Page 3 of 17
FM8.3 | Sexual Offences: Consent, Orientation & Unnatural Offences — SDL Guide
Learning Objectives
- Define informed consent in the context of intercourse and identify circumstances where consent is vitiated
- Describe the history of gender and sexuality-based identities and rights in India, including the decriminalisation of consensual adult homosexual behaviour
- Explain the decriminalisation of adultery under Indian law
- Define and describe the medico-legal significance of forced anal sex, forced oral sex, bestiality, finger/object insertion, and indecent assault
- Apply these concepts to clinical documentation and medicolegal reporting
INSTRUCTIONS
The concept of consent is the cornerstone of the entire law of sexual offences. When consent is present, freely given, and fully informed, sexual conduct between adults is neither criminal nor medico-legally significant. When consent is absent or vitiated, the law intervenes — and the examining doctor's role begins. This module examines consent as a legal and clinical concept, traces the evolution of Indian law on sexuality and gender identity, and defines the specific sexual offences with medicolegal significance that extend beyond vaginal rape.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old man presents to the emergency department with ano-rectal injuries. He reports that he was sexually assaulted by a male acquaintance. During triage, a nurse says, 'But two men — can that even be reported?' The registrar is unsure how to document the complaint. Across the corridor, a 30-year-old woman has been brought by police claiming her husband subjected her to forced oral sex and she wishes to file a complaint. The registrar has never seen a case documented as 'unnatural offence.' This module gives you the legal and clinical framework to handle both cases correctly — and understand why the nurse's question is factually and legally wrong.
WHY THIS MATTERS
Consent doctrine separates criminal from non-criminal sexual acts; without understanding it, the doctor cannot frame findings in legally meaningful terms. The 2018 Supreme Court judgment decriminalising consensual adult homosexual conduct (Navtej Singh Johar v. Union of India) fundamentally altered the medico-legal landscape — conduct that was formerly prosecutable is now lawful. The 2018 judgment decriminalising adultery (Joseph Shine v. Union of India) similarly removed a class of 'offence' from the statute book. Simultaneously, BNS has expanded the definition of sexual offences beyond vaginal penetration. The doctor who does not know this legal evolution risks improper documentation, improper advice to patients, and potentially contributing to discrimination.
RECALL
From your FM8.1 SDL: BNS Section 63 defines rape across seven circumstances, including consent given when the person is under 18, intoxicated, or threatened. From Year-1 sociology/ethics: consent requires capacity (age and mental state), voluntariness (absence of coercion), and information (understanding what is being consented to). From general legal principles: a person cannot consent to their own harm in most circumstances, and the law sets minimum age thresholds for consent. Recall that the IPC (replaced by BNS) included Section 377, which criminalised 'unnatural offences' — the fate of this section is central to this module.
Informed Consent in Intercourse: Definition and Vitiating Circumstances
Consent in the context of sexual intercourse is a voluntary, freely given, and informed agreement to participate in a specific sexual act, at a specific time, with a specific person. The law does not treat consent as a single, perpetual permission — consent to one act does not imply consent to another, and consent may be withdrawn at any time. The BNS Section 63 elaborates on this implicitly through its list of circumstances that vitiate consent, which are now understood as circumstances where the law treats the apparent agreement as legally invalid.
The circumstances that vitiate consent under BNS Section 63 are: (1) against will — the person actively objects at the time; (2) without consent — passive absence of agreement, even if there is no active resistance (the law in India has moved away from requiring active struggle as evidence of non-consent); (3) consent under fear of death or hurt — threats to the person or anyone close to her; (4) consent by impersonation of husband — the person consents believing the other to be her husband; (5) consent under unsoundness of mind, intoxication, or administered stupefying substance — the person cannot understand the nature of the act; (6) age under 18 years — consent is a legal nullity regardless of apparent willingness; (7) inability to communicate consent — physical or cognitive inability.
