Page 4 of 17
FM8.6 | Paraphilias & Paraphilic Disorders — SDL Guide
Learning Objectives
- Distinguish between a paraphilia (atypical sexual interest) and a paraphilic disorder (causing distress or involving harm to others)
- Classify the major paraphilic disorders as listed in DSM-5 and ICD-11
- State the medicolegal implications of each major paraphilic disorder
- Explain how the concept of informed consent interacts with paraphilic practices
INSTRUCTIONS
Human sexuality includes a spectrum of attractions and interests beyond conventional heterosexual intercourse. The law, psychiatry, and forensic medicine have all had to grapple with how to categorise, treat, and regulate these variations. This module focuses on the critical distinction — clinically and legally — between variant sexual interests that cause no harm and those that constitute disorder or crime.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old man is referred to the forensic medicine department by court order, following his arrest for publicly exposing his genitals to women at a bus stop — this being the third such incident in six months. His lawyer argues that he has a psychiatric condition and the acts were involuntary. The court wants a medico-legal opinion: does he have a 'paraphilic disorder' as defined by psychiatric classification? Is the behaviour a matter of mental illness, moral failing, or criminal conduct? The forensic clinician must navigate DSM-5 and ICD-11 alongside the criminal law to produce a nuanced, defensible opinion.
WHY THIS MATTERS
Paraphilic presentations arrive in forensic medicine through the criminal courts (offenders seeking psychiatric defence), through psychiatric referrals (patients in distress about atypical attractions), and through clinical encounters where a patient discloses non-mainstream sexual behaviour. The forensic clinician's value lies in being able to apply the DSM-5/ICD-11 distinction between paraphilia and paraphilic disorder precisely — because this distinction directly affects criminal responsibility assessments, sentencing submissions, and treatment decisions.
RECALL
