Page 13 of 18
FM10.9 | Human Rights, Family Violence & NHRC — SDL Guide
Learning Objectives
- Define human rights in the context of medical practice and medico-legal obligations
- Describe the mandate and powers of the National Human Rights Commission (NHRC) of India
- Identify the categories of human rights violations that involve doctors and healthcare institutions
- Explain the medico-legal framework for family violence — definitions, mandatory obligations, and documentation
- Apply the principles of human rights and anti-discrimination to clinical practice
INSTRUCTIONS
Human rights frameworks have become increasingly central to medical law and ethics. The NHRC has jurisdiction over healthcare-related human rights violations, and doctors frequently encounter victims of family violence whose medico-legal care requires specific knowledge and precise documentation. FM10.9 addresses both the institutional rights framework and the clinical front-line obligations.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A woman is brought to the emergency department with multiple contusions, a fractured radius, and cigarette burns on her forearms. She says she fell down the stairs. The junior doctor on duty notes the injury pattern is inconsistent with the given history — the burns are in different stages of healing, suggesting repeated injury, and the fracture pattern is high-force, inconsistent with a domestic fall. Her husband waits outside and has spoken to the nursing staff.
The junior doctor is uncertain: is there a legal obligation to report this? Can the patient be detained for her own safety? Who in the hospital should be involved? And is documenting a 'fall' in the case notes when injury pattern suggests assault a form of professional misconduct?
This scenario sits at the intersection of family violence, human rights, and the clinician's medico-legal obligations.
WHY THIS MATTERS
India has among the world's highest rates of reported domestic violence — the National Family Health Survey-5 (NFHS-5, 2019–2021) found that approximately 30% of ever-married women aged 15–49 reported experiencing spousal physical, sexual, or emotional violence. Healthcare settings are often the first and sometimes only point of contact for survivors of family violence before legal intervention occurs. Simultaneously, the National Human Rights Commission (NHRC) receives thousands of health-related human rights complaints annually — many involving custodial deaths, police encounters, and sub-standard care in public hospitals. Doctors are both potential agents of rights protection and potential subjects of NHRC scrutiny.
RECALL
Recall prior FM learning:
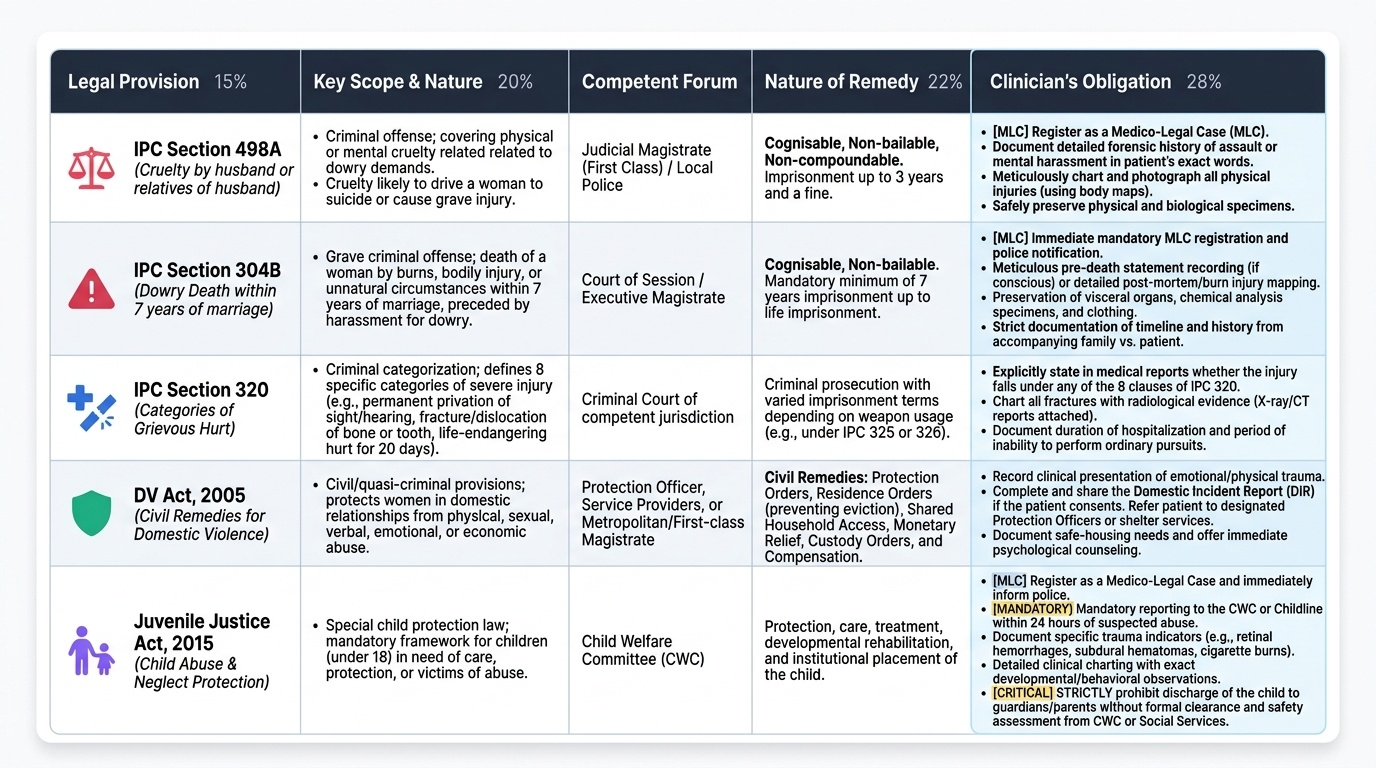