The medicolegal significance of these circumstances is direct: the doctor examining a survivor must identify which circumstance is alleged, because the examination protocol, the specimens collected, and the documentation emphasis will differ. If intoxication is alleged (circumstance 5), blood and urine toxicology is essential. If the survivor is under 18 (circumstance 6), POCSO triggers. If communication disability is relevant (circumstance 7), an assessment of the survivor's cognitive and communicative capacity becomes part of the report.
Age of consent: The age of consent in India for the purposes of sexual intercourse is 18 years — there are no exceptions based on marriage, religion, or cultural context. A person under 18 cannot legally consent to sexual intercourse, and sexual activity with a person under 18 is rape under BNS and sexual assault under POCSO regardless of the minor's apparent agreement.
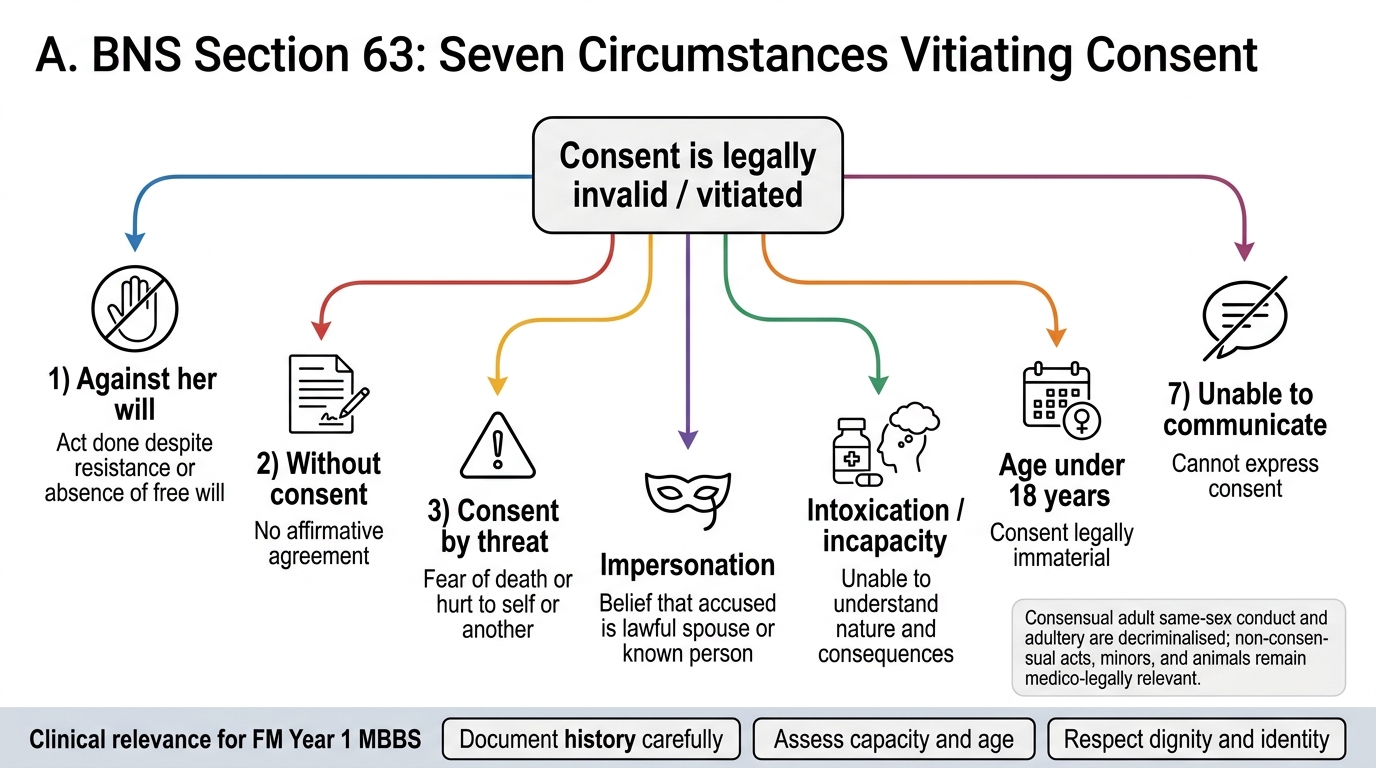
Seven Circumstances Vitiating Consent Under BNS Section 63
Decriminalisation of Consensual Adult Homosexual Conduct and Adultery
The history of gender and sexuality-based rights in India underwent a seismic shift with two landmark Supreme Court judgments that every medical professional must understand, because they directly affect how patients present and how the doctor must respond.
