Page 10 of 16
FM13.{7,10} | Analytical Toxicology & Bedside Tests — SDL Guide (Part 2)
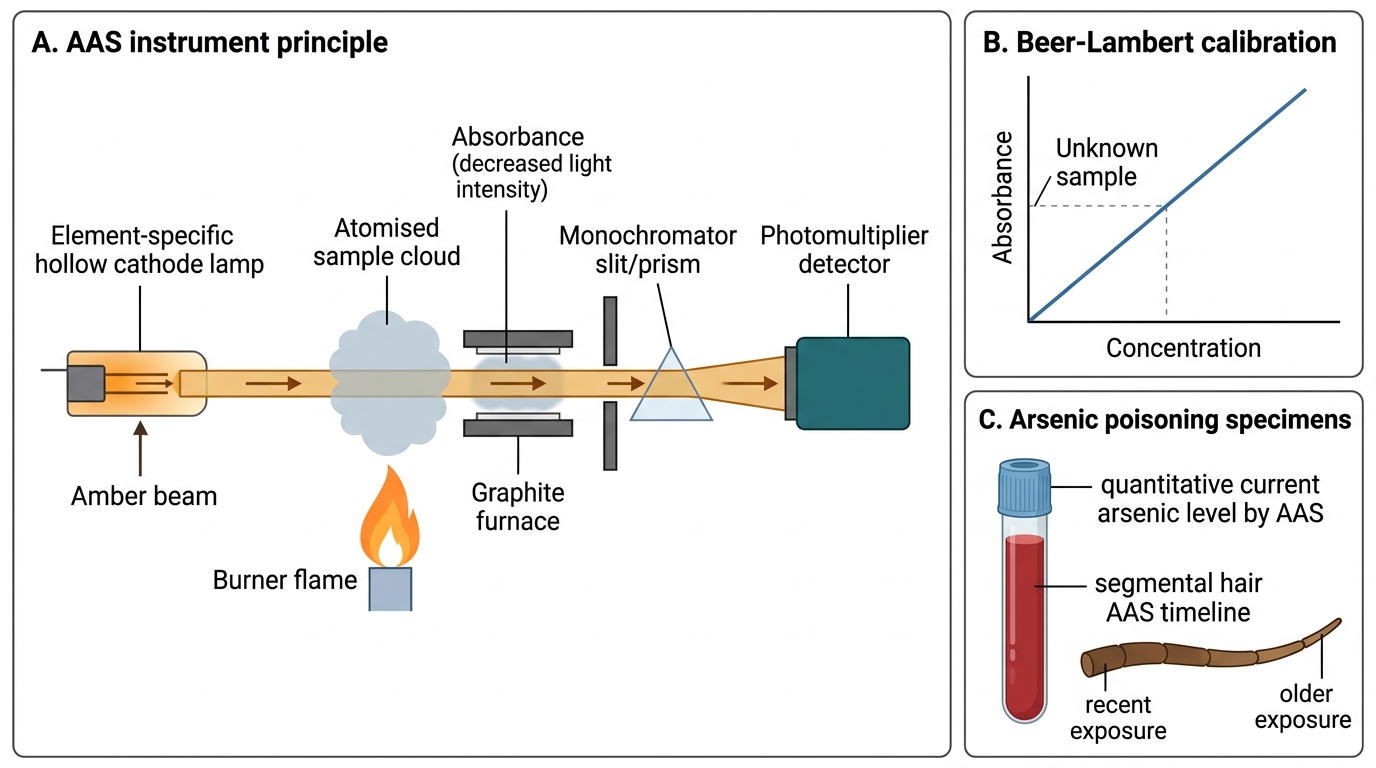
Atomic Absorption Spectroscopy for Metallic Poisons
Atomic Absorption Spectroscopy (AAS) is the definitive analytical technique for detecting and quantifying metallic poisons — arsenic, lead, mercury, thallium, copper, iron, barium, and cadmium — in biological specimens. It exploits a fundamental property of atomic physics: each element, when its atoms are in the ground state, absorbs light at precise, characteristic wavelengths that are unique to that element.
