Page 9 of 16
FM13.{7,10} | Analytical Toxicology & Bedside Tests — SDL Guide
Learning Objectives
- Describe simple bedside clinical tests to detect poison or drugs in a patient's body fluids (FM13.7)
- Describe the general principles of analytical toxicology and the workflow from sample receipt to court report (FM13.10)
- Explain the principles, applications, and limitations of TLC, GC, LC, and Atomic Absorption Spectroscopy (FM13.10)
- Interpret analytical results in a medico-legal context, including chain of custody and post-mortem redistribution
INSTRUCTIONS
Analytical toxicology translates the biochemical evidence of poisoning into court-admissible proof. As a physician, you need two distinct skill sets: the bedside tests you can perform yourself at the point of care within minutes, and the laboratory methods your FSL colleagues use to generate the definitive chemical evidence. Understanding both allows you to order the right tests, interpret reports correctly, and give reliable expert testimony. This module covers both scales — from a ferric chloride test on bedside urine to the mass spectrometer that produces the GC-MS chromatogram entered as Exhibit A in a murder trial.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology, 34th ed. (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology, 24th ed. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 22-year-old student is brought to the emergency department confused, with dilated pupils and a pulse of 130/min. His friends say he was at a party and 'took something.' No containers are available. The emergency physician has 10 minutes to make a clinical decision before the patient becomes unresponsive. She performs a urine dipstick (benzodiazepine screen: negative), checks the ECG (QRS 130 ms — widened), and examines the pupils with a light — markedly dilated, minimally reactive. Within 2 minutes of a rapid bedside assessment, she has a working diagnosis of tricyclic antidepressant (TCA) overdose. She starts sodium bicarbonate infusion. Three hours later, the FSL immunoassay confirms tricyclic antidepressants in the urine. The bedside diagnosis saved 3 hours of diagnostic uncertainty and likely the patient's life. The question is: which bedside tests give you this kind of decision-speed, and which are misleading?
WHY THIS MATTERS
Bedside tests are imperfect but time-critical tools for poison identification at the point of care, when laboratory results are unavailable. Knowing their false-positive and false-negative rates prevents anchoring on a bedside finding that is wrong. The FSL analytical methods — TLC, GC, LC, AAS — are the definitive evidentiary tools, and understanding their principles allows the physician to correctly specify which analysis to request, understand why some results take longer than others, and give credible court testimony about what the analytical findings mean. Without this knowledge, a physician called to testify will be unable to explain the basis of the chemical evidence.
RECALL
From your Year-1 Pharmacology: you recall that drugs are classified by polarity (lipid-soluble vs water-soluble), which governs their absorption and distribution. From Chemistry: you recall chromatographic principles — that compounds can be separated based on differential affinity for a stationary vs a mobile phase, and that atomic emission and absorption spectroscopy exploit element-specific wavelengths. From SDL tx4 (Autopsy and Viscera), you know the samples that arrive at the FSL and why their preservation matters. Today we follow those samples into the laboratory and understand what happens next.
Bedside Clinical Tests to Detect Poisons in Body Fluids
Bedside tests for poison detection are performed at the point of care, using simple chemical reactions or physical properties observable without laboratory equipment. They provide rapid qualitative guidance — not quantitative confirmation — and all have significant limitations that the physician must understand to avoid misinterpretation.
Ferric chloride (FeCl₃) test for salicylates: a few drops of 10% ferric chloride solution added to urine produces a purple or violet colour in the presence of salicylates (aspirin and its metabolite salicylic acid). This test is sensitive but not specific — phenothiazines (chlorpromazine, promethazine) and phenylpyruvic acid (phenylketonuria) also give a positive reaction. A positive result in the appropriate clinical context (suspected aspirin overdose, aspirin odour in gastric contents) is strongly supportive; a positive in a phenothiazine patient is a false positive. A negative result has reasonable negative predictive value for salicylate toxicity.
Examination of pupil size and reactivity is the most immediately available 'bedside test' and a critical discriminator: miosis (pupils <2 mm) = opioid or OP poisoning; mydriasis (pupils >7 mm) = anticholinergic, sympathomimetic, or TCA overdose. Pupils of 2-4 mm with reduced reactivity suggest sedative-hypnotic poisoning. This takes 5 seconds and provides immediate toxidrome direction.