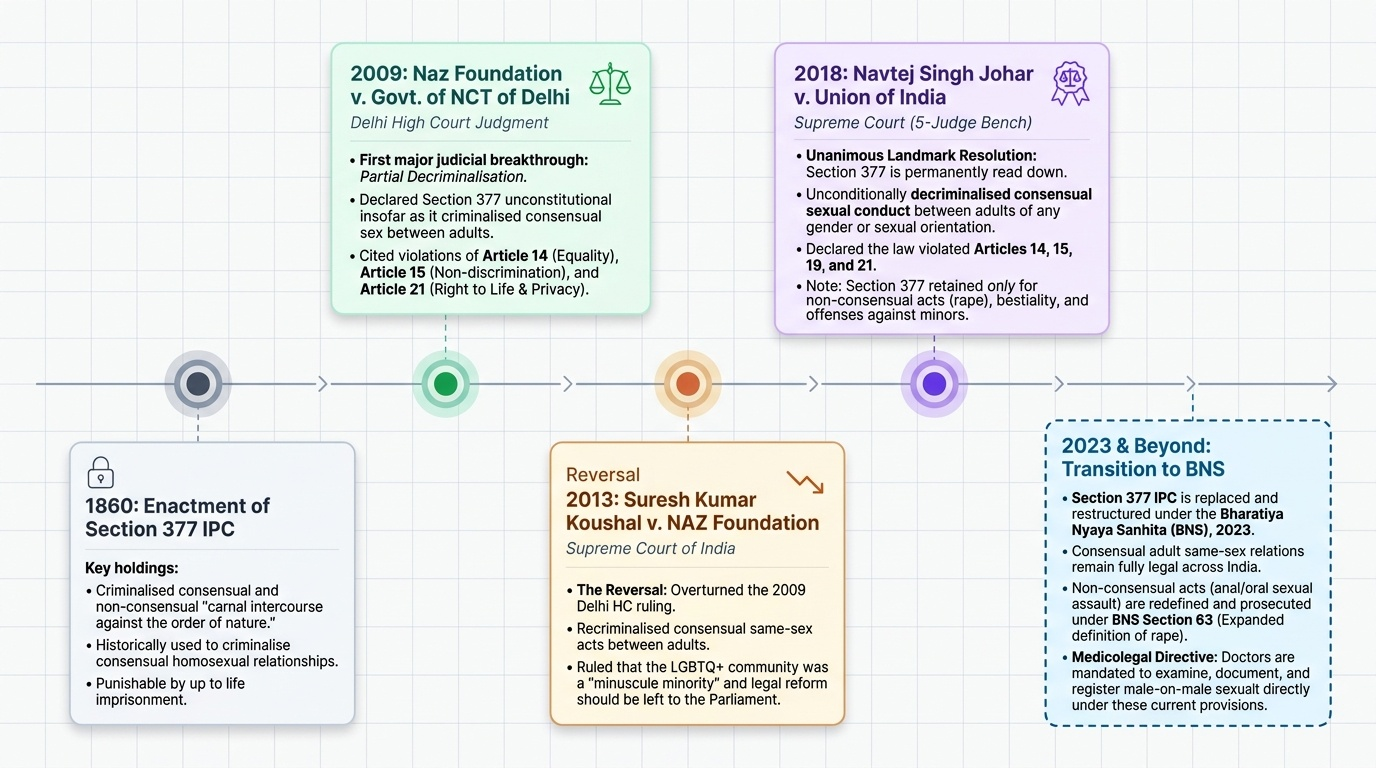
Section 377 IPC (Unnatural Offences) — partial decriminalisation: IPC Section 377 criminalised 'carnal intercourse against the order of nature' — historically interpreted to include homosexual intercourse, bestiality, and other acts. In Navtej Singh Johar v. Union of India (2018), a five-judge Constitution Bench unanimously held that insofar as Section 377 criminalised consensual sexual conduct between adults, it violated Articles 14 (equality), 15 (non-discrimination on grounds including sex), 19 (freedom of expression/identity), and 21 (personal liberty and dignity). The court partially read down Section 377: consensual sexual conduct between competent adults — regardless of gender or sexual orientation — is decriminalised. Section 377 continues to apply to non-consensual acts (anal rape, forced oral sex) and to sexual acts with minors and animals.
