Page 12 of 18
FM10.7 | HIV/AIDS Act: Ethics & Legal Aspects — SDL Guide
Learning Objectives
- Describe the key provisions of the HIV and AIDS (Prevention and Control) Act 2017
- Explain the rights of persons living with HIV (PLHIV) under the Act
- Apply the principles of confidentiality, non-disclosure, and anti-discrimination in the clinical context
- Identify the legal exceptions to non-disclosure of HIV status
- Discuss the ethical dilemmas arising from HIV testing, treatment refusal, and partner notification
INSTRUCTIONS
HIV infection remains stigmatised, criminalised by social prejudice, and subject to discrimination in healthcare settings. The HIV and AIDS (Prevention and Control) Act 2017 is India's landmark legislation that codifies the rights of persons living with HIV and creates legal obligations for healthcare providers. Understanding this Act is mandatory knowledge for every practising clinician in India.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 32-year-old schoolteacher is admitted for an elective surgical procedure. Pre-operative HIV testing (performed without her prior consent as part of a routine pre-operative screen) reveals she is HIV-positive. She is unaware of her status. The surgeon informs the hospital administrator and a ward nurse, and the patient's file is labelled prominently with an 'HIV+' sticker visible to all. The teacher's employer — the school principal — later contacts the hospital to enquire about her health status.
How many violations of the HIV and AIDS (Prevention and Control) Act 2017 has the hospital already committed? What are the legal consequences? And what should the correct clinical and ethical response have been at each decision point?
WHY THIS MATTERS
India has approximately 2.4 million persons living with HIV — the third-largest epidemic in the world. HIV-positive individuals in India face systematic discrimination in healthcare (refusal of treatment, sub-standard care, involuntary disclosure), employment, housing, and community life. The HIV and AIDS (Prevention and Control) Act 2017 is the first comprehensive anti-discrimination HIV law in India. It was enacted after decades of advocacy and creates a legally enforceable rights framework with penalties for violations. For every clinician, the Act defines specific obligations around testing, disclosure, confidentiality, and anti-discrimination that are regulatory requirements, not aspirational guidelines.
RECALL
Recall relevant prior knowledge:
- Informed consent — the legal requirement for voluntary, informed agreement before any medical intervention (SDL ml3). HIV testing is a medical intervention and requires informed consent.
- Confidentiality — the obligation to keep patient information private; part of medical ethics since the Hippocratic Oath. Codified in the NMC Code of Ethics.
- Stigma and discrimination — HIV stigma drives people away from testing and treatment; legal frameworks that protect against discrimination are public health tools as well as rights instruments.
- Public health obligations — tension between individual privacy and the duty to prevent disease transmission to third parties; one of the oldest ethical tensions in public health.
HIV and AIDS (Prevention and Control) Act 2017: Legal Context
The HIV and AIDS (Prevention and Control) Act 2017 (HIV Act 2017) was enacted by the Government of India and came into force in September 2018. It is a comprehensive statute that simultaneously addresses prevention, anti-discrimination, rights protection, and healthcare access for persons living with HIV (PLHIV). The Act applies across India and supersedes any inconsistent state law.
Core legal framework of the HIV Act 2017:
The Act establishes that every person has the right to live with HIV with dignity, free from discrimination and stigma. It recognises that HIV is a public health matter that requires both prevention of transmission AND protection of individual rights — a dual mandate that earlier AIDS control efforts had not adequately codified.
