Page 2 of 17
FM8.2,FM14.13-14 | Examination of Rape Survivor & Accused — SDL Guide
Learning Objectives
- Describe the medico-legal and clinical context governing examination of a rape survivor and accused
- Outline the step-by-step procedure for examining a rape survivor per MoHFW guidelines, including consent, history, and examination sequence
- List the trace evidence types to collect from the survivor and their methods of preservation and dispatch
- Describe the examination of the accused in cases of rape — findings, procedure, and documentation
- Prepare a standard medico-legal report for both survivor and accused with appropriate clinical objectivity and empathy
INSTRUCTIONS
The medical examination in a sexual assault case is simultaneously a clinical care encounter and a forensic investigation. Every step — from greeting the survivor to sealing a swab — has both a therapeutic and an evidentiary dimension. This module walks through the entire process, from entering the examination room through dispatching the evidence, so that your first live examination has a solid procedural foundation. The competency requires both cognitive knowledge and supervised skill (FM14.13, FM14.14): you must understand the method deeply enough to execute it under pressure.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Dr Priya, a second-year resident, is called to the emergency at 2 am. A 22-year-old woman has been brought in by a police officer following a reported sexual assault one hour ago. The police officer hands Priya a sealed envelope and says, 'Please examine her and give me the report.' Priya has read about rape examination in her textbooks, but she has never performed one. She knows she must examine the survivor, collect evidence, and write a medico-legal report. She also knows she must be empathetic and avoid re-traumatising the survivor. She does not know where to begin. This module walks her — and you — through every step, so the next time you are Priya, you are ready.
WHY THIS MATTERS
The quality of the medical examination in sexual assault cases directly influences justice outcomes. DNA evidence that is improperly collected or cross-contaminated is inadmissible; injuries not photographed or described in anatomical terms leave the court with no medical basis for inference. Equally, a poorly conducted examination that re-traumatises the survivor causes measurable psychological harm. The doctor's role is to do both — preserve evidence and preserve dignity — simultaneously. This module trains you in the MoHFW-prescribed procedure so you can meet both obligations.
RECALL
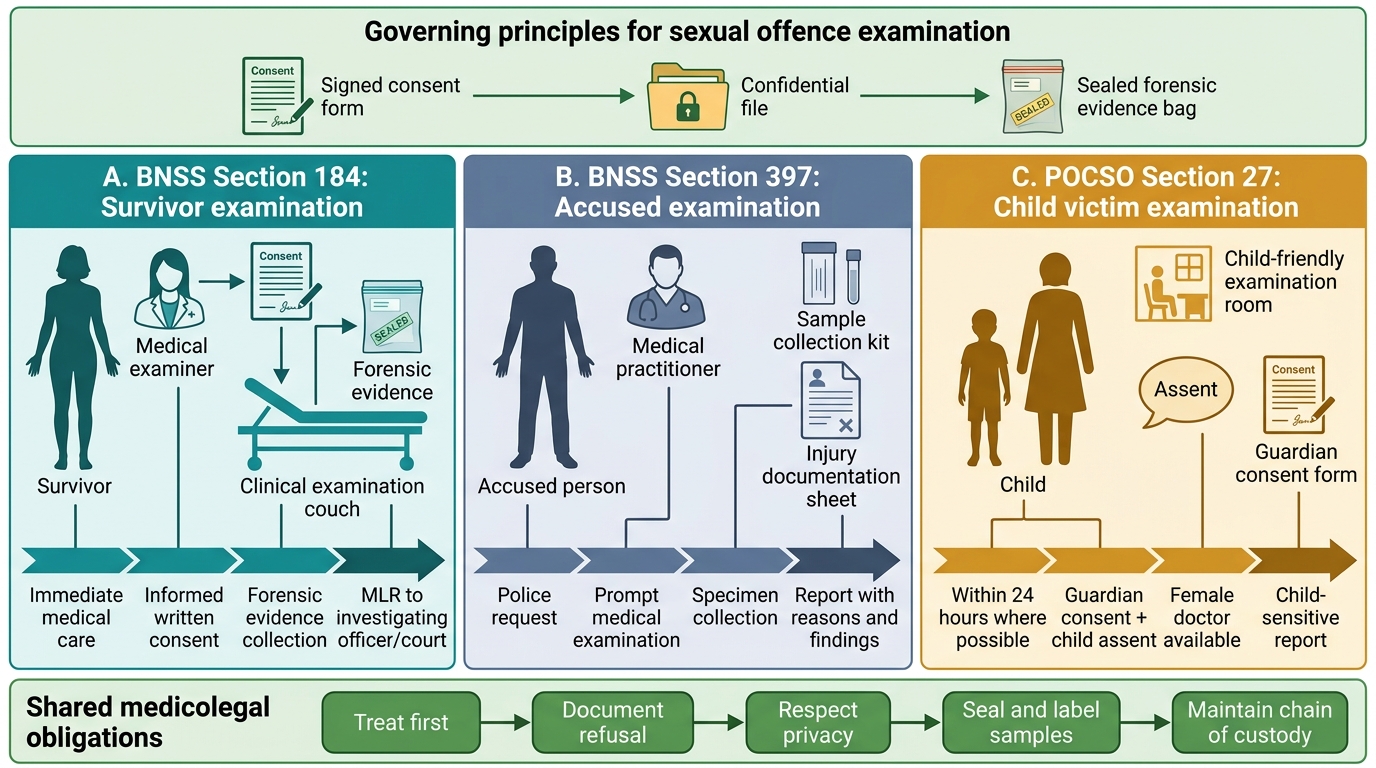