In the BNS 2023, Section 377 equivalent provisions were restructured: non-consensual penetration (anal, oral) is now prosecuted under BNS Section 63's expanded act definition, which explicitly includes penile penetration of the anus or mouth and oral-genital contact. The key medicolegal implication: a man reporting non-consensual anal or oral sexual assault by another man has a valid complaint under BNS Section 63 and the doctor must examine and document it as such.
Gender and sexuality-based identities: India legally recognises transgender persons as a 'third gender' following the NALSA judgment (2014) and the Transgender Persons (Protection of Rights) Act 2019. The doctor's examination and documentation must use the person's self-identified gender. Medical records must respect preferred pronouns and identity. This is a professional and legal obligation, not merely a courtesy.
Adultery — Section 497 IPC (repealed): In Joseph Shine v. Union of India (2018), the Supreme Court struck down IPC Section 497 (adultery) as unconstitutional, holding that it treated women as property of their husbands and violated Articles 14, 15, and 21. Adultery is no longer a criminal offence in India. It may still be a ground for divorce in civil matrimonial law, but it cannot be the subject of a criminal complaint. The medicolegal consequence: a doctor approached to examine a spouse for 'proof of adultery' for purposes of criminal prosecution must be aware that no such prosecution is possible.
Provided image
SELF-CHECK
Following the Navtej Singh Johar judgment (2018), which of the following remains criminalised under Section 377 IPC / equivalent BNS provisions?
A. Consensual anal sex between two consenting adult men
B. Consensual sexual conduct between any two consenting adults regardless of gender
C. Non-consensual anal penetration and sexual acts with minors or animals
D. Homosexual conduct between adults in private
Reveal Answer
Answer: C. Non-consensual anal penetration and sexual acts with minors or animals
The Navtej Johar judgment decriminalised consensual sexual conduct between competent adults. Section 377 / equivalent BNS provisions continue to apply to non-consensual acts, acts with minors (POCSO), and acts with animals (bestiality). Consensual adult homosexual conduct is fully decriminalised.
Sexual Offences with Medicolegal Significance: Unnatural Offences and Indecent Assault
Beyond vaginal rape, several categories of sexual offences require specific clinical examination protocols and medico-legal documentation. These are now primarily defined under BNS Section 63's expanded act definition, with some conduct under separate BNS provisions.