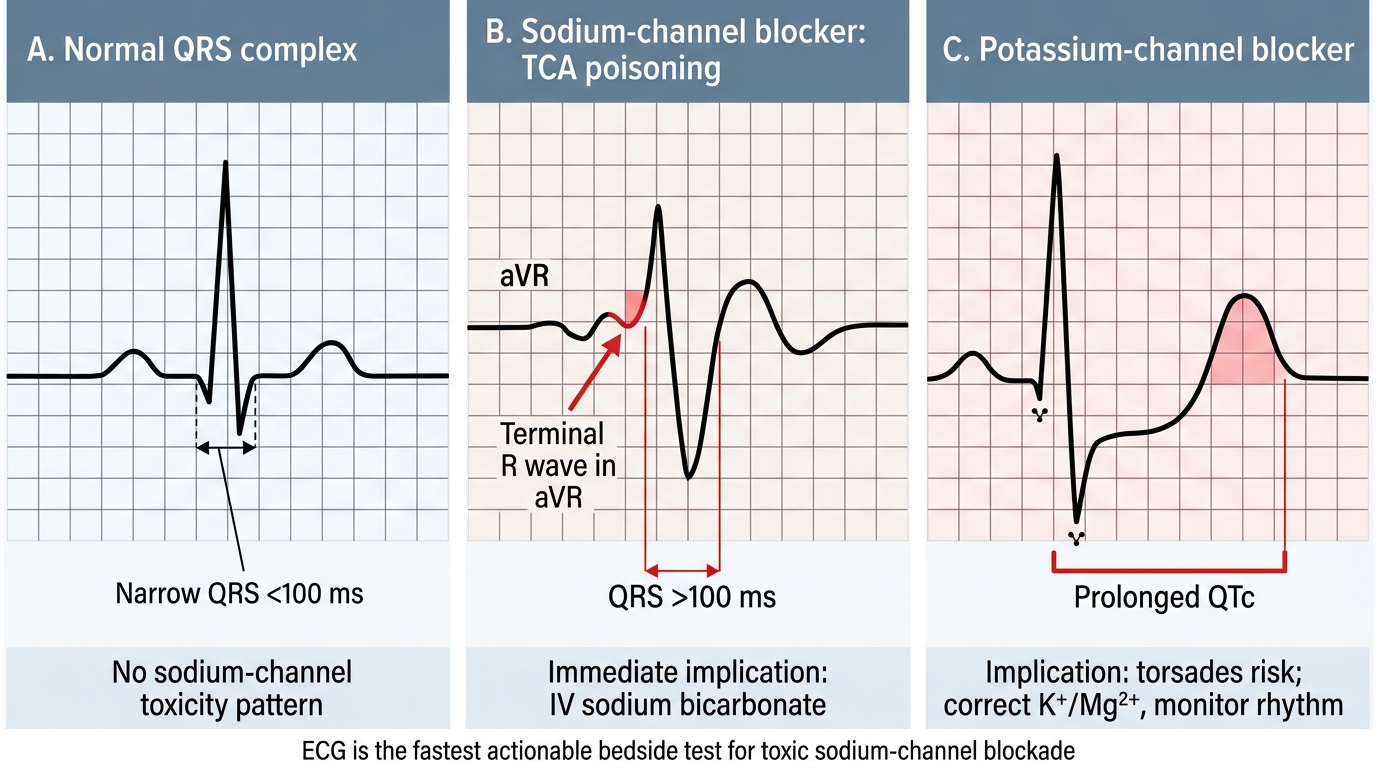
ECG is the most powerful single bedside investigation in undifferentiated poisoning. QRS widening (>100 ms) indicates sodium channel blockade — classic for tricyclic antidepressants (TCAs), but also seen with cocaine, class Ia antiarrhythmics (quinidine, procainamide), carbamazepine, and diphenhydramine. A terminal R wave >3 mm in aVR (a derivative of QRS widening) is specifically associated with TCA toxicity. QTc prolongation (>500 ms) indicates potassium channel blockade and torsades de pointes risk — seen with methadone, antipsychotics, antihistamines, macrolide antibiotics, and many toxins. Bradycardia with heart block = cardiac glycoside (digoxin, oleander) or beta-blocker toxicity.