You have already learned the BNS/BNSS/POCSO framework that authorises and mandates the examination (FM8.1 SDL). Recall: BNSS Section 184 governs examination of the survivor; BNSS Section 397 governs examination of the accused; examination does not require a prior FIR; a woman doctor must be used 'as far as practicable.' Also recall from Year-1 anatomy: the anatomy of the external genitalia, hymen variants, and the ano-rectal anatomy — these are the regions you will document. From forensic medicine basics: chain of custody is the forensic principle that every piece of evidence must have an unbroken, documented path from collection to court.
Legal and Professional Context of the Examination
The medico-legal examination of a rape survivor is a clinical encounter governed by a clear statutory and ethical framework. The legal context sets the parameters: examination is authorised under BNSS Section 184 (survivor) and BNSS Section 397 (accused); for victims under 18, POCSO Section 27 adds additional requirements including the presence of a trusted adult and use of a woman doctor. The professional context defines the examiner's role: the doctor is a witness to physical findings, not a judge of guilt or innocence. The examining doctor must maintain strict clinical objectivity — the report records what is observed, not whether the account is true. This objectivity requirement is explicitly stated in FM14.13: the examination of the accused demands neutrality and scientific rigour regardless of personal reaction to the alleged offence.
Crucially, the examination is a therapeutic-forensic encounter, not a purely forensic one. MoHFW guidelines (2014, reaffirmed 2022) require that the doctor explain each step to the survivor, obtain consent before each component of the examination, and pause or modify the approach if the survivor shows signs of acute distress. For child survivors (POCSO cases), the examination must not feel like an interrogation — use age-appropriate language, maintain a calm and reassuring tone, and ensure the trusted adult is within sight of the child throughout. These are not optional courtesies; they are standard-of-care requirements.
Legal Framework for Sexual Offence Examination
Governing Principles: Consent, Confidentiality, and Chain of Custody
Three governing principles underpin the entire examination process, and each has both a clinical and a medicolegal dimension.
Consent is the starting point. The survivor must provide informed, written consent before examination. For minors under 18 (POCSO), the guardian's consent is required alongside the child's assent where possible. If the survivor is unconscious or incapacitated, consent may be presumed for life-saving medical treatment, but the forensic examination components should be deferred until she can consent. The consent form must document what the survivor was told, that she understood, and that she agreed. Consent can be withdrawn at any time — if the survivor refuses to allow any component of the examination (e.g., vaginal swab), this must be documented and respected, and the rest of the examination must proceed.