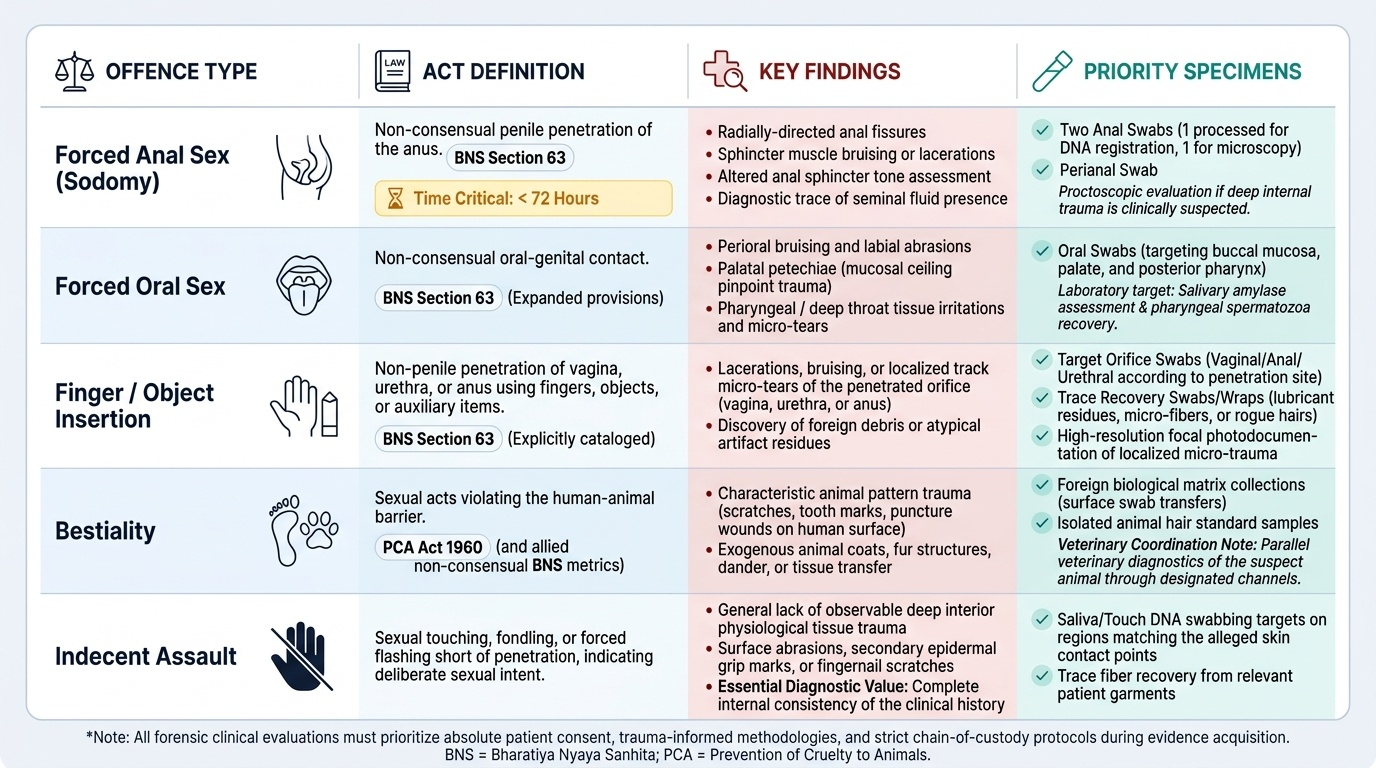
Forced anal sex (sodomy): Non-consensual penile penetration of the anus. In forensic examination, anal assault leaves characteristic findings: anal fissures (radially directed from the anus), bruising or lacerations of the anal sphincter, sphincter tone assessment, and occasionally seminal material in the anal canal. Specimens: anal swab (two — for DNA and microscopy), perianal swab. A proctoscopic examination may be indicated if internal injury is suspected. Key point: acute anal injuries heal rapidly — examination within 72 hours maximises evidence yield.
Forced oral sex: Non-consensual oral-genital contact. This requires an oral swab from the buccal mucosa, palate, and posterior pharynx. Injuries may include perioral bruising, abrasions of the lips, palatal petechiae (from forced fellatio), and rarely throat injuries. Oral swabs are the primary evidence — salivary amylase and spermatozoa on a pharyngeal swab can be valuable.
Bestiality: Sexual acts with animals. This constitutes an offence under the Prevention of Cruelty to Animals Act 1960 and, where non-consensual towards any human or animal, under BNS. In the human examination, the doctor looks for animal hair, foreign biological material, and pattern injuries consistent with animal claws or teeth. Veterinary examination of the animal may also be required by police.
Finger or object insertion: Non-penile penetration using fingers, objects, or other body parts. BNS Section 63 explicitly includes these acts. Clinical examination follows the same protocol as vaginal/anal assault examination: documentation of injuries, specimen collection from the penetrated orifice, and photography. Foreign body material (lubricant, fabric fibre) may be present and should be collected.
Indecent assault: Sexual touching short of penetration, done with sexual intent, without consent. This includes fondling, inappropriate touching over clothing, and exposure. Physical findings may be absent. Documentation relies on history, consistency of account, and any incidental findings (bruising from grip, etc.).
