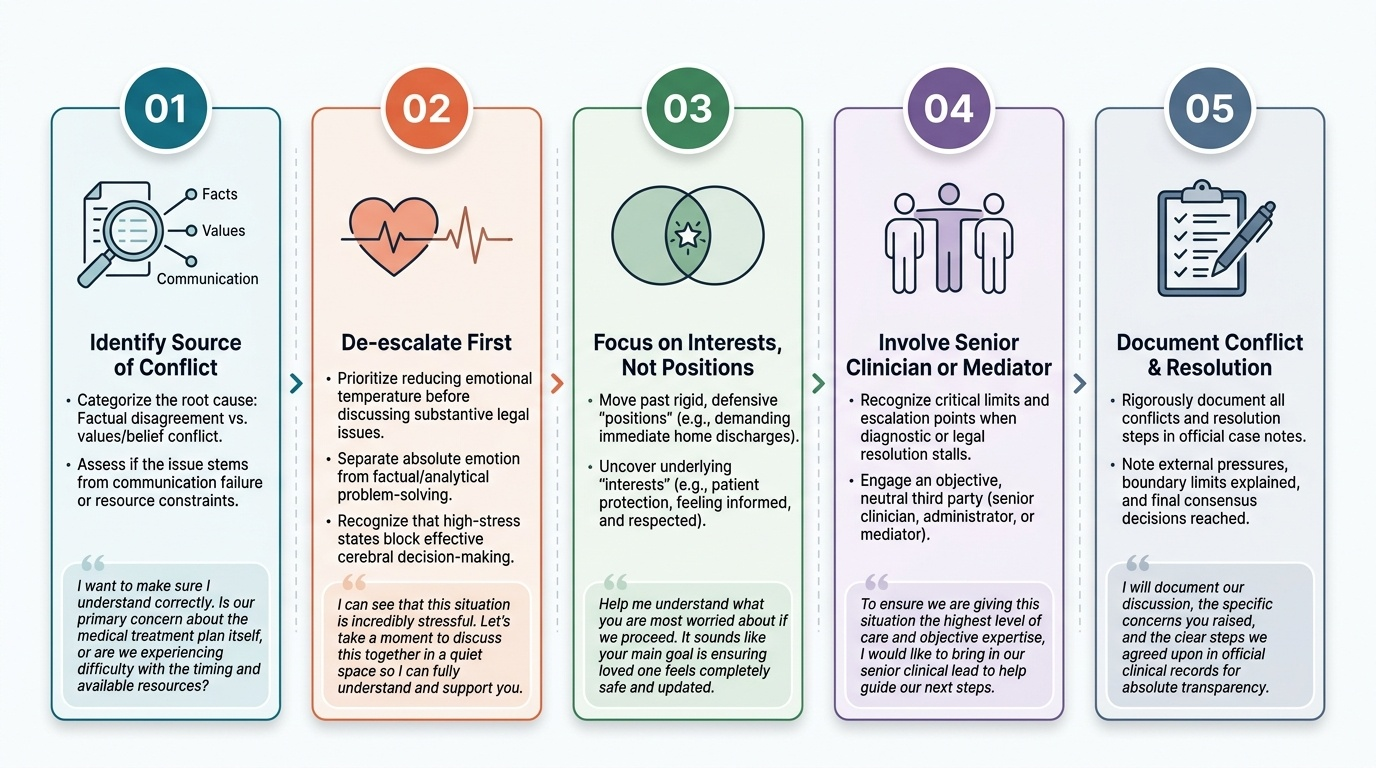
1. Identify the source of conflict: factual disagreement vs values conflict vs communication failure vs resource constraint. Different sources require different approaches.
2. De-escalation first: reduce emotional temperature before addressing substance — people in acute stress do not problem-solve effectively.
3. Focus on interests, not positions: 'The family wants the patient home' (position) vs 'The family wants their loved one to be safe and informed' (interest) — addressing the underlying interest is more effective.
4. Involve a senior clinician or mediator if direct de-escalation is not successful.
5. Document all conflict and its resolution in the case notes.
Provided image
CLINICAL PEARL
The three sentences every junior doctor must know for media encounters at the hospital: (1) 'I am not authorised to comment on individual patient cases.' (2) 'All media enquiries should be directed to [hospital spokesperson name and contact].' (3) 'I cannot provide any patient information without the patient's written consent and hospital authorisation.' These three sentences, delivered calmly and consistently, fulfil the clinician's legal obligations while managing the media interaction. Saying anything beyond this — however confident the clinician feels — opens a path to confidentiality breach, contempt of court in active cases, and professional complaints. Brevity and redirection are the correct tools.