Confidentiality is both an ethical and legal duty. The medico-legal report is a confidential document; copies go only to the investigating officer and the court. Sharing findings with family members, the media, or unauthorised persons is a professional misconduct offence. The survivor's identity is protected under Section 228A of the IPC (now continued under BNS provisions); disclosing it publicly is a criminal offence.
Chain of custody is the forensic cornerstone. Every specimen — vaginal swab, blood sample, clothing item, hair sample — must be collected, labelled, sealed, and dispatched with a documented, unbroken chain of possession. The label on each item must record: case number, date and time of collection, description of the specimen, the collector's name and signature, and the seal applied. The sealed packet must be handed personally to the investigating officer with a forwarding letter, and the doctor must retain a copy of the forwarding letter. Any break in the chain of custody may render the specimen inadmissible in court.
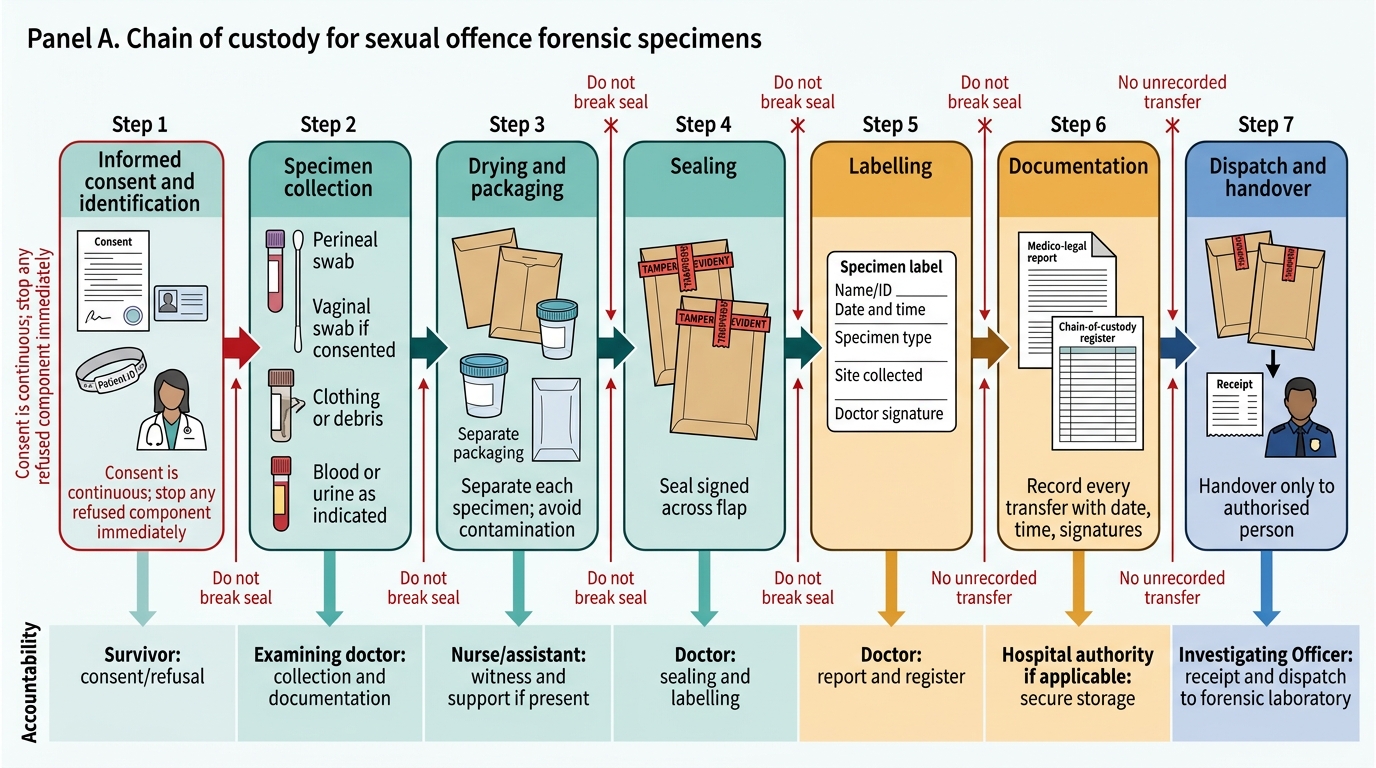
Chain of Custody for Sexual Offence Forensic Specimens
SELF-CHECK
A rape survivor undergoing examination suddenly asks the doctor to stop the vaginal swab collection. The doctor has already collected the perineal swab. What is the correct action?
