Page 8 of 16
FM13.{5,9} | Medico-legal Duties & Autopsy in Poisoning — SDL Guide
Learning Objectives
- Describe medico-legal autopsy procedure in suspected poisoning cases including external and internal findings (FM13.5)
- Describe the correct preservation and dispatch of viscera for chemical analysis — which specimens, which preservatives, and critical contraindications (FM13.5)
- Describe the procedure for mandatory intimation of suspicious poisoning cases to the police (FM13.9)
- Outline the maintenance of medico-legal records and chain-of-custody documentation in poisoning cases (FM13.9)
INSTRUCTIONS
When a suspicious death reaches the post-mortem room, the forensic physician becomes the primary evidence gatherer for the criminal justice system. Every decision made at autopsy — which organs to examine, which samples to collect, which preservative to use — has downstream consequences for the FSL analysis and the legal outcome. This module covers the exact protocols mandated by Reddy's FM&T and Modi's Medical Jurisprudence: the viscera collection standards used in every Indian FSL-linked autopsy, the statutory reporting obligations, and the medicolegal record-keeping that makes evidence admissible in court.
References
- KSN Reddy — Essentials of Forensic Medicine & Toxicology, 34th ed. (textbook)
- BV Subrahmanyam — Modi's Medical Jurisprudence and Toxicology, 24th ed. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 55-year-old man is found dead at home by his wife. The police observe a half-empty cup of tea near the body. He had no known illness and was last seen alive 8 hours ago. The police request a medico-legal autopsy. The assistant at the mortuary, in a hurry, places all the viscera — stomach, liver, kidney, brain — into a single container of 10% formalin (the standard fixative used for histology). The FSL analyst receives the sample and immediately rejects it. The reason: formalin has destroyed all volatile compounds in the stomach contents and cross-linked the proteins in the liver, making it impossible to detect any organic poison by gas chromatography or most other analytical methods. The case goes cold. One incorrect preservative choice has potentially allowed a homicidal poisoning to go unpunished.
WHY THIS MATTERS
The medico-legal autopsy in poisoning is unique among forensic examinations in that its primary purpose is evidence collection for chemical analysis, not merely clinical diagnosis of cause of death. The clinical findings at autopsy may be non-specific or absent — many poisons leave no macroscopic signature. The FSL chemical analysis is therefore the definitive arbiter, and its validity is entirely dependent on the quality of the specimens delivered to it. A single error in preservation — formalin instead of saturated NaCl — can render months of investigation worthless. This module gives you the exact protocol per Reddy's FM&T, the statutory framework for your reporting duties, and the documentation standards that make your evidence court-admissible.
RECALL
From SDL tx2 (Classification and Toxicokinetics), you recall the ADME framework — that volatile organic compounds (ethanol, organophosphates, chloroform) are rapidly distributed and excreted; that metals (arsenic, lead, mercury) concentrate in organs; and that post-mortem redistribution affects blood drug concentrations. From SDL tx1, you know the chain-of-custody concept and that all medico-legal samples require labelling, sealing, and police co-witnessing. Today we apply these principles to the specific procedural requirements of the post-mortem examination in suspected poisoning.
Post-mortem Findings in Poisoning Cases
The post-mortem examination in a suspected poisoning case must be conducted with a higher degree of systematic thoroughness than in non-suspicious deaths, because subtle findings that would be dismissed in a routine autopsy may be the only macroscopic evidence of poisoning. The examination proceeds from external to internal, and every significant finding must be documented with precision — photographs, measurements, and anatomical descriptors — before any tissue is removed.