From your Year-1 psychiatry and behavioural sciences: recall the DSM-5 diagnostic framework — a psychiatric diagnosis requires clinically significant distress or functional impairment. Recall from FM8.3: consent between competent adults is the legal gateway to lawful sexual conduct. Recall the criminal defence of insanity under the McNaughten rules (carried into Indian law under Section 84 IPC, now BNS equivalent): not guilty by reason of unsoundness of mind requires that the person did not know the nature or quality of the act, or did not know it was wrong. Most paraphilic disorders do not meet this threshold — the person usually knows what they are doing and knows it is legally prohibited.
Paraphilia vs Paraphilic Disorder: The Critical DSM-5/ICD-11 Distinction
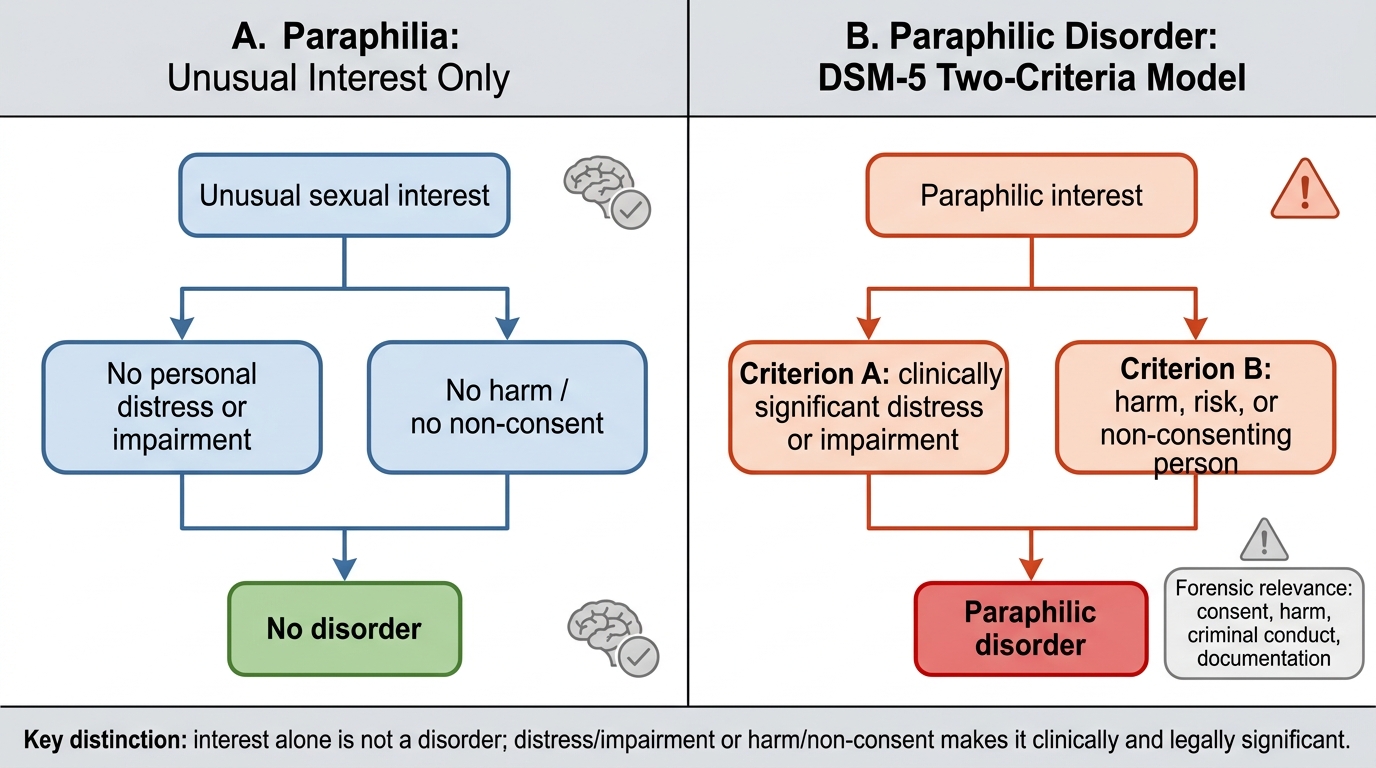
The most important conceptual distinction in this entire domain — one that has direct medicolegal consequences — is between a paraphilia and a paraphilic disorder.
A paraphilia (from Greek: para = beside, philia = attraction) refers to any intense, persistent sexual interest in objects, situations, or individuals other than physically mature, consenting adults. The interest itself is a variant of sexual behaviour. DSM-5 makes explicit: 'A paraphilia by itself does not necessarily justify or require clinical intervention.' If the atypical interest causes no distress to the individual and does not involve harm to others (including non-consenting persons, minors, or animals), it is a paraphilia — a variation, not a disorder.
A paraphilic disorder requires two criteria: (1) the paraphilic interest causes clinically significant distress or functional impairment to the individual, OR (2) the paraphilia involves acting on urges with a non-consenting person, a minor, or an animal — thereby incorporating harm to others as the second route to disorder classification. This distinction is crucial for the forensic clinician: the man who is sexually aroused by women's shoes but causes no harm and is not distressed has a paraphilia (shoe fetishism), not a disorder. The man who exposes his genitals non-consensually to strangers meets criterion 2 for exhibitionistic disorder, regardless of whether he is personally distressed.
ICD-11 (World Health Organisation, 2019) follows the same dichotomy under the category 'Paraphilic disorders' (6D30-6D3Z): it specifies that diagnosis requires 'marked distress to the individual' or 'a significant risk of harm to self or others.'