Handling Pressure in MLCs: Applied Practice
Pressure in the medico-legal context is defined as an influence that attempts to cause the clinician to deviate from the legally and ethically mandated course of action in an MLC — to alter documentation, delay reporting, suppress findings, or provide a false certificate. Understanding the types, causes, and sources of pressure, and having pre-planned responses, is the foundation of managing it effectively.
Types and sources of pressure in MLC practice:
Professional/hierarchical pressure: A senior colleague or department head instructs the junior doctor to 'not make trouble' by registering an obvious assault case as an MLC, or to 'soften' the injury description. This is institutional pressure from within the profession. The correct response: politely decline, document the instruction received, and escalate to the hospital's medical superintendent or the NMC's ethics infrastructure. Falsifying an MLC record on instruction from a superior is not a defence — each clinician is individually responsible for the accuracy of their documentation.
Family/patient pressure: A patient's family applies emotional pressure ('please don't call the police — it will destroy the family') or financial inducement to suppress or alter findings. Emotional pressure is managed through empathic boundary-holding. Financial inducement is bribery — not only an ethical violation but a criminal offence under the Prevention of Corruption Act 1988.
Media and public pressure: High-profile cases attract public attention that can cause institutional anxiety and implicit pressure on clinicians to make findings consistent with public narrative. Clinical findings must be based on evidence, not public pressure or institutional reputation management.
Political and VIP pressure: When the accused or victim is politically connected, there may be direct or indirect political pressure on the examining or reporting clinician. This is the highest-risk scenario: clinicians who alter findings under political pressure face both criminal liability and career-ending professional consequences if discovered.
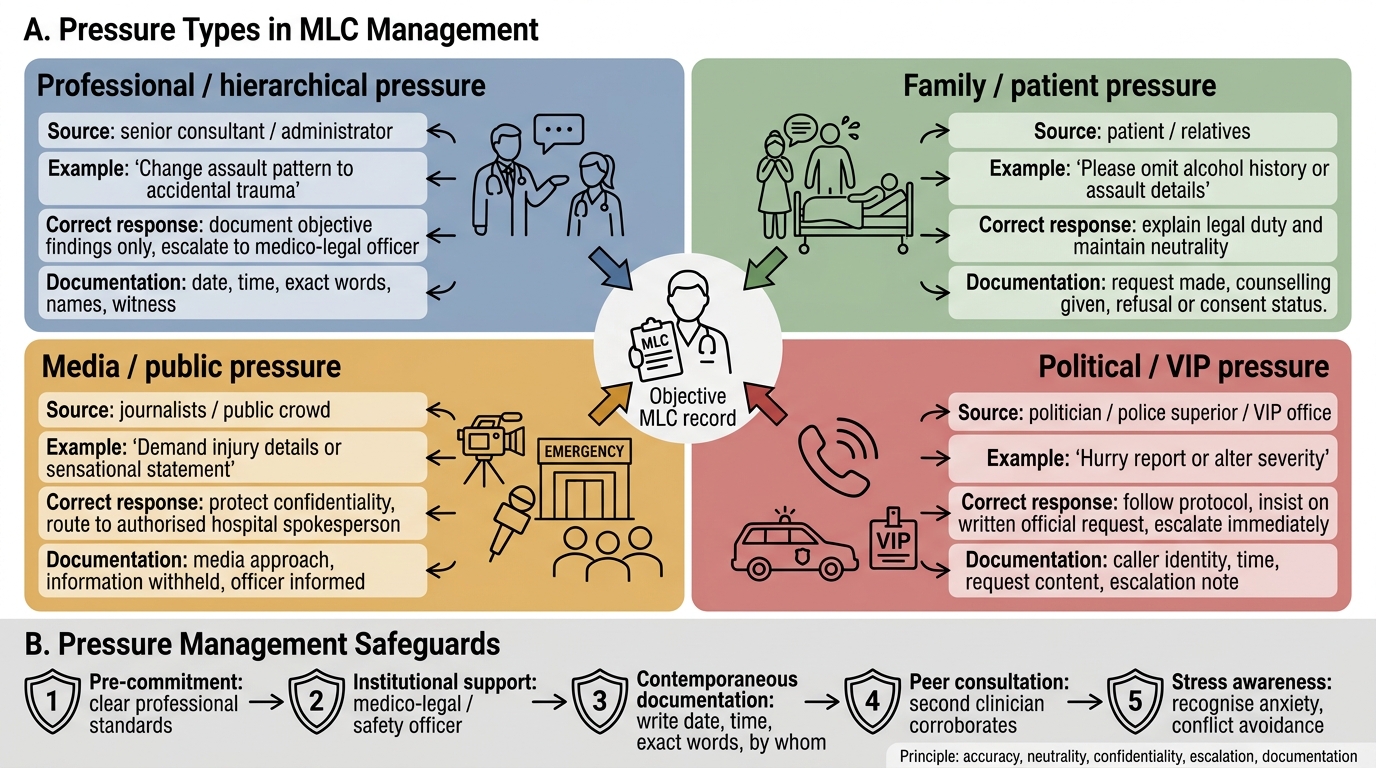
Pressure Types and Safeguards in MLC Management
Skills for dealing with pressure:
1. Pre-commitment: having clear personal professional standards before the pressure arrives makes it easier to maintain them under stress.