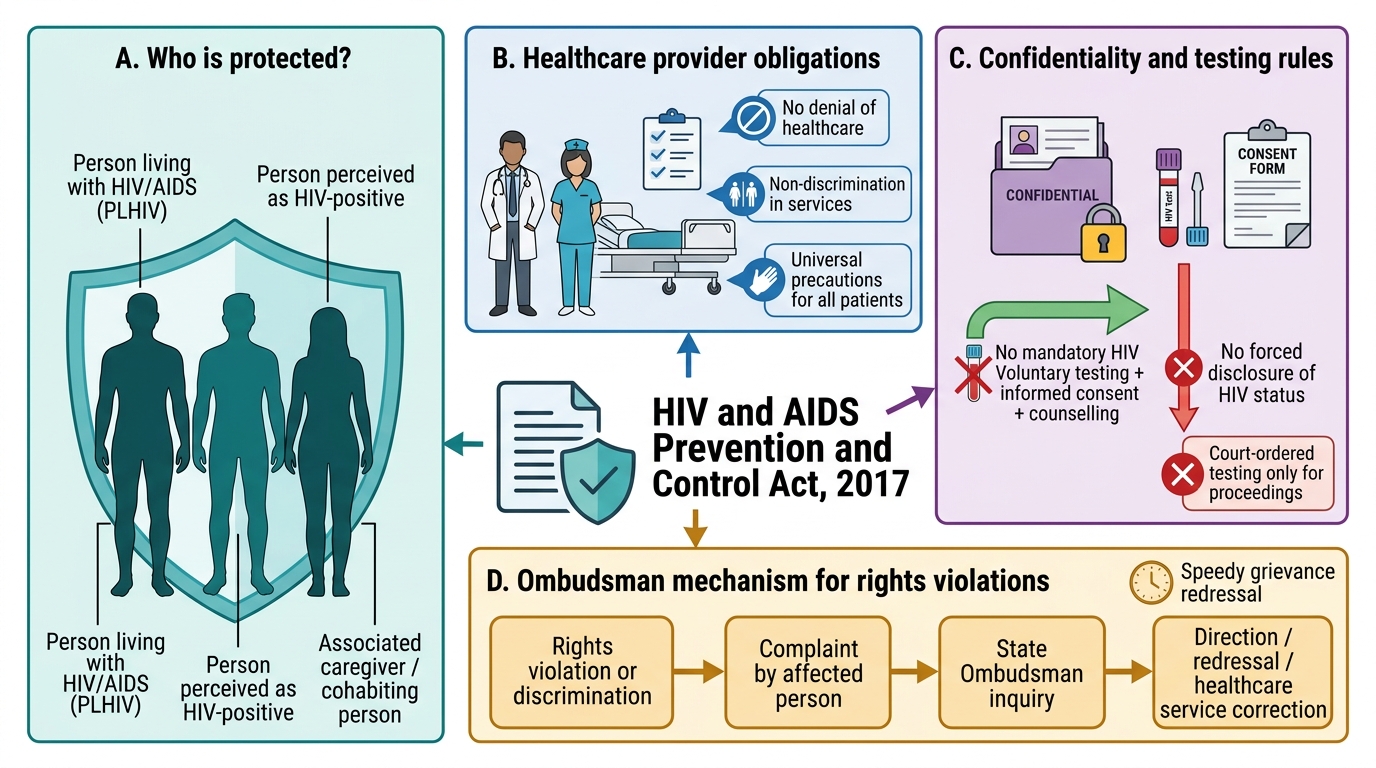
Who is protected: 'Protected persons' under the Act include (a) persons living with HIV, (b) persons who are perceived to be HIV-positive regardless of actual status, and (c) persons associated with or caring for PLHIV (family members, caregivers, partners). This broad definition ensures that stigma-by-association is also a punishable discrimination.
Healthcare provider obligations under the HIV Act 2017:
- Every healthcare provider (hospital, clinic, individual practitioner) must provide HIV testing and treatment services without discrimination.
- Refusal of treatment, or provision of sub-standard treatment, to a person solely on the basis of their HIV status is an offence under the Act.
- Universal precautions for infection control must be observed — the Act prohibits requiring HIV testing as a precondition for surgery or any other healthcare service.
The Ombudsman mechanism: The Act establishes an HIV/AIDS Ombudsman in each state to receive and address complaints of discrimination or rights violations related to HIV. This is a specific, accessible redressal mechanism distinct from consumer forums or courts.
HIV and AIDS Prevention and Control Act, 2017: Rights and Duties Framework
Confidentiality, Testing, and Non-Disclosure Principles
The right to confidentiality of HIV status is one of the most important protections in the HIV Act 2017, and its provisions are stricter than the general medical confidentiality obligation. HIV status occupies a special category of sensitive health information because its disclosure, unlike most other diagnoses, carries risk of discrimination, violence, relationship breakdown, and loss of livelihood.