For all these offences, the examination protocol mirrors the rape examination in its systematic approach, chain-of-custody requirements, and report format. The competency (FM14.13, FM14.14) applies equally — objectivity, empathy for survivors, and strict clinical documentation are required in every case.
Provided image
SELF-CHECK
In a case of alleged forced oral sex, which specimen should be prioritised for forensic evidence?
A. Vaginal swab from the posterior fornix
B. Oral swab from buccal mucosa, palate, and posterior pharynx
C. Blood sample for DNA profiling of the survivor
D. Anal swab
Reveal Answer
Answer: B. Oral swab from buccal mucosa, palate, and posterior pharynx
In forced oral sex (fellatio or cunnilingus forced on the survivor), the oral cavity is the primary site of potential spermatozoa and DNA transfer. Oral swabs from the buccal mucosa, palate, and particularly the posterior pharynx should be collected promptly, as spermatozoa are cleared from the oral cavity within a few hours.
Medicolegal Inference and Documentation Framework
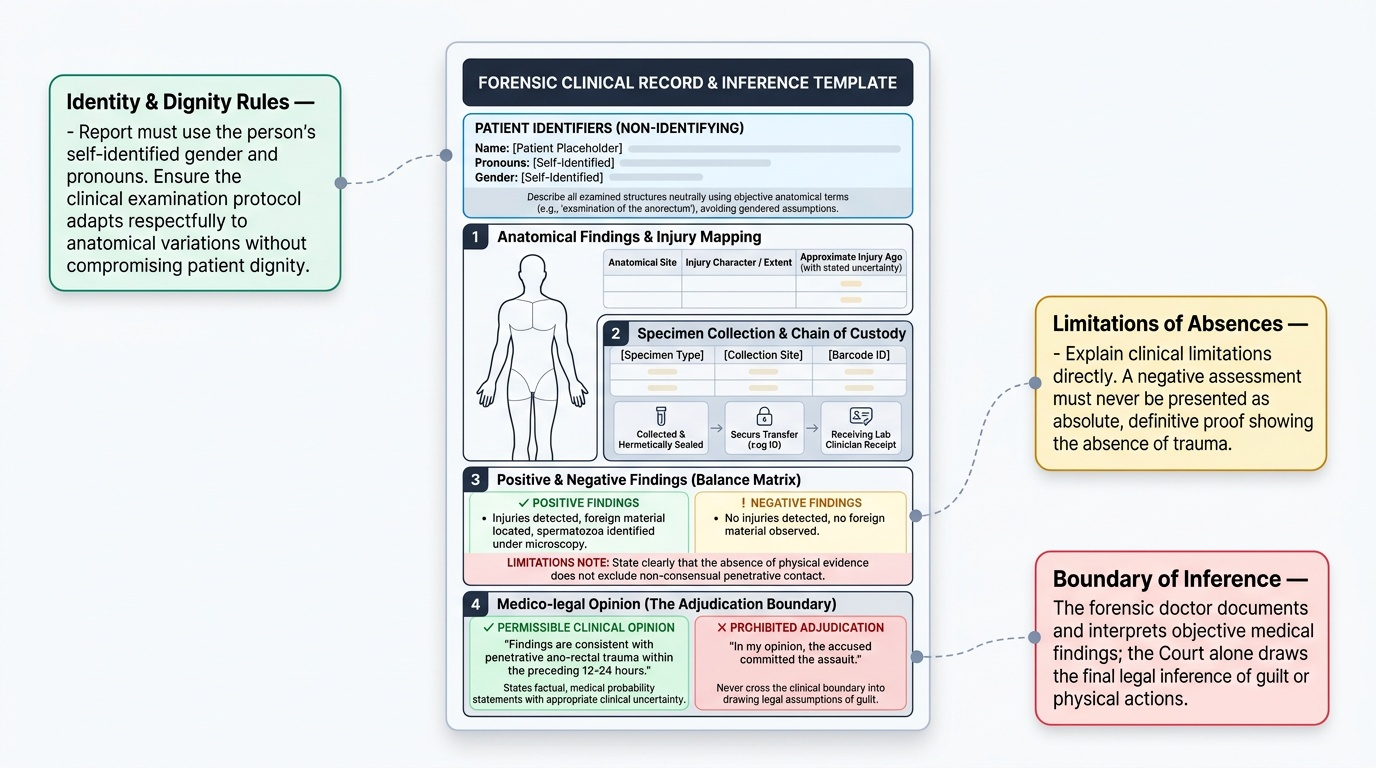
The forensic clinician's documentation must map clinical findings onto the legal framework, without crossing the boundary into legal adjudication. The medicolegal report for cases of unnatural or unusual sexual offences should address: (1) which anatomical sites show injuries consistent with trauma, and what the character, extent, and approximate age of those injuries are; (2) which specimens were collected, from which sites, under what chain-of-custody conditions; (3) which findings are positive (injuries present, spermatozoa identified, foreign material found) and which are negative (no injury detected, no spermatozoa on immediate microscopy) — always noting the limitations of negative findings; (4) an opinion on the approximate time of any injuries, stated with appropriate uncertainty.