Provided image
External examination begins with the scene documentation (provided by the police) and proceeds to the body. The most important external findings in poisoning include:
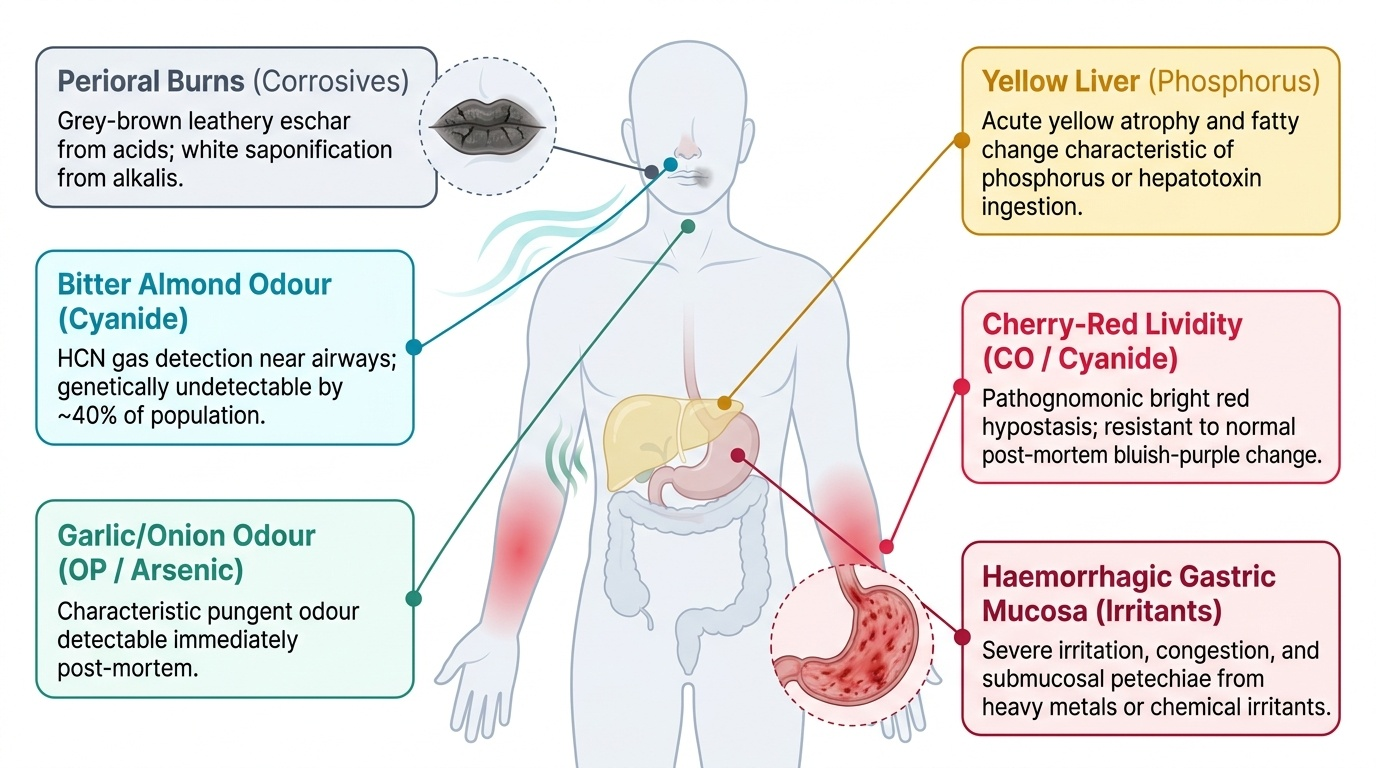
Lividity (post-mortem hypostasis): the colour and distribution of lividity provides early diagnostic clues. Cherry-red lividity — visible even through fixed blue-grey skin — is pathognomonic of carbon monoxide (CO) poisoning because carboxyhaemoglobin (HbCO) is bright red and resistant to the post-mortem bluish-purple colour change of deoxyhaemoglobin. The same cherry-red colour is produced in cyanide poisoning (histotoxic hypoxia — venous blood remains oxygenated). Grey-brown or chocolate-brown discolouration of lividity suggests methaemoglobinaemia (nitrites, dapsone, benzocaine). Normal dark lividity does not exclude poisoning.
Perioral and perinasal findings: corrosive acid ingestion produces grey, black, or brown chemical burns and coagulative necrosis around the lips and angles of the mouth; the burns are hard and leathery (eschar formation). Strong alkali ingestion (NaOH, KOH) produces softer, white or greyish saponification burns that spread along the mucosa. Both types may also show burns on the tongue, palate, and anterior pharynx. Frothy secretions at the mouth and nostrils suggest pulmonary oedema from irritant gas inhalation (paraquat, phosgene, chlorine).
Odours are valuable early clues but must be documented immediately (they dissipate quickly post-mortem): garlic or onion odour = organophosphate or arsenic; bitter almond odour = hydrogen cyanide (HCN) — note that 40% of people are genetically unable to detect this odour; alcohol odour = ethanol; petroleum odour = hydrocarbon ingestion; acetone/fruity odour = methanol or isopropanol metabolite.
Internal examination provides the critical organ-level evidence:
The stomach and its contents are the most important single specimen in suspected oral poisoning. The stomach must be opened carefully over a clean dissecting board, and the contents — their volume, colour, odour, consistency, and any identifiable tablet fragments, plant material, or chemical residue — must be documented and fully preserved. The gastric mucosa is examined for: patchy haemorrhage (irritant poisons — arsenic, antimony), diffuse sloughing (strong acids — produces 'tanning' and tough, leathery mucosa from coagulation), softening and friability (strong alkalis — saponification), or no macroscopic change (most organic poisons, including OPs and many medications).