No mandatory HIV testing: The Act explicitly prohibits mandatory HIV testing. No person can be required to undergo HIV testing as a precondition for: (a) receiving healthcare, surgery, or any medical service; (b) employment, promotion, or appointment; (c) education, admission, or any public entitlement; (d) any other purpose specified in the First Schedule. Testing may only be conducted after obtaining the person's informed consent — this means the same pre-test counselling and voluntary agreement standard as for any other medical procedure.
Exception: Court-ordered testing. HIV testing without the person's consent may be ordered only by a court of competent jurisdiction for the purpose of proceedings before it. Even then, the result remains subject to confidentiality obligations and may only be used for the specific court purpose.
Strict prohibition on non-consensual disclosure:
Section 10 of the HIV Act 2017 prohibits any person who has obtained knowledge of a person's HIV status (whether as a healthcare provider, employer, insurance agent, or official) from disclosing that information to any third party without the explicit written consent of the person concerned. This prohibition is absolute with one exception: a court order.
The exceptions to non-disclosure under the Act are narrow:
1. Written consent of the PLHIV to disclosure.
2. Court order directing disclosure for specific legal proceedings.
Notably, the HIV Act 2017 does NOT create a general duty for clinicians to inform sexual partners of a patient's HIV status (unlike the law in some other jurisdictions). The public health approach adopted in the Act is to encourage voluntary disclosure through counselling rather than mandatory partner notification.
Pre- and post-test counselling: The Act mandates that HIV testing be accompanied by pre-test counselling (explaining the purpose, implications of a positive/negative result, confidentiality, voluntary nature) and post-test counselling (disclosure of results, support, treatment navigation). These are not optional add-ons — they are part of the legally required testing process.

HIV Status Disclosure Decision Tree Under HIV Act 2017
SELF-CHECK
A doctor treats an HIV-positive patient. The patient's wife contacts the doctor privately to ask whether her husband has HIV. Under the HIV and AIDS (Prevention and Control) Act 2017, what is the doctor's CORRECT response?
A. Disclose the patient's status to the wife because she is a third party at risk
B. Disclose the status to the wife because there is a public health duty to prevent HIV transmission
C. Decline to disclose — the patient's HIV status cannot be shared without his written consent or a court order
D. Refer the wife to the State AIDS Control Society
Reveal Answer