2. Institutional support: every hospital should have a designated medico-legal officer or safety officer to whom clinicians under pressure can immediately escalate.
3. Documentation contemporaneously: if pressure is being applied, write it down immediately in the case notes with date, time, and exactly what was said and by whom.
4. Peer consultation: a second clinician consulted contemporaneously provides independent corroboration of the findings and reduces vulnerability to subsequent challenges.
5. Awareness of stress responses: the clinician's own anxiety, compassion fatigue, and conflict avoidance responses can cause subtle deviations from best practice. Recognising one's own stress response is the first step to managing it.
SELF-CHECK
A senior surgeon requests that a junior doctor document a road accident victim's injuries as 'consistent with accidental trauma' when the injury pattern — including a defensive laceration on the forearm and a periorbital haematoma — is clearly inconsistent with the stated mechanism and suggests assault. The surgeon says, 'The family are important people. Don't make this a problem.' What is the junior doctor's CORRECT response?
A. Comply with the senior surgeon's request to maintain professional hierarchy
B. Document the injuries accurately as an MLC with a note of the mechanism inconsistency; decline to alter documentation even under senior pressure
C. Document 'accidental' but privately inform the police without documenting this action
D. Refer the patient to another hospital to avoid the conflict
Reveal Answer
Answer: B. Document the injuries accurately as an MLC with a note of the mechanism inconsistency; decline to alter documentation even under senior pressure
Each clinician bears individual legal and professional responsibility for the accuracy of their clinical documentation. Altering findings on the instruction of a senior is not a defence — it is professional misconduct and potentially a criminal act (falsification of medical records). The correct approach is to document the injuries accurately as an MLC, note the mechanism inconsistency in precise clinical terms, inform police per mandatory obligation, and if the pressure persists, document that the instruction was given (who said it, when, in what words) in the case notes and escalate to the medical superintendent. 'I was following orders' is not a professional protection.
KEY TAKEAWAYS
Communication with media: all patient-specific media enquiries are redirected to the hospital spokesperson; the clinician never discloses patient information to media without written consent; sub-judice cases require particular care. Communication with police: share factual clinical findings; produce records only on lawful authority; do not allow police during examination without patient consent. Social aspects of MLC cases: survivors of rape, assault, attempted suicide, domestic violence, and homicide have specific psychosocial needs that must be addressed alongside legal documentation — survivor-centred examination for rape, capacity assessment for attempted suicide, structured bereavement support for homicide families. Relationship management: active listening, empathic acknowledgment, boundary clarity, and documented conflict resolution. Types of pressure: professional/hierarchical, family, media, political — managed through pre-commitment, contemporaneous documentation, peer consultation, and escalation. Altering documentation under any pressure is professional misconduct and potentially criminal. Mental Healthcare Act 2017 decriminalised attempted suicide; assess capacity, not criminal culpability, in these cases.
REFLECT
Think about a situation — real or imagined — in which you faced pressure from a senior colleague or family member to do something professionally sub-optimal. How did it feel? What did you do? Now revisit that scenario through the lens of this SDL: what were the sources of your discomfort? What would the 'pre-committed clinician with clear standards' have done? Develop a personal policy — one or two sentences — on how you will respond when institutional or family pressure conflicts with your medico-legal obligations. Write it down and revisit it at the end of your house officer year.