Urine dipstick and lateral flow immunoassays: commercial point-of-care urine drug screens test for common drugs of abuse and their metabolites using antibody-based detection (immunoassay principle). They detect: opioids (morphine, codeine — heroin metabolises to morphine), benzodiazepines, cannabis (THC-COOH), cocaine metabolite (benzoylecgonine), amphetamines, and barbiturates. Critical limitations: cross-reactivity is common — quinine can test false-positive for opioids; some NSAIDs for cannabis; over-the-counter decongestants (pseudoephedrine) for amphetamines. These tests confirm a drug class, not a specific drug, and positive results require confirmation by GC-MS or LC-MS before use as legal evidence.
Pulse oximetry limitations in CO poisoning: standard pulse oximetry measures the ratio of oxygenated to total haemoglobin using two wavelengths. Carboxyhaemoglobin (HbCO) absorbs light at one of these wavelengths similarly to oxyhaemoglobin — it is therefore read as 'oxygenated haemoglobin' by a standard pulse oximeter, producing a falsely normal SpO₂ reading in CO poisoning. A patient with 30% HbCO may display SpO₂ 99% on a standard oximeter. Co-oximetry (a multi-wavelength spectrophotometric device or arterial blood gas analyser with co-oximetry capability) is required for accurate HbCO measurement.
Wood's lamp and urine fluorescence: ethylene glycol (antifreeze) poisoning — ethylene glycol is metabolised to calcium oxalate crystals in the renal tubules. Commercial antifreeze contains fluorescein as a leak detector; urine under ultraviolet (Wood's lamp) illumination may fluoresce if the patient ingested commercial antifreeze. This is a screening test only — absence of fluorescence does not exclude ethylene glycol poisoning (some formulations do not contain fluorescein).
Toxicology ECG Patterns and Immediate Management
Key bedside tests and their limitations:
• Ferric chloride = salicylates in urine (purple/violet) — false positive with phenothiazines
• ECG QRS widening = TCA/sodium channel blockade — fastest and most actionable test
• Pupil exam = toxidrome discriminator (miosis vs mydriasis)
• Urine immunoassay strips = drug class screening — not specific; confirmation needed
• Pulse oximetry = UNRELIABLE in CO poisoning — needs co-oximetry
• Wood's lamp urine = ethylene glycol screening (if fluorescein-containing antifreeze)
SELF-CHECK
A patient presents with suspected CO poisoning. His SpO₂ on pulse oximetry reads 98%. The physician reassures the family that oxygenation is normal. What is the critical error in this reasoning?
A. SpO₂ 98% is abnormally low and should prompt immediate intubation
B. Pulse oximetry cannot distinguish carboxyhaemoglobin from oxyhaemoglobin — a falsely normal SpO₂ does not exclude CO poisoning
C. The pulse oximeter probe was not correctly positioned
D. SpO₂ by pulse oximetry is the gold standard for CO diagnosis
Reveal Answer
Answer: B. Pulse oximetry cannot distinguish carboxyhaemoglobin from oxyhaemoglobin — a falsely normal SpO₂ does not exclude CO poisoning
Standard pulse oximetry uses two wavelengths and reads carboxyhaemoglobin (HbCO) as 'oxyhaemoglobin,' producing a falsely normal SpO₂ reading even in severe CO poisoning. A patient with 40% HbCO may have SpO₂ 99% by pulse oximetry while being in respiratory danger. Co-oximetry (multi-wavelength spectrophotometric analysis on an ABG machine or co-oximeter) is the only accurate method. The error is not probe positioning — it is a fundamental limitation of two-wavelength oximetry.
Principles of Analytical Toxicology
Analytical toxicology is the branch of toxicology concerned with the detection, identification, and quantification of foreign substances (poisons, drugs, metabolites) in biological and non-biological matrices. In the medico-legal context, the analytical workflow must satisfy both scientific requirements (accuracy, precision, sensitivity, specificity) and legal requirements (chain of custody, validated methods, documented quality control, expert interpretation).