- IPC 319–321 — simple hurt (bodily pain without endangering life or causing grievous hurt) vs grievous hurt (eight categories: emasculation, eye damage, ear damage, loss of any member/joint, destruction of any member/joint, permanent disfigurement of head/face, fracture/dislocation of bone/tooth, hurt endangering life or causing severe bodily pain for 20+ days). The distinction is medico-legally critical for charge framing.
- Protection of Women from Domestic Violence Act 2005 (DV Act) — civil law providing protection orders, residence orders, and compensation orders for victims of domestic violence.
- Medico-legal case (MLC) — any case where the injury or condition may have been caused by a criminal or legal act; requires specific documentation and police intimation.
- Wound classification — abrasion, contusion, laceration, incised wound, firearm wound. See FM wound classification SDL.
Human Rights in Medicine: Legal and Professional Context
Human rights are fundamental entitlements held by every individual by virtue of their humanity — irrespective of nationality, ethnicity, gender, religion, or legal status. In the medical context, the human rights most directly implicated are: the right to life (Article 21 of the Constitution); the right to health as an aspect of the right to life and dignity; the right to equality and non-discrimination (Articles 14–15); the right to personal liberty (Article 21); and the right to be free from torture and cruel, inhuman, or degrading treatment (a customary international law norm, reflected in India's constitutional jurisprudence).
Human rights violations in healthcare settings that engage doctor's professional obligations include:
- Sub-standard care in government hospitals that leads to preventable deaths.
- Denial of treatment to marginalised groups (homeless persons, prisoners, undocumented migrants).
- Non-consensual medical procedures (sterilisation without consent, forced psychiatric detention, compulsory HIV testing).
- Custodial medical neglect — failure to provide adequate medical care to prisoners, detainees, or persons in state custody.
- Failure to document and report injuries in medico-legal cases, which may impede the victim's access to justice.
- Discrimination in care based on caste, religion, gender, or HIV status.
The Constitutional framework: Under Article 21 (right to life), the Supreme Court has held that the right to health is implicit in the right to life. The State has an obligation to ensure adequate healthcare, and a government doctor's negligent failure to provide emergency care may constitute a constitutional rights violation, actionable under Article 32 or Article 226 (writ jurisdiction of courts), in addition to negligence claims under civil law or Consumer Protection Act 2019.