A. Explain the importance of the swab and proceed after reassurance
B. Stop immediately, document the refusal, and respect her decision; proceed with remaining non-refused examination components
C. Ask the police officer to authorise continuation of examination
D. Defer the entire examination to a later time when the survivor may be calmer
Reveal Answer
Answer: B. Stop immediately, document the refusal, and respect her decision; proceed with remaining non-refused examination components
Consent is continuous and can be withdrawn at any time. The doctor must immediately stop the refused component, document the refusal in the report, and continue with the parts of the examination the survivor permits. Proceeding against explicit refusal constitutes assault.
Examination of the Rape Survivor: Method and Documentation
The examination follows a prescribed sequence to maximise evidence yield while minimising trauma. The MoHFW guidelines divide the process into six phases, which must be followed in order.
Phase 1 — Documentation of general findings: Record the time and date of examination, time elapsed since alleged assault, general mental and physical state (conscious, oriented, anxious, tearful — use descriptive, not interpretive language), vital signs, and height/weight. Photograph any visible injuries on exposed skin areas with consent.
Phase 2 — History: Take a structured history covering: the account of the assault (time, place, nature of acts described), whether the survivor bathed or changed clothes since the assault, last consensual intercourse (if applicable — relevant to DNA interpretation), gynaecological history (menstrual status, prior deliveries, surgical history), and medical/medication history. The history is taken in private, in a supportive manner, and must not read like an interrogation transcript in the report.
Phase 3 — Clothing examination: Note the condition of clothing (intact, torn, stained), photograph it, and collect items for trace evidence analysis (semen stains, foreign fibres, hair). Each garment is placed in a separate paper bag (not plastic — plastic promotes microbial growth that degrades DNA), sealed, labelled, and entered into the evidence register.
Phase 4 — General body examination: Systematic top-to-bottom examination for injuries — document every finding using the standard injury description format: site, size, shape, colour, character, and age estimation. Pay particular attention to: neck (strangulation marks, petechiae), wrists and ankles (restraint marks), inner thighs, breasts, and any bite marks. Use a body diagram.
Phase 5 — Ano-genital examination: This is the most technically demanding and most legally scrutinised component. The examination must be performed with the survivor in the lithotomy position (for women) or knee-chest position for anal examination. Steps include:
- External genitalia: labial inspection, examination for lacerations, bruising, erythema
- Hymen: describe its form (annular, fimbriated, imperforate, etc.), any fresh tears (note location using clock face), old healed tears, or absence
- Vaginal examination: speculum examination if consented to; swabs from posterior fornix, lateral walls
- Anal examination: inspect for lacerations, bruising, fissures, spasm
- Urethra: examine for meatal injury
Critical documentation principle: describe findings precisely — 'fresh hymenal tear at 6 o'clock position, measuring approximately 0.5 cm, with erythematous margins and active bleeding' — and avoid conclusory statements such as 'findings consistent with penetrative intercourse.'