Paraphilia vs Paraphilic Disorder
Classification of Major Paraphilic Disorders (DSM-5 / ICD-11)
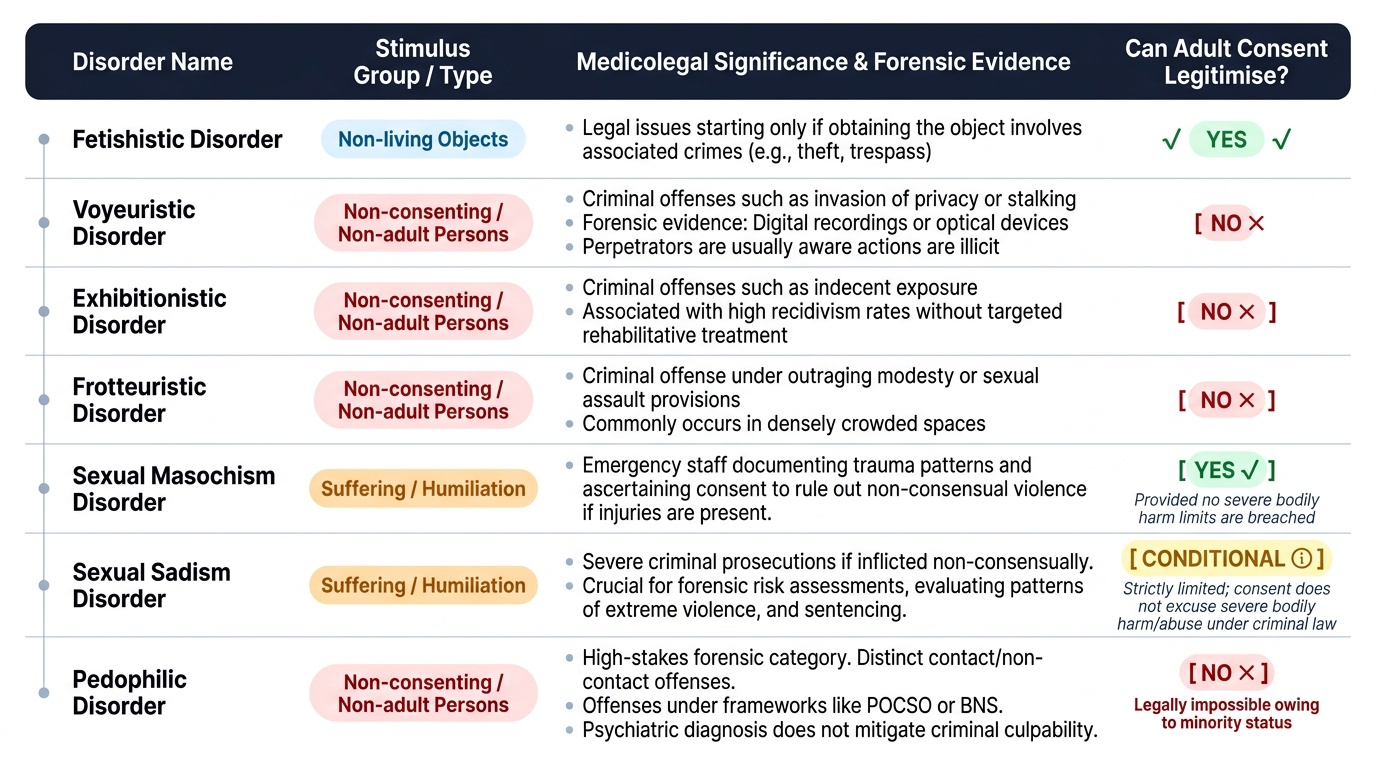
DSM-5 lists eight specific paraphilic disorders and one residual category. ICD-11 maps closely to this structure. Each has specific medicolegal implications. The classification is organised by the nature of the stimulus (non-human objects, suffering/humiliation, non-consenting/non-adult persons).
1. Voyeuristic disorder: Sexual arousal from observing non-consenting persons undressing or engaged in sexual activity. Medicolegal implication: criminal offence (invasion of privacy, stalking); evidence may include recording devices, digital material. Individuals are typically aware their conduct is wrong.
2. Exhibitionistic disorder: Sexual arousal from exposing genitals to unsuspecting strangers without their consent. Medicolegal: criminal offence; recidivism rate is high without treatment; the hook scenario above illustrates this presentation.
3. Frotteuristic disorder: Sexual arousal from touching or rubbing against a non-consenting person (typically in crowded spaces — the 'groping' offence). Medicolegal: criminal offence under outraging modesty provisions.