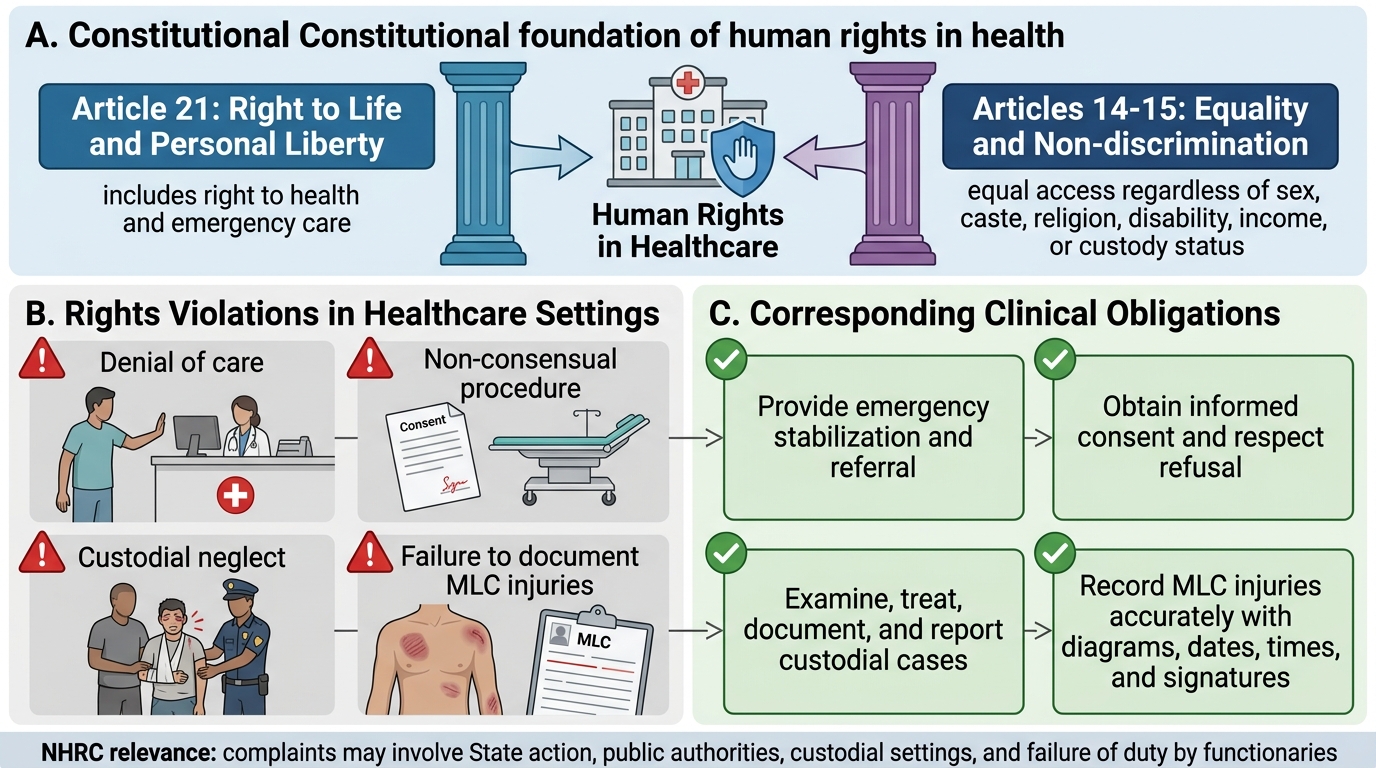
Constitutional Basis of Human Rights in Healthcare
National Human Rights Commission (NHRC): Governing Principles
The National Human Rights Commission (NHRC) was established under the Protection of Human Rights Act 1993 (PHRA 1993). It is a quasi-judicial statutory body that investigates complaints of human rights violations by the State and its functionaries. Understanding the NHRC's jurisdiction, powers, and the types of cases it handles is directly relevant to FM10.9.
Constitution of the NHRC:
- Chairperson: a retired Chief Justice of India.
- Members: two members who are retired Judges of the Supreme Court, and two members with experience in human rights matters.
- Deemed members: the chairpersons of the National Commission for Minorities, National Commission for SC/ST, National Commission for Women, and National Commission for Backward Classes are deemed members ex officio.