Answer: C. Decline to disclose — the patient's HIV status cannot be shared without his written consent or a court order
Section 10 of the HIV Act 2017 prohibits disclosure of a person's HIV status to any third party without their explicit written consent or a court order. The wife — despite being a potential contact — does not meet either exception. The Act does not create a general partner-notification duty for clinicians. The correct approach is to decline disclosure, counsel the patient about his responsibility to disclose to his partner, and provide support for voluntary disclosure. Referring her to the AIDS Control Society without disclosing the patient's status may be appropriate for general HIV counselling and testing.
Anti-Discrimination Provisions and Rights of PLHIV
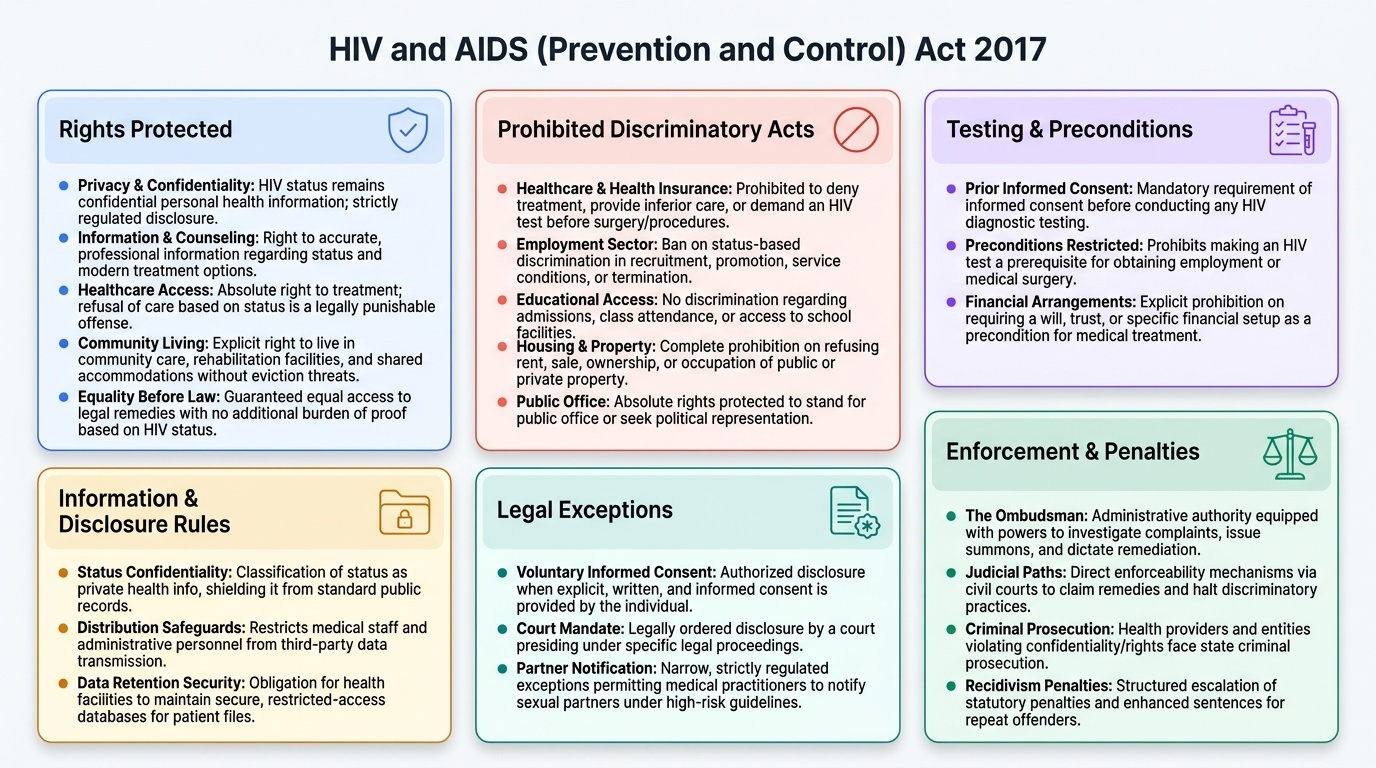
The anti-discrimination provisions of the HIV Act 2017 are among its most practically important sections for healthcare settings. Section 3 of the Act prohibits discrimination against PLHIV in a wide range of settings, and the prohibitions are directly enforceable through the Ombudsman mechanism and courts.
Prohibited discriminatory acts under the HIV Act 2017:
No person shall, on the grounds of HIV status, discriminate against a protected person in:
- Healthcare and health insurance (including demanding an HIV test before surgery, denying treatment, providing inferior care).
- Employment (recruitment, promotion, service conditions, termination).
- Education (admission, attendance, access to facilities).
- Housing and public or private property.
- Standing for public office.
- Requiring a will, trust, or financial arrangement as a precondition for treatment.
Rights of PLHIV under the Act:
- Right to privacy: HIV status is confidential personal health information; its disclosure is strictly regulated.
- Right to information and counselling: the right to accurate information about their HIV status and treatment options.
- Right to access healthcare: no healthcare provider may refuse treatment solely on the basis of HIV status; refusal is a punishable offence.
- Right to live in community care settings: persons with HIV cannot be evicted from community care facilities, rehabilitation centres, or shared accommodation solely on the basis of their HIV status.
- Right to equality before law: equal access to legal remedies; no additional burden of proof imposed solely because of HIV status.
Penalties for violations: The HIV Act 2017 prescribes penalties for various offences — persons who commit prohibited discriminatory acts can be prosecuted; healthcare providers who violate confidentiality face prosecution; repeat offenders face enhanced penalties. The Ombudsman has powers to investigate, summon, and recommend remediation.