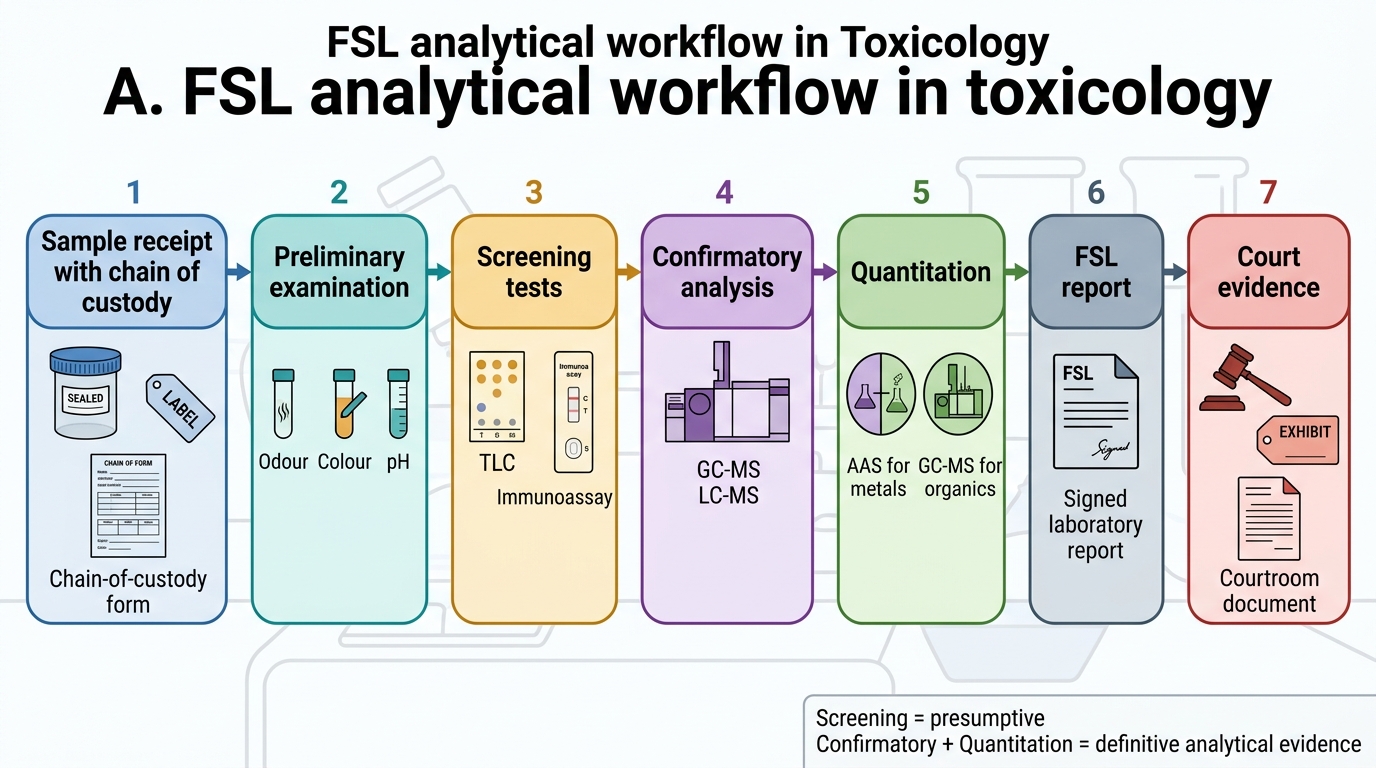
The analytical workflow in an Indian FSL typically proceeds through four sequential stages:
Stage 1 — Sample receipt and preliminary examination: the FSL analyst receives the sealed, labelled specimens from the police and checks that the chain-of-custody documentation is complete and unbroken. Any broken seal, mismatched labelling, or inadequate preservation is documented and may result in the sample being returned or its evidential weight being challenged in court. Preliminary examination includes: visual inspection (colour, consistency, odour), pH measurement, and preliminary chemical screening (reactions with acid, alkali, and indicator solutions that may indicate broad categories of substance).
Stage 2 — Sample preparation and extraction: biological matrices (blood, liver, urine) require extraction to isolate the poison from the complex biological medium before instrumental analysis. Common extraction methods: liquid-liquid extraction (LLE) — the toxin partitions into an organic solvent; solid-phase extraction (SPE) — the toxin is retained on a sorbent column then eluted; protein precipitation (acetonitrile, methanol) — proteins are removed, leaving analyte in the supernatant. Extraction efficiency and recovery must be validated.