Phase 6 — Specimen collection and labelling: Collect vaginal swabs (at least two — one for DNA, one for microscopy), endocervical swab, anal swab if anal assault reported, oral swab if oral assault reported, blood sample (for DNA reference, toxicology if intoxication suspected), urine sample (for toxicology), fingernail scrapings (for DNA from contact), and pubic hair combings. Each sample: label, seal, evidence register entry.
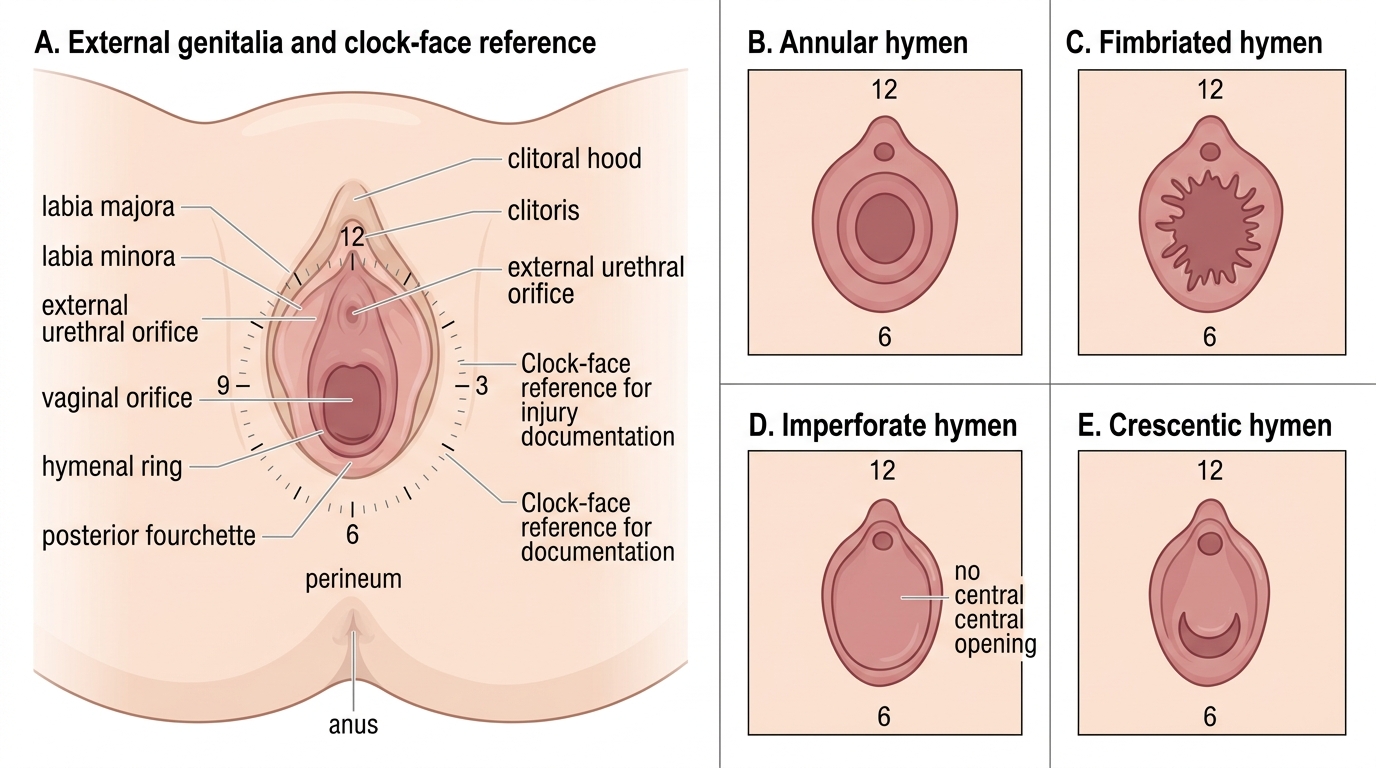
Female External Genitalia, Hymen Variants, and Clock-Face Documentation
SELF-CHECK
Clothing collected from a rape survivor as evidence should be stored in which type of container to preserve DNA integrity?