Provided image
Applied Practice: Ethical Dilemmas in HIV Medicine
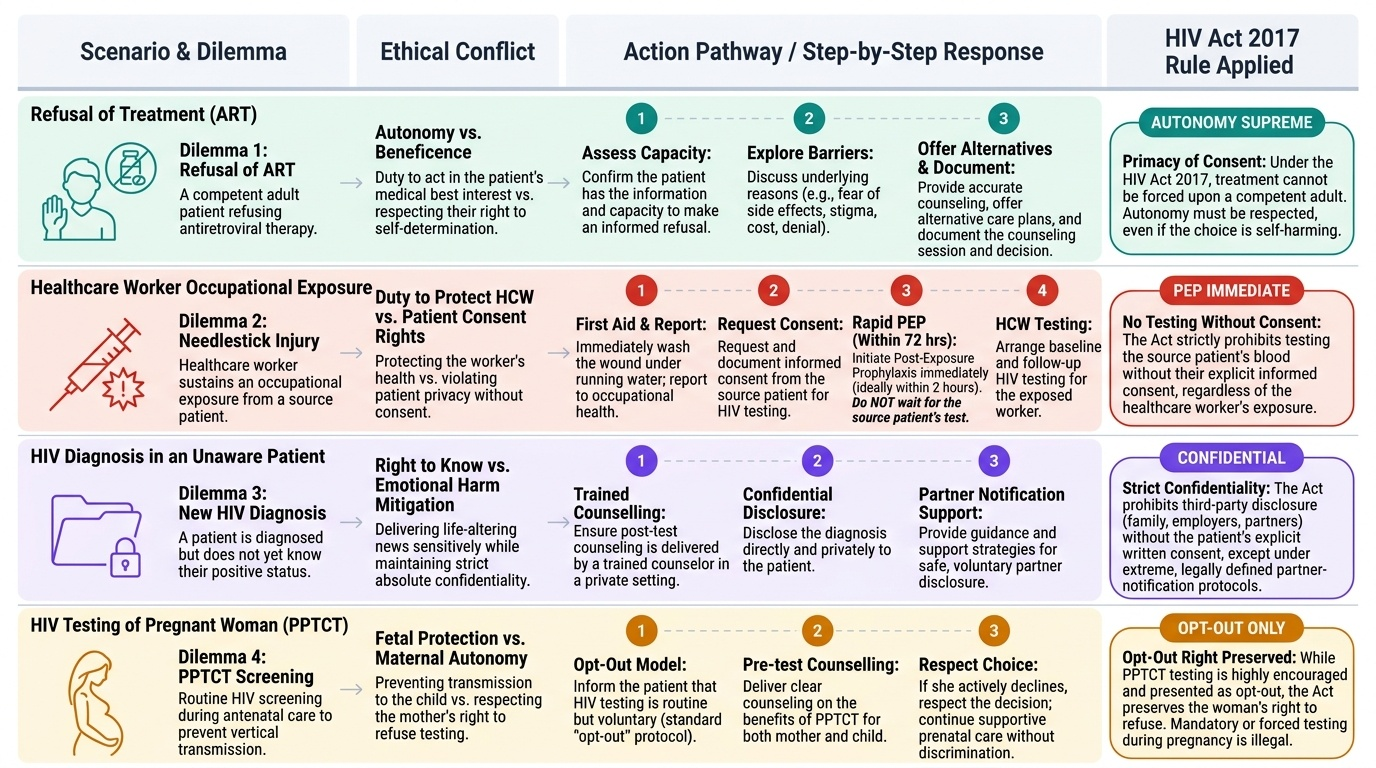
Managing HIV-positive patients in clinical practice generates a cluster of recurring ethical dilemmas that require a structured approach. These scenarios test the practitioner's ability to balance individual rights against public health obligations, the duty of confidentiality against the duty to prevent harm, and autonomy against beneficence.
Provided image
Dilemma 1 — Refusal of treatment by the patient:
An HIV-positive patient refuses antiretroviral therapy (ART). The clinician's obligations are: (a) ensure the patient has the information and capacity to make the decision; (b) explore the reasons for refusal — fear of side effects, stigma, denial, cost; (c) provide accurate counselling and offer alternatives; (d) respect the competent patient's autonomy, even if the decision is harmful to themselves. ART cannot be forced on a competent adult patient who refuses. Document the counselling and the patient's decision.