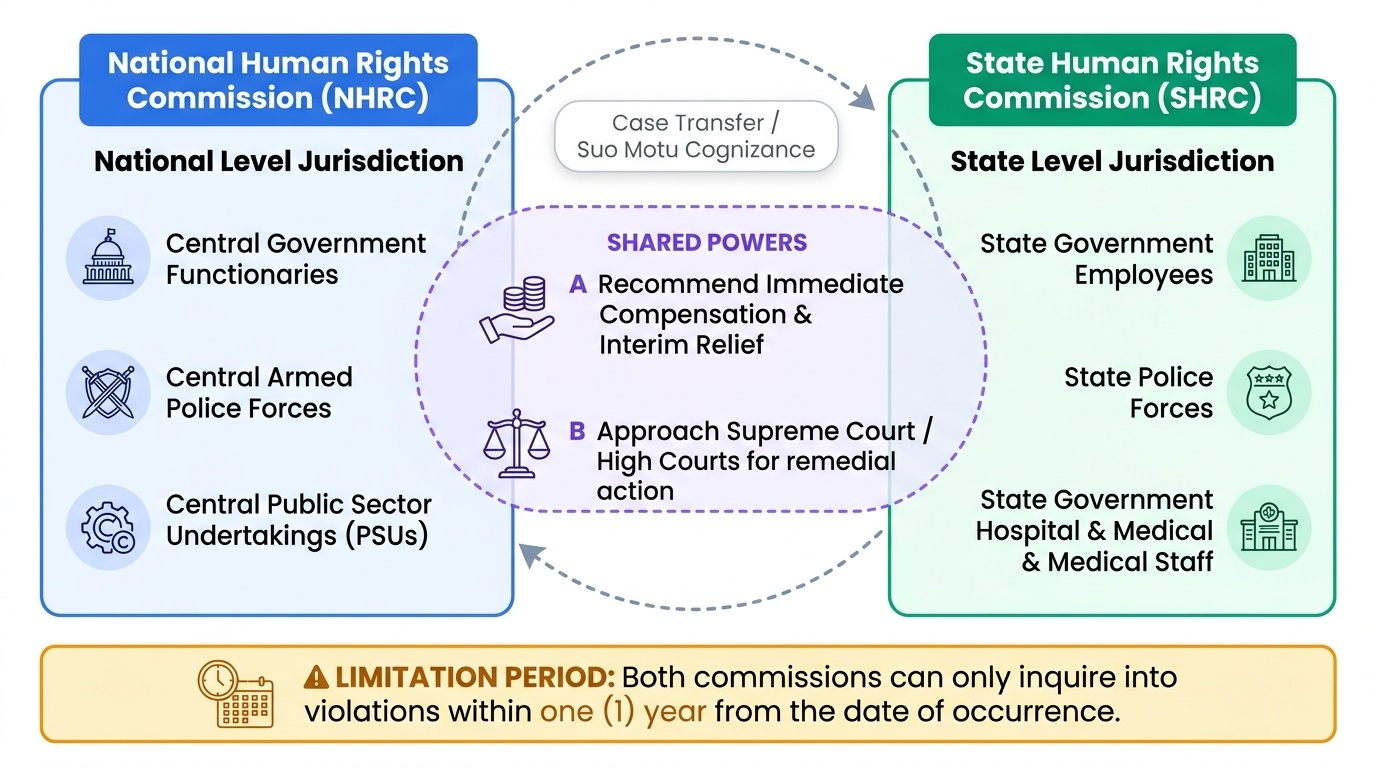
Jurisdiction of the NHRC:
The NHRC has jurisdiction over violations of human rights committed by: (a) officers of the central government, (b) officers of any central public sector undertaking, and (c) any person acting under the Central Government or a Central Armed Police Force. For state-level violations (including state government hospitals), the complaint must generally go to the State Human Rights Commission (SHRC) (where constituted) or the NHRC may transfer state complaints.
Healthcare-related NHRC jurisdiction:
The NHRC has taken cognizance of numerous health-related rights violations:
- Custodial deaths and injuries in police/prison custody — the NHRC investigates and recommends compensation to families; the Medical Officer who performed the post-mortem must be independent.
- Suomotu cognizance of mass casualty events in government hospitals (e.g., neonatal deaths, contaminated drugs).
- Medical negligence in government hospitals that constitutes a human rights violation.
- Violation of rights of psychiatric patients in government institutions.
Powers of the NHRC:
The NHRC can: (a) investigate complaints of human rights violations; (b) examine government reports and records; (c) visit any government institution under the control of the State (including jails and hospitals); (d) recommend payment of immediate interim relief; (e) approach the Supreme Court or High Courts to direct the State to take remedial action; and (f) review constitutional and legal safeguards. The NHRC does NOT have the power to prosecute or impose criminal punishment — its recommendations are directed to the government, which is expected to comply. Non-compliance may lead to court enforcement.
Limitation for NHRC complaints: Generally, complaints must be filed within 1 year of the alleged violation, though this may be condoned in exceptional circumstances.