Liver findings: yellow discolouration with greasy, yellow-orange fatty change of the hepatic parenchyma is characteristic of phosphorus poisoning (the classic 'phosphorus liver' — may glow faintly green in the dark due to oxidation products), paracetamol hepatotoxicity (centrilobular necrosis — pale yellow-white zones), and carbon tetrachloride (CCl₄) poisoning. In arsenic poisoning, the liver may show congestion, steatosis, and periportal fibrosis in chronic cases.
Kidney findings: renal cortical pallor, swelling, and waxy consistency with petechial haemorrhage in the cortex suggests ethylene glycol or mercuric chloride nephropathy. Oxalate crystals may be visible as white streaks in the renal parenchyma (ethylene glycol).
Lung findings: oedematous, congested, heavy lungs with frothy fluid = pulmonary irritant or aspiration; paraquat characteristically produces progressive pulmonary fibrosis with a 'wet cement' consistency on cut section.
Viscera Collection, Preservation and Dispatch for Chemical Analysis
The collection, preservation, and dispatch of viscera to the Forensic Science Laboratory (FSL) is the most procedurally critical component of the medico-legal autopsy in poisoning. Errors at this stage are irreversible — incorrect preservatives destroy analytical targets permanently, and insufficient quantities make quantitative analysis impossible. The following protocol is per Reddy's FM&T, which represents the current Indian standard.
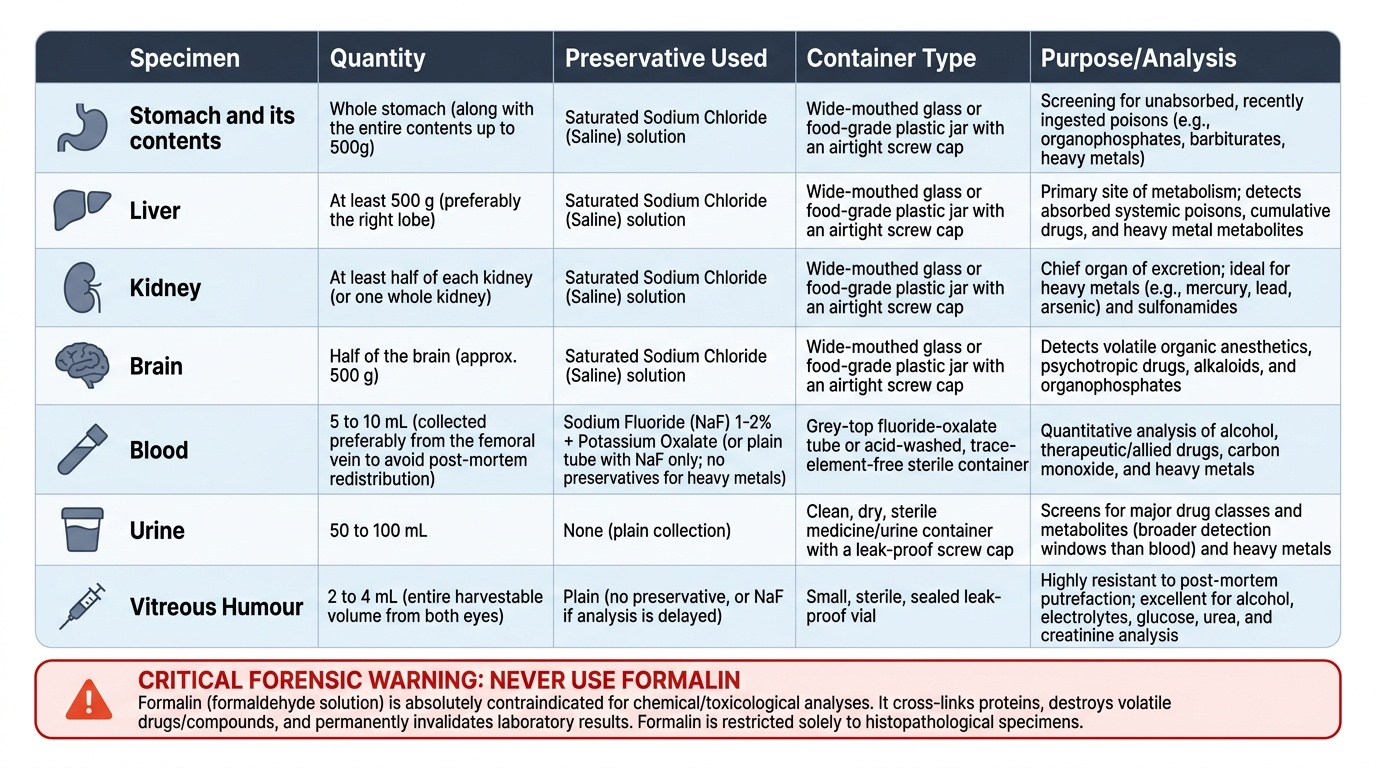
The fundamental rule: FORMALIN IS ABSOLUTELY CONTRAINDICATED for any specimen destined for chemical (toxicological) analysis. Formalin (formaldehyde solution, 10% in water = '10% neutral buffered formalin') cross-links proteins through methylene bridges and destroys all volatile organic compounds. Its use in histopathological specimens is correct; its use in forensic toxicological specimens is a serious error that invalidates the analysis. The preservatives used for toxicological analysis are:
1. Blood: collected in two separate containers:
- For alcohol, drug, and general toxicological analysis: fluoride-oxalate tube (grey-top) — sodium fluoride (NaF) at a concentration of 1-2% inhibits glycolysis (preventing post-mortem glucose fermentation that can generate spurious ethanol) and is bacteriostatic; oxalate anticoagulates. Volume: at least 5-10 mL. Alternatively, blood can be collected in plain tubes with NaF (without oxalate).