Dilemma 2 — Healthcare worker occupational exposure:
A healthcare worker sustains a needlestick injury from an HIV-positive patient. The Act's provisions apply: the source patient cannot be tested without consent simply because of the healthcare worker's concern. The correct pathway is: (a) immediately wash the wound; (b) report to occupational health; (c) seek and document informed consent for the source patient's HIV testing (or confirm known HIV status); (d) initiate post-exposure prophylaxis (PEP) within 72 hours (ideally within 2 hours) — do NOT wait for source patient's test result to begin PEP; (e) arrange baseline and follow-up testing for the healthcare worker.
Dilemma 3 — HIV diagnosis in a patient who does not know:
When HIV is first diagnosed (as in the hook scenario), the clinician must: (a) ensure a trained counsellor or the physician delivers the result in a private, supportive setting; (b) provide post-test counselling including the meaning of the result, treatment options, and support resources; (c) NOT disclose to family, employer, or any third party without the patient's written consent; (d) work with the patient over time to encourage voluntary disclosure to sexual partners.
Dilemma 4 — HIV testing of a pregnant woman:
Antenatal HIV testing is strongly recommended and often provided as an opt-out test under the PPTCT (Prevention of Parent-to-Child Transmission) programme. The woman retains the right to decline. Opt-out testing must still be preceded by counselling; a bare 'opt-out without counselling' is ethically sub-standard and may not meet the HIV Act's informed consent requirement.
CLINICAL PEARL
'Opt-out' testing is not the same as mandatory testing: Opt-out HIV testing — where patients are told testing will be performed unless they specifically decline — is permissible and widely used in PPTCT and pre-operative settings in India, but it is NOT the same as mandatory testing. An opt-out system that does not provide pre-test counselling and a genuine opportunity to decline, or that tests without telling the patient, is not legally consistent with the HIV Act 2017's informed consent requirement. The act of not actively objecting when not properly counselled is not the same as giving informed consent.
SELF-CHECK
A healthcare worker sustains a needlestick injury while treating an HIV-positive patient. The patient refuses consent for HIV testing (their status is not formally documented). Under the HIV Act 2017, what is the PRIORITY action for the healthcare worker?
A. Obtain a court order to test the patient before starting post-exposure prophylaxis (PEP)
B. Do not start PEP because the patient's HIV status has not been confirmed
C. Initiate post-exposure prophylaxis (PEP) within 72 hours without waiting for the source patient's confirmed HIV test result
D. Report the patient to the state health authority for refusing HIV testing
Reveal Answer
Answer: C. Initiate post-exposure prophylaxis (PEP) within 72 hours without waiting for the source patient's confirmed HIV test result
Post-exposure prophylaxis (PEP) must be started within 72 hours of occupational HIV exposure — the shorter the time to initiation the better (ideally within 2 hours). PEP should NOT be delayed pending the source patient's consent to test or pending HIV test results. A known HIV-positive source makes PEP mandatory; an unknown status still warrants PEP initiation if clinical suspicion is significant. The HIV Act 2017 does not permit forcing the source patient to test — their right to decline testing is protected; the healthcare worker's protection comes from PEP, not from the source patient's test.
KEY TAKEAWAYS
The HIV and AIDS (Prevention and Control) Act 2017 prohibits mandatory HIV testing and requires informed consent for all HIV tests (except court-ordered tests). Confidentiality of HIV status is strictly protected under Section 10 — disclosure to third parties requires either written consent of the PLHIV or a court order; there is no partner-notification duty. Anti-discrimination provisions prohibit denial of healthcare, employment, housing, and education on the basis of HIV status. PLHIV have the right to privacy, information, counselling, and equal access to care. Violations are prosecuted via the HIV/AIDS Ombudsman mechanism. Ethical practice requires pre- and post-test counselling, non-discriminatory care, respecting refusal of ART by competent patients, and initiating PEP without waiting for source patient test confirmation after occupational exposure.
REFLECT
You are a first-year registrar in surgery. A patient on your ward is found to be HIV-positive. You notice that a ward nurse is refusing to touch the patient without double-glowing and is visibly reluctant to enter the patient's room. Another nurse has mentioned the patient's status to a porter. Reflect on what violations of the HIV Act 2017 and general ethical principles have occurred. What are your specific obligations as the responsible clinician — to the patient, to your team, and to the hospital? How would you manage both the immediate rights violation and the underlying attitudinal issues in your clinical team?