The report must never state: 'In my opinion, the accused committed the act.' The report may state: 'Findings are consistent with penetrative ano-rectal trauma within the preceding 12-24 hours.' The court draws the inference; the doctor states the facts.
Special documentation issues arise with cases involving gender-diverse persons. The report must use the person's self-identified gender and pronouns; the anatomy examined should be described neutrally using anatomical terms (e.g., 'examination of the anorectum' rather than gendered assumptions about the patient's body). Trans persons may have anatomy that does not match their self-identified gender, and the examination protocol must be adjusted accordingly while respecting the person's dignity and identity.
Provided image
CLINICAL PEARL
The Supreme Court in Navtej Singh Johar specifically directed that the LGBTQ+ community be accorded equal rights and treatment by state institutions, including medical facilities. A doctor who refuses to examine a same-sex assault survivor, documents their orientation in a discriminatory manner, or treats their complaint with less seriousness is violating a constitutionally recognised right. Clinical objectivity and equal treatment are mandatory, not optional.
SELF-CHECK
A 28-year-old transgender woman (male-to-female) reports non-consensual anal assault. Which of the following is the most appropriate approach to documentation?
A. Document as 'male patient with anal assault' based on biological sex
B. Refuse examination pending legal clarification of gender status
C. Conduct examination using anatomical terms, respect self-identified gender in the report, and follow the standard protocol for ano-rectal assault
D. Defer to psychiatry to assess gender dysphoria before proceeding
Reveal Answer
Answer: C. Conduct examination using anatomical terms, respect self-identified gender in the report, and follow the standard protocol for ano-rectal assault
The Transgender Persons (Protection of Rights) Act 2019 and the NALSA judgment mandate equal treatment and respect for self-identified gender. Documentation uses anatomical terms for findings, uses the person's self-identified gender and preferred pronouns in the report, and follows standard examination and evidence collection protocol. There is no basis to defer or refuse.
KEY TAKEAWAYS
Consent in intercourse requires voluntary, informed agreement with capacity; it may be vitiated by threat, deception, incapacity, intoxication, age under 18, or inability to communicate. BNS Section 63's expanded act definition covers penile/object/body-part penetration of any orifice and oral-genital contact. The Navtej Singh Johar judgment (2018) decriminalised consensual adult homosexual conduct; non-consensual acts remain criminal under BNS. Joseph Shine (2018) removed adultery from criminal law. India legally recognises transgender identity; equal clinical treatment is mandatory. Sexual offences beyond vaginal rape — forced anal sex, forced oral sex, bestiality, finger/object insertion, indecent assault — each require site-specific examination protocols and evidence collection. The medicolegal report records findings, not adjudication.
REFLECT
A 35-year-old man presents claiming his male partner subjected him to non-consensual anal assault. He is anxious and says he was told at another hospital that the police won't take his complaint seriously. How would you conduct this examination? What is the legal basis for treating this as a valid complaint? What documentation would you prepare, and which evidence would you prioritise?