- For heavy metal analysis: trace-element-free tube or acid-washed container (no rubber stopper containing metal contaminants).
Source sites: femoral vein blood is preferred over cardiac blood for toxicological analysis because it is less subject to post-mortem redistribution — the phenomenon where lipophilic drugs (particularly basic amines like tricyclics, opioids, amphetamines) diffuse from organs into adjacent cardiac blood post-mortem, falsely elevating apparent concentrations. Cardiac blood levels of these drugs significantly overestimate antemortem levels.
2. Urine: collected in a plain, clean container (no preservative) — 50-100 mL. Urine is valuable for drug metabolites (many drugs are extensively metabolised before reaching urine; metabolite detection windows are longer than parent compound) and for some metals.
3. Vitreous humour: 2-4 mL collected from each eye using a syringe, preserved in a plain container (NaF is acceptable). Vitreous humour is particularly valuable because it is protected from post-mortem redistribution (the vitreous cavity is anatomically isolated from the central circulation), making it the most reliable specimen for alcohol quantification, electrolyte analysis, and some drug levels in decomposed or redistributed cases.
4. Stomach and its contents: the entire stomach is ligated at both ends before opening, then removed intact. The contents are carefully poured into a plain, clean wide-mouth glass jar — no preservative (preservative may interfere with analytical chemistry). Volume of contents to be documented. The stomach wall (gastric mucosa) is submitted as a separate specimen in saturated NaCl.
5. Liver, kidney, brain: each collected as large specimens (liver: 500 g from the right lobe; kidney: one whole kidney; brain: approximately half). Preserved in saturated sodium chloride (NaCl) solution OR rectified spirit (90% ethanol). The choice between these two preservatives depends on the suspected poison:
- If ethanol itself is the suspected poison, do NOT use rectified spirit (ethanol preservative will contaminate the sample) — use saturated NaCl instead.
- If volatile poisons (chloroform, ether, organophosphates, petrol) are suspected, saturated NaCl is preferred over rectified spirit (alcohol-based preservative may interfere with GC analysis of some volatiles).
- For most other organic poisons (alkaloids, drugs, metals), both saturated NaCl and rectified spirit are acceptable.
6. Small intestine: approximately 30 cm from the duodenojejunal flexure (to capture slow-release material not yet in the stomach), preserved in saturated NaCl or rectified spirit (same rules as above).
Labelling and sealing: each container must be labelled with: patient name, age, MLC number, case number, date and time of collection, type of specimen, autopsy surgeon's name, and autopsy centre. Each container must be sealed with the physician's seal (or court seal) in the presence of a police officer (ideally the investigating officer). The seal prevents tampering and establishes chain of custody. The label must be signed by both the autopsy surgeon and the police officer present.
Dispatch to FSL: all specimens are packed together in a wooden box or durable container, with padding to prevent breakage. The outer package is sealed, labelled with the FSL address and case details, and dispatched by the investigating police officer (not by hospital staff alone). A detailed covering letter (FSL requisition) must accompany the samples, specifying: the clinical and autopsy findings, the suspected poison(s), and the specific analyses requested.
Provided image
SELF-CHECK
At autopsy of a suspected alcohol-poisoning death, the mortuary technician asks which preservative to use for the liver specimen being sent to the FSL. Which is the correct choice and why?