4. Sexual masochism disorder: Sexual arousal from being humiliated, beaten, bound, or made to suffer. Where conducted with a consenting adult, it is not criminal; if the individual's own distress triggers the disorder diagnosis, treatment is indicated. Medicolegal: injury pattern may present to emergency — document injuries carefully; ascertain consent.
5. Sexual sadism disorder: Sexual arousal from inflicting pain, humiliation, or suffering on another. Where the other party is non-consenting or a minor, this is a serious criminal offence associated with the worst categories of sexual violence. Medicolegal: may explain pattern injuries or extreme violence in sexual assault cases; relevant to risk assessment and sentencing.
6. Pedophilic disorder: Sexual arousal directed primarily to prepubescent children (generally ≤13 years). Note: the diagnosis requires the individual be ≥16 years and ≥5 years older than the victim. This is perhaps the highest-stakes paraphilic disorder medicolegally — it is associated with contact and non-contact offences under POCSO and BNS. The disorder diagnosis does not reduce criminal culpability; it informs treatment mandates alongside punishment.
7. Fetishistic disorder: Sexual arousal from non-living objects or highly specific non-genital body parts. Medicolegal implications are limited unless the fetish involves acquiring items through theft or involves non-consenting persons.
8. Transvestic disorder: Sexual arousal from cross-dressing. Important note: this must be distinguished from transgender identity, which is NOT a disorder. Transvestic disorder is specific to sexual arousal from cross-dressing in a non-transgender person who experiences distress about it.
Other specified / unspecified paraphilic disorders: Including necrophilia (sexual arousal from corpses — criminal offence), zoophilia/bestiality (sexual arousal from animals — criminal offence under Indian law), and coprophilia/urophilia.
Provided image
SELF-CHECK
A 40-year-old man reports intense sexual arousal from wearing women's clothing. He is not transgender. He is not distressed by this behaviour and it has not harmed anyone. Under DSM-5, how should this be classified?
A. Transvestic disorder — the cross-dressing itself is the disorder
B. A paraphilia (fetishistic cross-dressing), not a disorder, because there is no distress and no harm to others
C. Gender dysphoria
D. Unspecified paraphilic disorder because it involves non-standard behaviour
Reveal Answer