In AAS, the biological sample (blood, urine, or acid-digested tissue) is aspirated into a flame (flame AAS) or heated in a graphite furnace (graphite furnace AAS, or GFAAS — more sensitive). The heat converts metal compounds in the sample into free ground-state atoms. A hollow cathode lamp specific to the target element (e.g., an arsenic hollow cathode lamp for arsenic analysis) emits light at the element's characteristic absorption wavelength. The ground-state atoms in the flame absorb this light. The reduction in light intensity — measured by a photomultiplier detector — is proportional to the concentration of that element in the sample (Beer-Lambert Law). AAS is highly specific for the element being measured because the hollow cathode lamp emits only the target element's wavelengths — neighbouring elements in the periodic table do not interfere.
Flame AAS is adequate for most routine metallic poison analysis (detection limits in the microgram/mL range). Graphite furnace AAS (GFAAS) achieves detection limits in the nanogram/mL to picogram/mL range, making it suitable for trace metal analysis (e.g., arsenic in drinking water at the WHO guideline level of 10 µg/L) and for severely decomposed post-mortem specimens where the available sample is minimal.
Key applications in Indian forensic toxicology:
- Arsenic: the most commonly analysed metal in Indian FSLs; measured in blood, urine, hair (chronic exposure — hair grows ~1 cm/month, so arsenic distribution along hair length indicates the timeline of exposure — the 'arsenic time-line' used in homicide investigations), and nail samples
- Lead: blood lead level by GFAAS; hair and bone for chronic exposure
- Mercury: organic mercury (methylmercury) and inorganic mercury have different organ distributions; urine mercury for inorganic; blood mercury for organic
- Thallium: a rare but forensically important poison (tasteless, colourless, no immediate odour) — detected in urine by GFAAS
Critical limitation: AAS measures only the elemental form — it does not distinguish between different chemical forms of the same element (organic vs inorganic mercury; As³⁺ vs As⁵⁺ vs organic arsenic). This speciation (distinguishing chemical forms) requires additional techniques such as HPLC coupled to AAS (HPLC-AAS) or inductively coupled plasma mass spectrometry (ICP-MS). AAS also cannot identify organic compounds — it is specific to metals and metalloids. Attempting to use AAS for OP pesticides or pharmaceutical drugs would be inappropriate and produce no meaningful result.
Atomic Absorption Spectroscopy Principle
SELF-CHECK
The FSL analyst receives blood and hair samples from a suspected chronic arsenic poisoning case. Which analytical technique is most appropriate for quantitative arsenic determination, and which specimen provides information about the timeline of poisoning?
A. TLC on blood gives the arsenic level; hair is not useful for metal analysis
B. AAS on blood gives quantitative arsenic level; hair AAS with segmental analysis provides the timeline of exposure
C. GC-MS on blood gives the arsenic level; urine is the best specimen for timeline
D. ELISA on blood gives quantitative arsenic; hair provides the current level only
Reveal Answer
Answer: B. AAS on blood gives quantitative arsenic level; hair AAS with segmental analysis provides the timeline of exposure
AAS is the definitive quantitative method for arsenic (and all metallic poisons). Blood AAS gives the current arsenic level. Segmental hair analysis by AAS exploits the fact that hair grows approximately 1 cm/month — the distribution of arsenic along the length of a hair sample provides a timeline of exposure (arsenic deposited proximally = recent; distally = older exposure). This technique has been used in historical homicide investigations to reconstruct the duration of chronic arsenic administration. TLC and GC-MS are for organic compounds, not metals. ELISA is for antibody-based detection, not metal quantification.
Medicolegal Interpretation of Analytical Results
Receiving an FSL report that states 'paracetamol detected in blood at 420 mg/L' is only the beginning of the medico-legal analysis. Translating that chemical finding into a court-admissible interpretation requires understanding the chain of custody that validates the result, the reference ranges that contextualise it, and the known artefacts (particularly post-mortem redistribution) that may limit interpretation.
The chain of custody validation is the legal prerequisite for the analytical result to be admissible as evidence. If the chain-of-custody documentation accompanying the sample to the FSL has any gaps — an unsealed container, a missing signature, a mismatch between the case number on the label and the requisition form — the defence may successfully challenge the sample's integrity. The FSL report should explicitly state that the chain of custody was intact on receipt. As the autopsy surgeon who dispatched the sample, the physician may be called to testify about the integrity of the collection and dispatch procedure.