A. 10% formalin — standard histological preservative
B. Rectified spirit (90% ethanol) — best preservative for organic compounds
C. Saturated sodium chloride (NaCl) solution — formalin destroys analytical targets; rectified spirit must not be used when ethanol is the suspected poison
D. Plain container without preservative — no preservative is needed for liver
Reveal Answer
Answer: C. Saturated sodium chloride (NaCl) solution — formalin destroys analytical targets; rectified spirit must not be used when ethanol is the suspected poison
When ethanol (alcohol) is the suspected poison, rectified spirit (which contains ethanol) must NOT be used as the preservative because it will contaminate the specimen and produce a falsely elevated ethanol result on FSL analysis. Saturated NaCl is the correct preservative. Formalin is absolutely contraindicated for any specimen sent for toxicological chemical analysis — it destroys volatile compounds and cross-links proteins. A plain container without preservative allows putrefactive bacteria to ferment glucose to ethanol, generating a spurious positive.
Mandatory Intimation of Suspicious Cases to Police
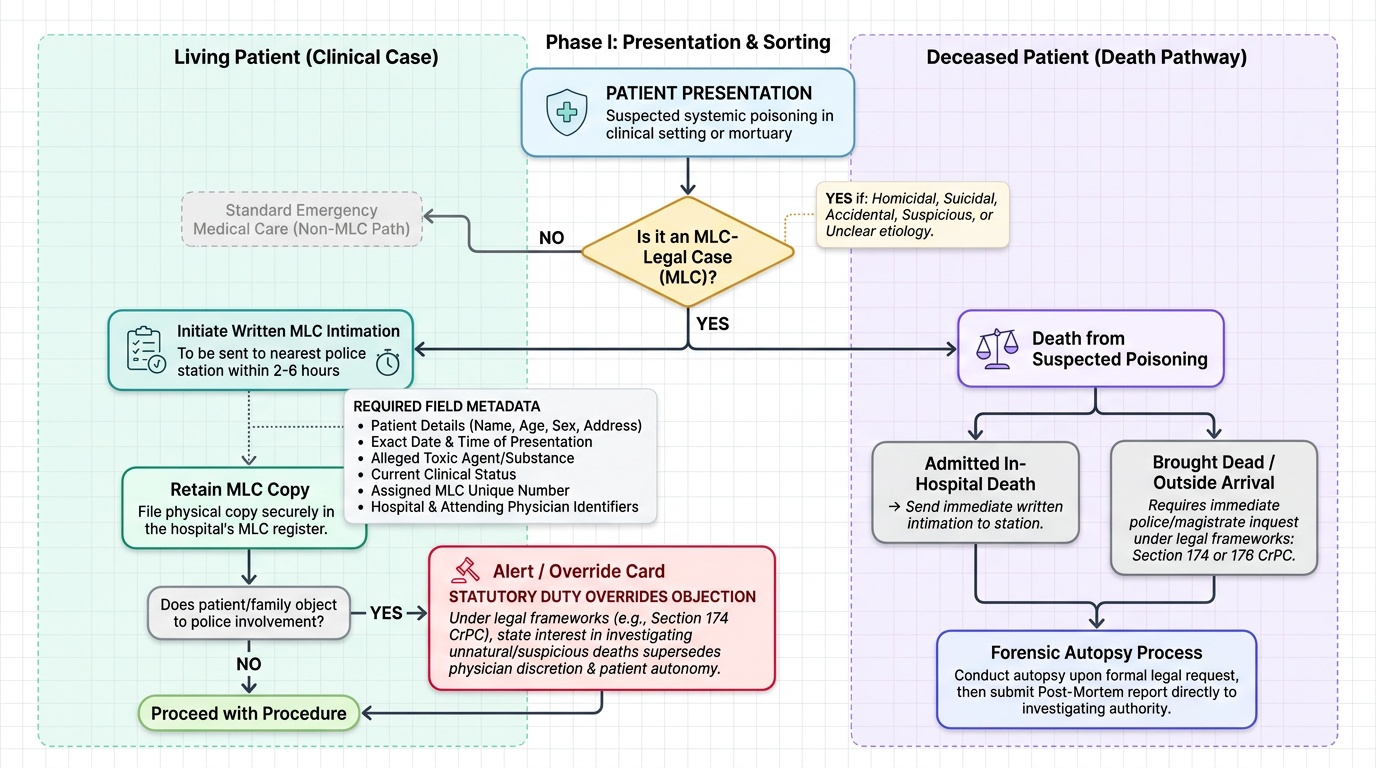
The obligation to inform the police of suspected poisoning deaths is a statutory duty that applies to all medical practitioners who encounter such cases — whether in a clinical setting (emergency department, ward) or at post-mortem. This duty exists because the state has an independent interest in investigating unnatural and suspicious deaths, which supersedes the individual physician's discretion and the family's preferences.