Provided image
SELF-CHECK
The National Human Rights Commission (NHRC) receives a complaint about a patient death due to alleged negligence in a state government medical college. Which body has PRIMARY jurisdiction over this complaint?
A. The NHRC has direct jurisdiction over all state government hospital complaints
B. The State Human Rights Commission (SHRC) of the relevant state has primary jurisdiction
C. The case must go directly to the Supreme Court under Article 32
D. The Consumer Protection National Commission has jurisdiction
Reveal Answer
Answer: B. The State Human Rights Commission (SHRC) of the relevant state has primary jurisdiction
Under the Protection of Human Rights Act 1993, the NHRC has jurisdiction over violations by officers of the Central Government and central undertakings. For violations by state government functionaries (including state government hospital employees), the primary jurisdiction lies with the State Human Rights Commission (SHRC) of the relevant state. The NHRC may take cognizance in the absence of a functional SHRC or in matters of national importance, but SHRC is the correct first forum for state hospital matters.
Family Violence: Documentation and Medico-Legal Procedure
Family violence (also termed domestic violence or intimate partner violence) encompasses physical, sexual, emotional, and economic abuse perpetrated within a domestic or intimate relationship. In the Indian legal framework, it is primarily governed by the Protection of Women from Domestic Violence Act 2005 (DV Act 2005) — a civil statute — alongside criminal provisions of the IPC for specific offences (assault under IPC 351, grievous hurt under IPC 320, dowry-related offences under IPC 304B and Section 498A, sexual assault under IPC 375–376).
Recognition of family violence presentations:
Clinicians must maintain a structured suspicion index for family violence, particularly in presentations with:
- Injury patterns inconsistent with the given mechanism (the hook scenario's fracture and burn pattern).
- Multiple injuries at different stages of healing, indicating a pattern of repeated trauma.
- Delayed presentation — a patient who comes to hospital days after an injury without a convincing explanation.
- Presence of a controlling companion who answers for the patient and requests to be present during examination.
- Minimising language and behavioural cues (avoidance of eye contact, fearfulness, vague recounting of events).
Medico-legal obligations in family violence cases:
Family violence cases presenting with physical injury are medico-legal cases (MLCs) and impose specific obligations on the treating clinician:
1. Documentation: record the history in the patient's own words (verbatim wherever possible) in quotation marks. Document all injuries systematically — site, size, shape, margins, colour, age, and possible causative object for each wound. Photographs (with consent) are valuable corroborating evidence.
2. Police intimation: the treating doctor has a legal duty to inform the police when injuries suggest assault, under the provisions of the Code of Criminal Procedure (CrPC) Section 39 (public duty to provide information of offences). The DV Act 2005 also creates a duty for service providers (including healthcare providers) who encounter domestic violence to inform the Protection Officer.
3. Independence from the accompanying person: the clinician must assess and document the history from the patient alone, without the alleged perpetrator present. This is both an ethical obligation and a practical necessity — history taken in the presence of the abuser is unreliable and may put the patient at risk.
4. Referral and safety planning: following documentation and police intimation, the patient should be referred to a social worker, counsellor, or the designated Protection Officer under the DV Act 2005, who can assist with protection orders, shelter, and legal support.
Protection of Women from Domestic Violence Act 2005:
The DV Act is a civil statute providing fast-track non-criminal remedies for domestic violence survivors. Key provisions:
- Protection orders: prohibit the respondent from committing further acts of domestic violence, entering the shared household, or contacting the victim.
- Residence orders: permit the victim to continue residing in the shared household or secure alternative accommodation.
- Compensation orders: monetary compensation for physical and emotional harm.
- Protection Officers: designated government officials who assist complainants, file domestic incident reports, and coordinate with police and medical services. Healthcare providers are expected to cooperate with Protection Officers.