Stage 3 — Screening: a broad, sensitive screening test identifies the class or classes of substances present. Immunoassay screening (ELISA, RIA, lateral flow) is used for drugs of abuse; TLC is used for alkaloid and drug class screening; colour reactions and spot tests are used for common poisons (Reinsch test for arsenic/antimony/mercury using a copper strip). Screening results are presumptive — they direct the analyst to the appropriate confirmatory method.
Stage 4 — Confirmation and quantification: confirmatory methods identify and quantify the specific compound with high specificity. These are the methods that generate the FSL report figures cited in court. The confirmatory method used depends on the class of substance and is described in the following sections.
The distinction between qualitative (present/absent) and quantitative (concentration) analysis is legally significant. A qualitative positive identifies the poison; a quantitative result (e.g., blood paracetamol 850 mg/L at 4 hours) allows the Rumack-Matthew nomogram to be applied and enables calculation of whether the detected concentration is consistent with the alleged exposure history. In post-mortem cases, quantitative results must be interpreted with caution given post-mortem redistribution.
FSL Analytical Workflow in Toxicology
Analytical Methods: TLC, GC and LC
The three chromatographic methods described in the FM13.10 competency — TLC, GC, and LC — are distinguished by their mobile phase (liquid or gas), their separation mechanism, and their application to specific compound classes. A fourth method, Atomic Absorption Spectroscopy (AAS), is covered separately as it is a spectroscopic rather than chromatographic technique.
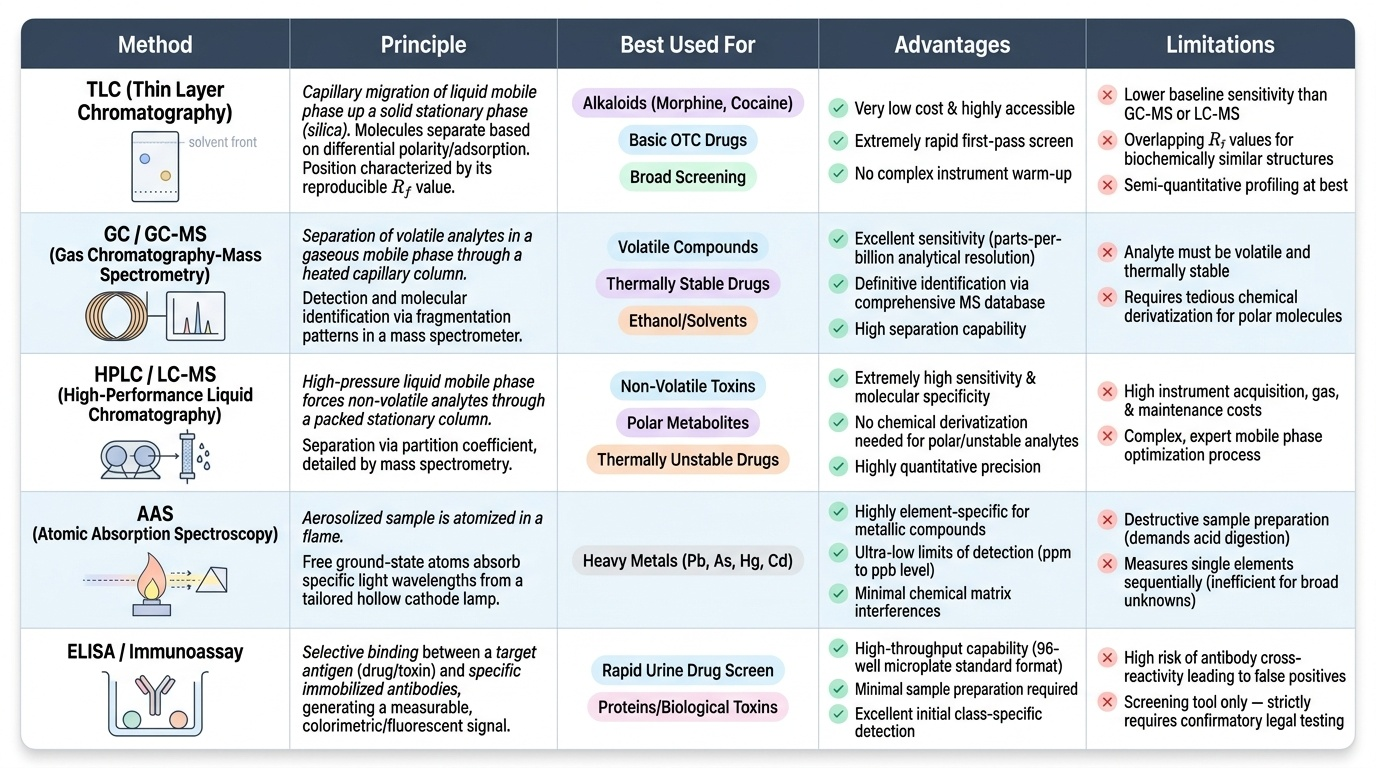
Thin Layer Chromatography (TLC) is the simplest, cheapest, and most widely accessible chromatographic method. In TLC, the stationary phase is a thin layer of silica (or alumina) coated on a glass, aluminium, or plastic plate. The sample extract is spotted at the base of the plate, which is then developed by standing it in a shallow pool of solvent (mobile phase). As the solvent migrates up the plate by capillary action, the compounds in the sample are carried with it at different rates determined by their polarity — polar compounds interact more with the silica (more retarded), non-polar compounds travel faster. After development, the plate is visualised by UV light (at 254 nm for UV-absorbing compounds) or by spraying with a chemical reagent (e.g., iodine vapour, ninhydrin for amino acids, Dragendorff reagent for alkaloids — produces orange spots). Each compound's position is characterised by its Rf value (distance migrated by