The relevant legal framework for police intimation derives from the Code of Criminal Procedure, 1973 (CrPC). Under Section 174 CrPC, when any person dies under circumstances suggesting suicide, homicide, accident, or under suspicious circumstances, the police officer in charge of the local station is empowered and obligated to hold an inquiry. The medical officer's role is to inform the police when a death (or a surviving patient with a life-threatening poisoning) meets these criteria. For deaths occurring in hospital after admission for poisoning, the physician must send a written intimation to the nearest police station as soon as poisoning is suspected as a significant factor.
For deaths that occur outside a hospital and are brought directly to the mortuary, the police typically initiate the request for autopsy through a police inquest under Section 174 CrPC (or a magistrate's inquest under Section 176 CrPC for cases requiring higher scrutiny — deaths in police custody, deaths of unknown identity, or cases of public concern). The forensic physician performs the autopsy in response to this formal request and submits the post-mortem report to the requesting authority. The physician does not report to the police independently in these cases — the police already have jurisdiction.
For clinical cases (living patients in hospital who are suspected poisoning victims): the physician must send a written MLC intimation to the nearest police station promptly. In practice, this should happen within 2-6 hours of the patient's presentation. The intimation must include: patient's name, age, sex, address (if known), date and time of hospital presentation, alleged substance, current clinical condition, MLC number, and the hospital/physician's details. A copy must be retained in the MLC register.
When does the duty arise? The duty to intimate arises whenever there is a reasonable suspicion of poisoning — it does NOT require a confirmed diagnosis. The threshold is low by design: a patient presenting with an altered level of consciousness and an unknown agent is an MLC. An agricultural worker presenting with cholinergic toxidrome is an MLC. A patient presenting with 'accidental' medication overdose is an MLC. The physician does not need to determine intent or substance identity before reporting — that is the investigating officer's job.
Provided image
Specific considerations:
- Patient objects to police notification: the physician's statutory duty overrides patient objection in MLC cases. Document the patient's objection in the notes, and proceed with notification.
- Family requests secrecy: same principle — statutory duty takes precedence.
- Death before police arrives: notify the police of the death; do not move the body until the police have attended and directed the next steps.
Maintenance of Medico-legal Records in Poisoning
The medico-legal record in a poisoning case is a legal document from the moment of its creation. Its legal weight in subsequent criminal or civil proceedings depends entirely on its contemporaneous nature, completeness, accuracy, and the identifiable signatures of the physician and witnessing officers. Record-keeping errors that would be trivial in a routine clinical case become potentially outcome-determining in a criminal trial.