Answer: B. A paraphilia (fetishistic cross-dressing), not a disorder, because there is no distress and no harm to others
DSM-5 distinguishes paraphilia from paraphilic disorder. Transvestic cross-dressing that causes no personal distress and harms no one is a paraphilia, not a disorder. The disorder diagnosis (transvestic disorder) requires clinically significant distress or impairment to the individual. The Navtej Johar principle applies: consensual adult behaviour that harms no one is legally and medically acceptable as a variant.
Medicolegal Implications and Consent
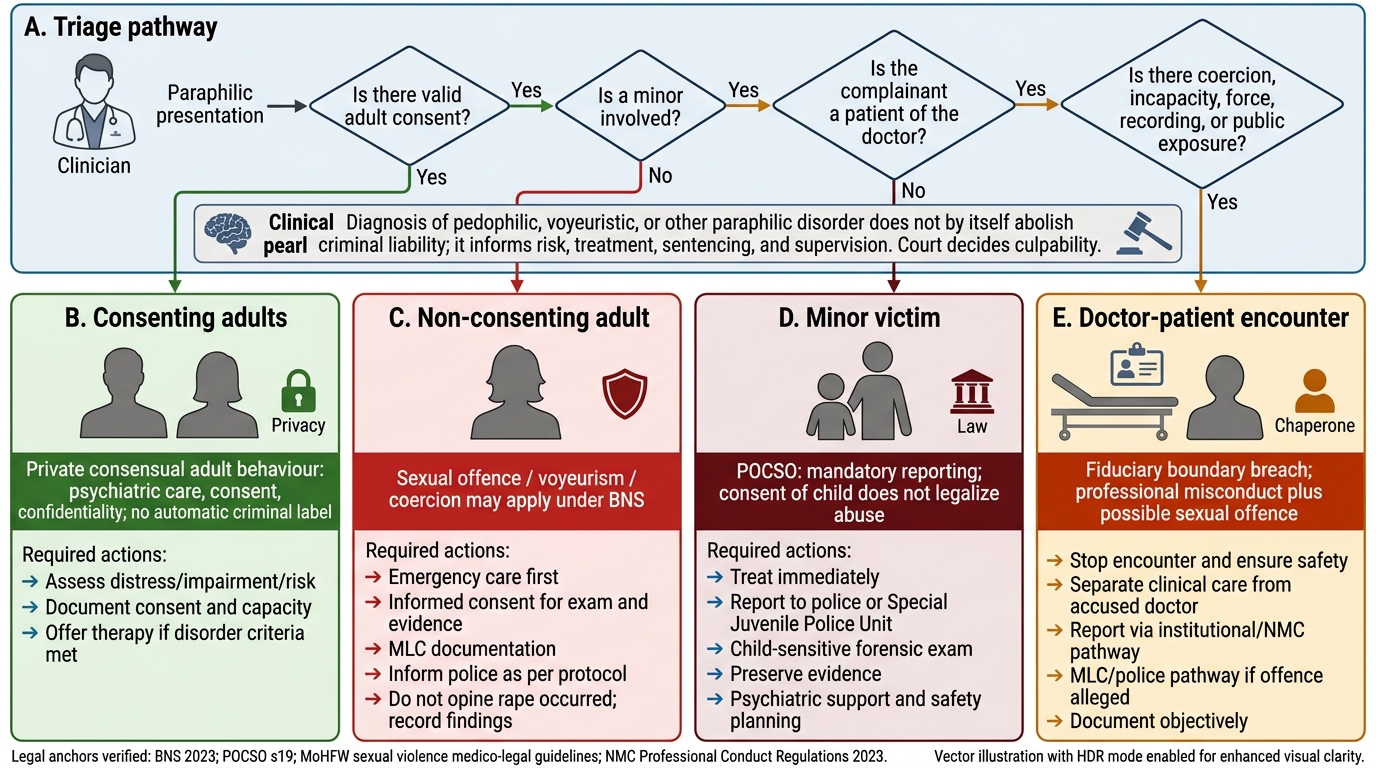
The medicolegal implications of paraphilic presentations cluster into four distinct scenarios, each requiring a different clinical and legal analysis.
Scenario 1: Paraphilic acts with consenting competent adults. Where two adults freely consent to, for example, sadistic/masochistic conduct, their sexual interaction is lawful (post-Navtej Johar). However, injury caused during such encounters may still present medicolegally — a person with bite marks, rope injuries, or lacerations presenting to an emergency without clarifying the consent context creates a potential misidentification of assault. Documentation of consent (ideally in writing for severe acts) and injury character is important. The doctor should not presume assault and should not presume consent — ask, in private, in a non-judgmental manner.
Scenario 2: Paraphilic acts with non-consenting adults. Non-consensual voyeurism, exhibitionism, frotteurism, or sadism are criminal offences irrespective of the psychiatric diagnosis. The presence of a paraphilic disorder is relevant to sentencing and treatment recommendations, but is not a complete defence to criminal liability in Indian law (IPC Section 84 / equivalent BNS defence of unsoundness of mind is rarely established for paraphilic disorders, because the person typically knows the act is wrong).
Scenario 3: Paraphilic disorder with a minor (paedophilic disorder). This is categorically criminal under POCSO and BNS regardless of any disorder diagnosis. The forensic clinician conducting a psychiatric assessment of a paedophilic offender is assessing for treatment recommendations and risk, not providing a defence framework. The risk assessment should address: likelihood of reoffending, insight into disorder, amenability to treatment (pharmacological — anti-androgens; psychological — cognitive-behavioural therapy), and recommendations for community supervision.