compound ÷ distance migrated by solvent front) — a reproducible physical constant under standard conditions. TLC is used in Indian FSLs for: alkaloid screening (morphine, cocaine, quinine, strychnine, aconitine), basic drug screening (benzodiazepines, barbiturates, phenothiazines), and as a first-pass broad screen. Limitations: lower sensitivity than GC-MS or LC-MS; Rf values can overlap between structurally similar compounds; semi-quantitative at best.
Gas Chromatography (GC) separates compounds based on their volatility and interaction with the stationary phase in a heated column. In GC, the mobile phase is an inert carrier gas (helium, nitrogen, or hydrogen). The sample (in volatile form — either naturally volatile or chemically derivatised) is injected into a heated injection port, vaporised, and swept by the carrier gas through a long (15-30 m) capillary column coated with a liquid stationary phase. Separation occurs because different compounds spend different amounts of time dissolved in the stationary phase (stationary phase retention) versus carried in the gas phase — compounds with higher affinity for the stationary phase elute later (higher retention time). Detection is by flame ionisation detector (FID) (for most organic compounds) or mass spectrometer detector (MS) — the combination GC-MS is the gold standard confirmatory method for organic drug and poison identification. GC is the method of choice for: volatile compounds (ethanol, methanol, acetone, chloroform, carbon tetrachloride, petrol), drugs of abuse (opioids, amphetamines, cannabis metabolite THC-COOH, cocaine, benzodiazepines), organophosphate pesticides, and many pharmaceuticals in overdose.
Liquid Chromatography (LC), specifically High-Performance Liquid Chromatography (HPLC) and its combination with mass spectrometry (LC-MS or LC-MS/MS), is the most powerful and versatile confirmatory method for non-volatile, thermally labile, or high-molecular-weight compounds that cannot be analysed by GC. In LC, the mobile phase is a liquid solvent (aqueous/organic gradient). The sample is injected and separated on a packed column. Detection by UV (HPLC) or mass spectrometry (LC-MS). LC-MS/MS (triple quadrupole mass spectrometry) provides unparalleled specificity and can detect and quantify compounds at picogram concentrations — it is increasingly becoming the standard for forensic confirmation. LC applications: opioids (morphine, codeine, fentanyl, buprenorphine) and their glucuronide metabolites; benzodiazepines and metabolites; paracetamol; tricyclic antidepressants; many pesticides (paraquat, pyrethroids); and large-molecule toxins (ricin, abrin — using LC-MS/MS or immunoassay).
Provided image