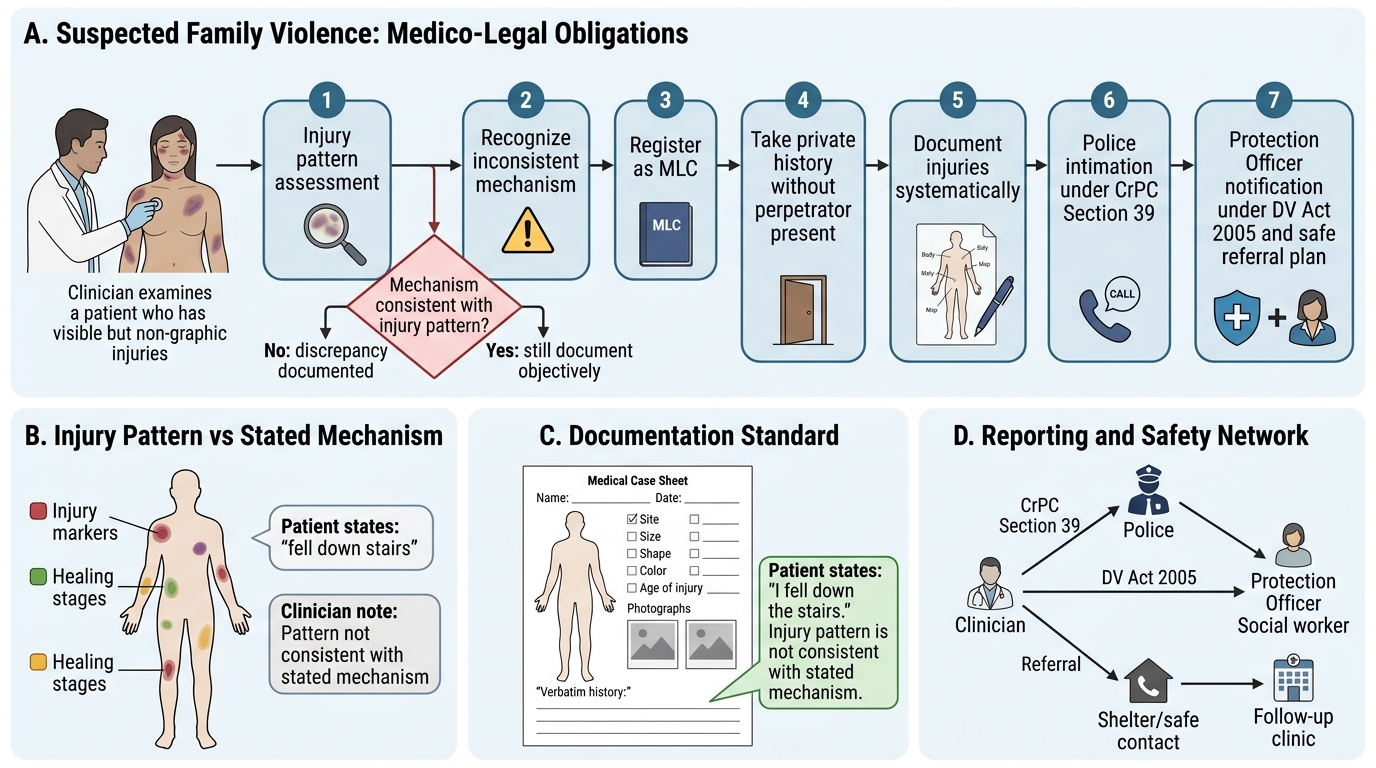
Medico-Legal Flowchart for Suspected Family Violence
CLINICAL PEARL
Never document a false history: If the clinician's clinical judgment (based on injury pattern, healing stages, biomechanics) indicates the stated mechanism is inconsistent with the injuries, the case notes must reflect this discrepancy. Writing 'patient fell down stairs' when the injury pattern is clearly inconsistent with that mechanism — because the patient or accompanying person insists on it — is at minimum poor documentation and at worst an act that obstructs justice. The correct documentation is: 'Patient states she fell down the stairs. The injury pattern (cigarette burns in multiple healing stages + high-force radius fracture) is not consistent with the stated mechanism. A medico-legal case has been registered and police informed.' This protects the patient's access to justice and protects the clinician from later accusations of cover-up.
Applied Practice: Managing Specific Human Rights and Family Violence Scenarios
The practical management of human rights violations and family violence in clinical settings requires the clinician to apply the legal framework systematically while maintaining the therapeutic relationship with the patient. The following worked examples address the most frequently encountered scenarios.
Scenario 1 — Prisoner with inadequate medical care:
A prisoner is brought to the emergency department having been in custody for 72 hours with an untreated open fracture. This constitutes (a) a medico-legal case, and (b) a potential human rights violation (denial of necessary medical care in custody). The clinician's obligations are: (a) treat the medical emergency; (b) document injuries meticulously including the history of delayed presentation in custody; (c) record the findings relevant to the human rights concern in the notes; (d) inform the hospital's medico-legal officer; (e) a complaint to the NHRC or SHRC is the appropriate channel for the human rights violation (denial of timely care).