Scenario 4: Paraphilic disorder in a criminal defence context. When a court orders psychiatric evaluation to determine criminal responsibility, the forensic clinician applies the McNaughten criteria as adopted in Indian law: did the accused, at the time of the act, by reason of unsoundness of mind, not know the nature or quality of the act, or not know it was wrong? Most paraphilic disorders do not produce this degree of cognitive incapacity. The clinician's report must clearly state: (a) the diagnosis (if any), (b) whether the McNaughten threshold is met (almost invariably it is not for paraphilic disorders), and (c) treatment recommendations irrespective of criminal outcome.
Medicolegal Flowchart for Paraphilic Presentations
CLINICAL PEARL
Pedophilic disorder is a psychiatric diagnosis — but it is never a legal defence to acts of child sexual abuse in India. The doctor's role in these cases is to provide an accurate psychiatric assessment for the court (disorder present or absent), and a risk and treatability assessment for the benefit of sentencing considerations and post-conviction supervision. Never conflate disorder diagnosis with mitigation of culpability in the report; leave that inference to the court.
SELF-CHECK
A person is charged with voyeurism — installing a hidden camera in a toilet. Psychiatric assessment shows they meet DSM-5 criteria for voyeuristic disorder. Under Indian law (BNS equivalent), which statement is most accurate regarding criminal responsibility?
A. The psychiatric diagnosis provides a complete defence to criminal liability
B. The person is not criminally liable because voyeuristic disorder is a recognised psychiatric diagnosis
C. The psychiatric diagnosis does not abolish criminal liability; it is relevant to sentencing and treatment recommendations, but the McNaughten threshold is typically not met
D. The court must acquit the person and order compulsory psychiatric treatment
Reveal Answer
Answer: C. The psychiatric diagnosis does not abolish criminal liability; it is relevant to sentencing and treatment recommendations, but the McNaughten threshold is typically not met
A paraphilic disorder diagnosis does not constitute a defence of unsoundness of mind under Indian law. The McNaughten standard (BNS equivalent) requires that the person did not know the nature or quality of the act, or did not know it was wrong — a criterion virtually never met by paraphilic disorder alone. Criminal liability is typically upheld; the disorder informs sentencing and treatment planning.
SELF-CHECK
Which of the following paraphilic disorders invariably has criminal medicolegal implications under POCSO, regardless of whether the individual has acted on their urges?
A. Sexual masochism disorder
B. Fetishistic disorder
C. Pedophilic disorder — if the individual has had contact with a child
D. Transvestic disorder
Reveal Answer
Answer: C. Pedophilic disorder — if the individual has had contact with a child
Pedophilic disorder becomes criminally relevant under POCSO if there has been any contact (penetrative, non-penetrative, or harassment) with a child under 18. The disorder diagnosis alone, without any acted-upon conduct, is not a criminal offence — but it is a significant clinical finding requiring risk assessment and management.
KEY TAKEAWAYS
A paraphilia is an atypical sexual interest; a paraphilic disorder requires personal distress/impairment or harm to non-consenting persons, minors, or animals. DSM-5 specifies 8 paraphilic disorders: voyeuristic, exhibitionistic, frotteuristic, sexual masochism, sexual sadism, pedophilic, fetishistic, and transvestic disorders. ICD-11 maps similarly. Medicolegal implications range from none (paraphilia with consenting adults, no distress) to severe criminal exposure (pedophilic acts under POCSO, sadism with non-consenting adults). Paraphilic disorder diagnosis does not constitute a defence of unsoundness of mind in Indian law; the McNaughten standard is rarely met. The forensic clinician's report must address: diagnosis, McNaughten assessment, risk, and treatment recommendations — without conflating disorder with criminal defence.
REFLECT
A 28-year-old man is brought to your forensic clinic by court order following an arrest for groping women in a crowded metro station. He reports this is the fifth such incident and he cannot control the urge. He meets DSM-5 criteria for frotteuristic disorder. Write the key elements of your medicolegal report for the court: (1) diagnosis, (2) assessment of criminal responsibility under Indian law, (3) risk of reoffending, and (4) your recommendations.