Reference ranges in poisoning: interpreted differently from clinical laboratory reference ranges. In toxicology, the relevant thresholds are:
- Therapeutic range: the concentration range associated with pharmacological effect without toxicity — relevant for therapeutic drug monitoring and for determining whether a 'therapeutic dose' was actually within the expected range
- Toxic range: the concentration range associated with signs of toxicity — relevant for confirming that a detected level is toxicologically significant
- Lethal range: concentrations reported in post-mortem cases — highly variable due to post-mortem redistribution
Post-mortem redistribution (PMR) is the most important interpretative challenge in forensic toxicology. After death, lipophilic basic amines (tricyclic antidepressants, opioids, cocaine, methadone, amitriptyline) diffuse from high-concentration tissue depots (lungs, liver, myocardium) into adjacent cardiac blood. This produces post-mortem blood concentrations several times higher than the antemortem concentration, potentially leading to an overestimate of the antemortem dose. Mitigation strategies: collect peripheral blood (femoral vein) rather than cardiac blood; measure vitreous humour (not affected by PMR) for corroboration; compare liver-to-blood ratio (a high ratio suggests PMR has occurred).
Negative FSL results: a negative result does not exclude poisoning. The FSL can only test for substances it was asked to screen for — if the requesting physician did not specify that a novel synthetic compound was suspected, the FSL may not have tested for it. Additionally, the detection window varies: urine drug screens for cannabis detect THC-COOH for up to 30 days in chronic users, but cocaine metabolite only for 2-4 days. A post-mortem specimen collected after prolonged resuscitation may have diluted blood concentrations below detection thresholds.
The FSL report in court: the FSL analyst who signs the report may be called as an expert witness to explain the methodology, the specificity of the analytical method, the chain of custody, and the interpretation of the findings. The forensic physician who performed the autopsy may be called separately to explain the clinical and anatomical context. These two expert witnesses together provide the complete chemical + anatomical picture — neither alone is sufficient.
CLINICAL PEARL
The co-oximetry trap and the TLC Rf confusion: Two bedside/laboratory test errors recur regularly in clinical and medico-legal practice. First: standard pulse oximetry gives falsely normal SpO₂ in CO poisoning — a normal SpO₂ in a cherry-red patient who smells of exhaust fumes is a false negative. Always request co-oximetry or ABG co-oximetry in any suspected CO case. Second: TLC Rf values are not unique identifiers — two different compounds may have identical Rf values on a given TLC system. TLC is a screening tool; a positive TLC result (correct Rf, correct visualisation reagent colour) is presumptive and must be confirmed by a second, independent method (GC-MS or LC-MS) before being cited in a court report as positive identification. This distinction — between a screening test and a confirmatory test — is one of the most important conceptual boundaries in forensic analytical chemistry, and failure to maintain it has led to wrongful convictions based on unconfirmed immunoassay or TLC results.
SELF-CHECK
The FSL reports 'TLC positive for alkaloid consistent with strychnine' in a case of suspected strychnine poisoning. The defence counsel argues this is insufficient for a conviction. What additional analysis is required, and why?
A. No additional analysis is needed — TLC with correct Rf value is definitive identification
B. AAS must be performed to confirm strychnine as strychnine is a metal
C. GC-MS or LC-MS confirmation is required because TLC Rf values are not unique identifiers — a second independent method is required before the result is admissible as definitive identification
D. A second TLC on the same plate with the same solvent system provides the required confirmation
Reveal Answer
Answer: C. GC-MS or LC-MS confirmation is required because TLC Rf values are not unique identifiers — a second independent method is required before the result is admissible as definitive identification
TLC is a screening test — a positive Rf value is presumptive, not definitive. Different compounds can share the same Rf value on a given chromatographic system. Legal standards for forensic identification require confirmation by a second, independent analytical method with higher specificity — typically GC-MS (mass spectrum provides a unique molecular fingerprint) or LC-MS/MS. AAS is for metallic poisons, not alkaloids. Repeating TLC on the same system does not provide independent confirmation. This principle — screening result requires confirmatory method for legal proceedings — is the cornerstone of forensic analytical chemistry.