A. Sealed plastic zip-lock bags to prevent contamination
B. Separate paper bags — one per garment
C. A single sealed plastic container with desiccant
D. Refrigerated glass jars with preservative
Reveal Answer
Answer: B. Separate paper bags — one per garment
Clothing evidence must be placed in separate paper bags. Plastic bags trap moisture, which promotes microbial growth and degrades biological material including DNA. One garment per bag prevents cross-contamination between items.
Examination of the Accused: Procedure and Objectivity
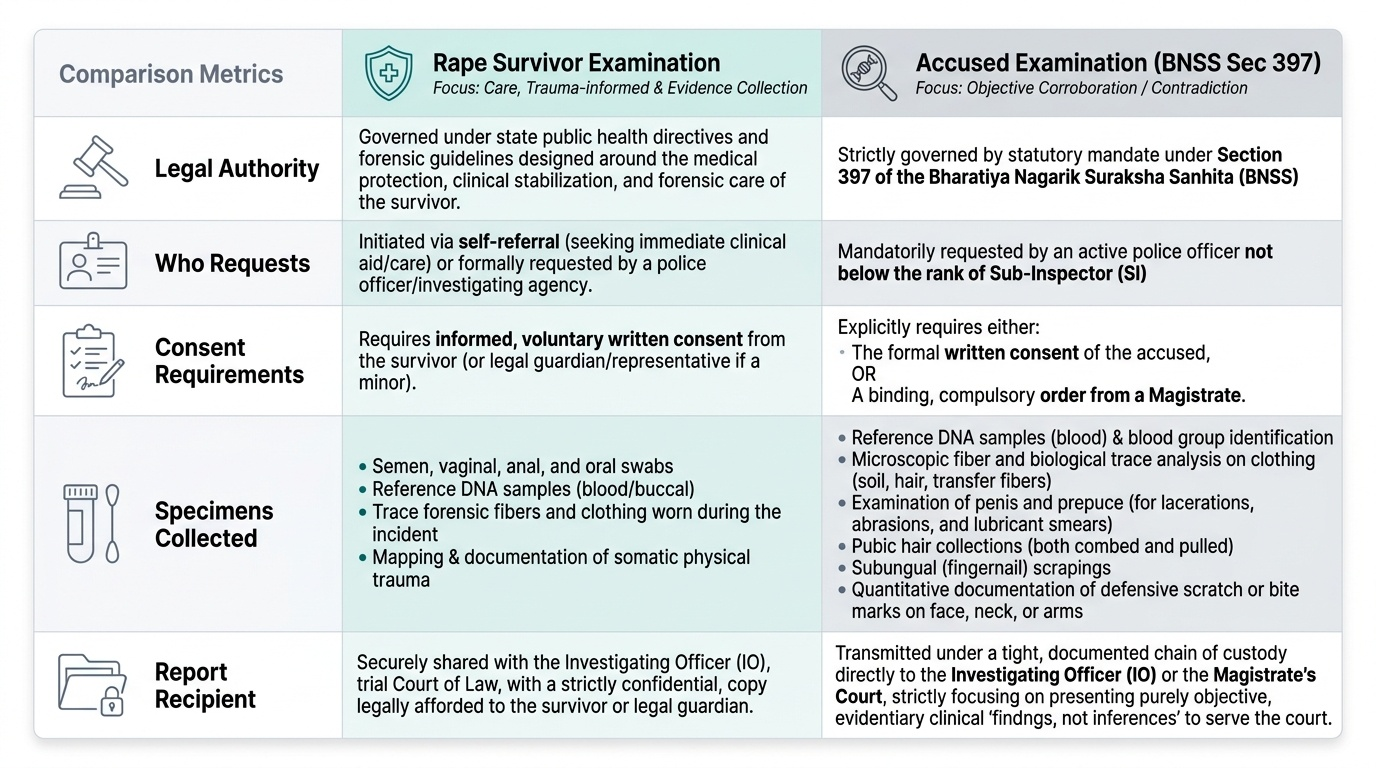
The examination of the accused is governed by BNSS Section 397. It is conducted by a registered medical practitioner at the request of a police officer not below the rank of Sub-Inspector (SI), and requires either the written consent of the accused or an order from a magistrate. The examination is conducted with the same forensic rigour as the survivor examination, but the clinical orientation is fundamentally different: the doctor is looking for corroborative or contradictory physical evidence, not providing care.