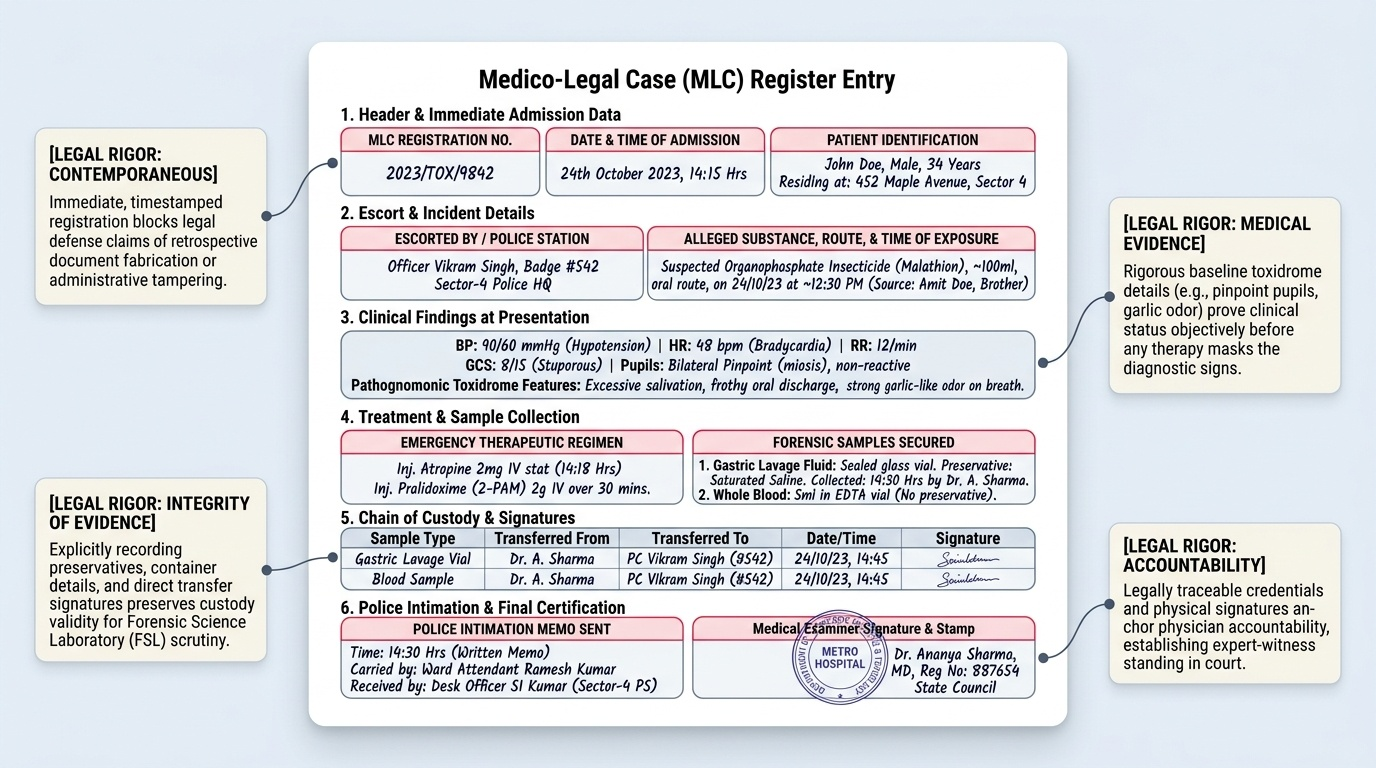
The MLC register is the central record-keeping document for all medico-legal cases in hospital. Each entry must include:
- MLC serial number (assigned on admission)
- Date and time of registration
- Patient name, age, sex, address (as available)
- Name of the police officer accompanying and their station
- Alleged substance, quantity, route, and time of exposure (with source attribution)
- Clinical findings at presentation (full vital signs, GCS, pupil findings, relevant toxidrome features, burns, odours)
- Treatment initiated (with timing)
- Samples collected (with container type, preservative, time, collector's identity)
- Chain-of-custody details (who received each sample, signed and witnessed)
- Police intimation: time, mode (written/telephonic), receiving officer's name and station
- Any change in patient condition
For the post-mortem report (autopsy in poisoning cases), the document must be structured to serve both medical and legal functions. Standard sections include: case details (name, age, date of death, autopsy number), circumstances as supplied by police, external examination findings (documented in anatomical order), internal examination findings (organ weights, macroscopic findings), specimens collected (complete list with preservative and FSL dispatch details), cause of death opinion, and the forensic physician's signature, date, and designation. The cause of death in a suspected poisoning case, pending FSL results, is stated as 'pending chemical analysis of viscera' — it is not appropriate to commit to a specific poison as cause of death before the FSL report.
The FSL request (chemical examination form) must specify clearly which analytical tests are requested and why. An under-specified FSL form (e.g., 'please analyse viscera for poison' without specifying the suspected class) may result in a standard screen that misses the specific toxin. The autopsy surgeon should specify: suspected poison class, specific compound if known, and any negative findings that rule out certain classes.
Long-term record retention: MLC registers are retained for a minimum of 10 years in most Indian states (state government rules vary). Post-mortem reports are permanent records. All chain-of-custody documents must be retained until the conclusion of any criminal proceedings, which may span years.
Provided image
Legal weight of medico-legal records: records created contemporaneously (at the time of examination) by a certified medical officer are considered prima facie evidence under Section 65B of the Indian Evidence Act 1872 (as amended). A record created after the fact, or altered, loses this evidential status and exposes the physician to charges of fabrication. The physician may be called to court as an expert witness to explain their findings — contemporaneous, legible, signed records are the foundation of credible expert testimony.
Consumer Protection Act 2019 and NMC Act 2020 implications: failure to maintain adequate MLC records constitutes deficiency in service under the CPA 2019 and professional misconduct under the NMC Act 2020. These statutes form the contemporary accountability framework — physicians must be aware that the 1986 CPA and the 1956 IMC Act are no longer operative and that the current standards are higher.