Scenario 2 — Child brought in with suspicious injuries:
A 4-year-old child is brought in with bilateral retinal haemorrhages and subdural haematoma. The parents say the child fell from a cot. This presentation is a classic pattern of non-accidental injury (shaken baby syndrome). The clinician must: (a) treat the child; (b) register as MLC and inform police; (c) inform the Child Welfare Committee (CWC) under the Juvenile Justice (Care and Protection of Children) Act 2015 — this is a mandatory reporting obligation for suspected child abuse; (d) document in detail; (e) NOT allow the child to be discharged to the parents without social services assessment.
Scenario 3 — Victim of dowry harassment:
A woman with evidence of assault and burns presents with a history of dowry demands. IPC Section 498A (cruelty by husband or relatives to compel property demand) and Section 304B (dowry death — death within 7 years of marriage in suspicious circumstances with evidence of dowry harassment) are the relevant criminal provisions. The clinician must document injuries, inform police, and be aware that Section 498A is a cognisable, non-bailable offence — police must register the FIR on receipt of information.
Scenario 4 — Refusal to document MLC:
A senior colleague asks a junior doctor to document a family violence case as an 'accidental injury' to avoid 'trouble.' Doing so is unprofessional conduct, potentially a criminal offence (falsification of records, abetment of concealment), and a human rights violation — it denies the victim access to justice. The junior doctor's obligations under the NMC Code of Ethics require accurate documentation. The correct response is to refuse, document accurately, and if pressured, escalate to the medical superintendent or the State Medical Council.
Provided image
SELF-CHECK
A woman with injuries consistent with domestic violence presents to the emergency department. She tells you privately she is afraid to report it. What is the doctor's MANDATORY legal obligation under Indian law?
A. Respect her wish and document 'accidental injury' to avoid police involvement
B. Admit her to the hospital without her consent for her own safety
C. Inform the police of the suspected offence under CrPC Section 39 and ensure the injuries are documented as an MLC
D. Report only to the Protection Officer under the DV Act and not the police
Reveal Answer
Answer: C. Inform the police of the suspected offence under CrPC Section 39 and ensure the injuries are documented as an MLC
Under CrPC Section 39, any person (including a doctor) who has knowledge of an offence has a public duty to inform the police. Physical assault constitutes a cognisable offence, and a doctor encountering injuries consistent with assault must register an MLC and inform the police — this is a legal obligation, not a discretionary decision. The patient's fear or wish not to report does not override the doctor's legal duty to report. The doctor should sensitively counsel the patient about the process, arrange support (social worker, Protection Officer under DV Act 2005), and ensure her safety, but documentation and police information are mandatory.
KEY TAKEAWAYS
Human rights in medicine derive from Article 21 (right to life and dignity) and apply to all State-provided healthcare; violations include denial of care, non-consensual procedures, and custodial medical neglect. The NHRC (est. Protection of Human Rights Act 1993) has jurisdiction over Central Government violations; SHRC handles state-level violations; NHRC can recommend compensation and approach courts. Family violence is governed by the DV Act 2005 (civil remedies: protection, residence, compensation orders) and IPC (498A dowry cruelty, 304B dowry death, 320 grievous hurt). Clinical obligations: document injuries in detail with verbatim history in quotation marks, note mechanism inconsistencies, register as MLC, inform police under CrPC Section 39, refer to Protection Officer and social services. Never falsify a clinical record to conceal assault — this is professional misconduct and potential criminal liability. Child abuse requires additional notification to the Child Welfare Committee under the JJ Act 2015.
REFLECT
Imagine you are the junior doctor in the hook scenario. The nurse tells you the patient's husband is demanding to be present during the examination and is asking what treatment she is receiving. The patient looks scared when told this. Think through each step: how do you secure a safe examination environment? What do you document, in what words, about the injury pattern? How do you handle the husband? Who do you inform and in what order? Reflect on how the legal framework — medico-legal case registration, CrPC Section 39, DV Act 2005 — gives you not just the obligation but also the authority to act in the patient's interest even when she is unable to advocate for herself.