The standard elements of the accused examination include: general physical condition, blood group, DNA reference sample (blood), clothing examination for biological trace evidence, examination of the penis and prepuce for lacerations, abrasions, or lubricant smears, pubic hair samples (combed and pulled), fingernail scrapings, and any injuries that may have been caused by the survivor in self-defence (scratches, bite marks, finger-nail injuries on the face, neck, or arms). Foreign fibres, hair, and soil from the accused's clothing may corroborate the alleged location of the assault.
The objectivity requirement (FM14.13) is paramount. The accused may present with apparent social status, may deny involvement, or may display distress. None of these affect the examination process. The doctor's report must be identical in structure and clinical tone to the survivor's report — findings, not inferences. If the penis shows no injury and there is no semen in the clothing, this is recorded as such; it does not mean rape did not occur, and the report must not state that it does. The doctor is a fact-finder, not an adjudicator.
The medicolegal report for the accused includes: time and date of examination, general physical findings, detailed ano-genital findings, list and description of specimens collected, chain-of-custody documentation, and the doctor's signature and registration number. The report is addressed to and dispatched to the investigating officer who requested the examination.
Provided image
CLINICAL PEARL
The absence of injuries does not mean sexual assault did not occur. Studies show that the majority of rape survivors have no genital injury detectable on examination — particularly in adults, in cases involving prior sexual activity, or when examination is delayed beyond 72 hours. Do not write 'no evidence of sexual assault' in a report. Write 'no injury detected on examination on [date/time].' The legal and factual significance of that finding is for the court to weigh.
SELF-CHECK
After completing the examination of a rape survivor, the examining doctor has no genital injuries to document. Which statement is most appropriate to include in the medico-legal report?
A. No evidence of sexual assault
B. Findings are inconsistent with the alleged history
C. No injuries detected on examination of the external genitalia and hymen; findings neither confirm nor exclude the alleged history
D. The alleged assault appears to have not occurred based on clinical findings
Reveal Answer
Answer: C. No injuries detected on examination of the external genitalia and hymen; findings neither confirm nor exclude the alleged history
The doctor records findings only. Absence of injury does not exclude sexual assault; this must be stated explicitly. Conclusory statements such as 'no evidence of sexual assault' exceed the doctor's role and may prejudice the survivor's case unjustly.
KEY TAKEAWAYS
The examination of rape survivor and accused involves a systematic, consent-based, empathy-guided procedure governed by BNSS Sections 184 and 397. For the survivor: consent documentation → history → clothing → general body examination → ano-genital examination (hymen, vaginal, anal, oral as indicated) → specimen collection (vaginal swabs, blood, urine, hair, fingernail scrapings, clothing) → chain-of-custody documentation → report dispatch within 24 hours. For the accused: police request (SI or above) → consent or magistrate order → reference blood, clothing, penile examination, pubic hair, fingernail scrapings → chain-of-custody → report dispatch. Governing principles: consent is continuous and can be withdrawn; chain of custody is unbroken; report records findings not conclusions; absence of injury does not exclude assault. The doctor's role is therapeutic-forensic — not adjudicatory.
REFLECT
A 19-year-old man is brought for examination as the accused in a rape case. He is visibly distressed and says he is innocent. The police officer who brought him is in the room throughout and appears hostile. How would you conduct this examination to meet your forensic obligations under BNSS Section 397 while preserving the required objectivity? What specific findings would you look for? How would you manage the presence of the police officer in the examination room?