CLINICAL PEARL
The two preservative traps every FM student must own: (1) Never use formalin for toxicological specimens — this is the single most damaging error in forensic toxicology sample handling. Formalin is correct for histology and wrong for chemical analysis. If you remember nothing else from this module, remember this. (2) Do not use rectified spirit when ethanol is the suspected poison — for alcohol poisoning deaths, the solid viscera must go into saturated NaCl only. These two rules together define the correct preservative choice for all scenarios. A third trap: vitreous humour is not routinely collected in many hospitals but is diagnostically invaluable. It is resistant to post-mortem redistribution, protected from decomposition-related ethanol generation, and provides electrolyte values that are meaningful well after death (vitreous potassium can estimate time since death). Always collect vitreous humour in any suspicious death — it costs nothing and can save the investigation.
SELF-CHECK
At the time of autopsy for a suspected organophosphate poisoning, which of the following specimens and preservative combinations is CORRECT per Indian FSL standards?
A. Liver 500 g in 10% formalin; stomach contents in rectified spirit; blood in plain tube
B. Liver 500 g in saturated NaCl; stomach contents in plain clean jar; blood in sodium fluoride tube
C. Liver 500 g in rectified spirit; stomach contents in 10% formalin; urine in sodium fluoride tube
D. Liver 500 g in saturated NaCl; stomach contents in 10% formalin; blood in plain tube
Reveal Answer
Answer: B. Liver 500 g in saturated NaCl; stomach contents in plain clean jar; blood in sodium fluoride tube
For OP poisoning: liver in saturated NaCl (correct; formalin is absolutely prohibited; rectified spirit is acceptable for OP but NaCl is preferred as OP compounds are volatile and alcohol-based preservative may interfere with some GC analyses); stomach contents in a plain clean jar with no preservative (correct; preservatives interfere with chemical analysis of contents); blood in NaF tube (correct; NaF prevents spurious ethanol generation and glycolysis; required for drug/toxin analysis). Urine goes in a plain container — not NaF.
SELF-CHECK
A forensic physician performing an autopsy on a suspected homicidal poisoning case finds that the chain-of-custody seal on the viscera containers was broken before they were handed to the FSL analyst. What is the likely consequence for the criminal case?
A. The FSL analysis result is still fully admissible as long as the FSL analyst certifies the containers arrived
B. The admissibility of the FSL result may be successfully challenged by the defence, potentially rendering the chemical evidence inadmissible
C. The broken seal only affects the viscera — blood results in a separately sealed tube remain unaffected and fully admissible
D. The physician who initially sealed the containers is automatically acquitted of any professional responsibility
Reveal Answer
Answer: B. The admissibility of the FSL result may be successfully challenged by the defence, potentially rendering the chemical evidence inadmissible
An unbroken chain of custody is the legal prerequisite for forensic evidence admissibility. A broken seal raises the possibility of tampering — even if no actual tampering occurred, the defence can successfully argue that the integrity of the specimen cannot be guaranteed. Courts may exclude or significantly discount the FSL analytical result. This is why each container must be sealed in the presence of a police officer, with matched documentation in the MLC register and the FSL requisition. The physician who correctly sealed and documented the containers at dispatch is not automatically liable for downstream custody breaks, but they must be able to testify to the integrity of their own actions.
KEY TAKEAWAYS
The medico-legal autopsy in poisoning requires systematic documentation of external and internal findings. Key post-mortem signatures: cherry-red lividity (CO, cyanide); perioral burns (corrosives — grey coagulative = acid, soft white saponification = alkali); yellow liver (phosphorus, paracetamol, CCl₄); haemorrhagic gastric mucosa (irritants — arsenic, antimony); characteristic odours (garlic = OP/arsenic; bitter almond = cyanide — cannot be detected by 40% of people genetically).
Viscera collection per Reddy's FM&T: stomach + contents (plain jar), liver 500 g, kidney (whole), brain (half) — preserved in saturated NaCl or rectified spirit (NOT formalin; NOT rectified spirit if ethanol is the suspected poison); blood 10 mL in NaF tube (femoral vein preferred over cardiac — avoids post-mortem redistribution artefact); urine 50-100 mL in plain container; vitreous humour 2-4 mL plain. All containers labelled, sealed, police co-witnessed — chain of custody documented in MLC register.
Mandatory intimation: statutory duty under CrPC; arises at reasonable suspicion (no confirmed diagnosis required); written intimation to nearest police station; patient/family objection does NOT override the duty. MLC records: contemporaneous, signed, complete; MLC register documents all actions and chain-of-custody; post-mortem report states cause of death as 'pending FSL chemical analysis' until results available; records retained ≥10 years. Professional accountability: NMC Act 2020 (not IMC 1956) and Consumer Protection Act 2019 (not CPA 1986).
REFLECT
Return to the opening scenario. The forensic physician had to explain in court why the formalin-preserved viscera could not be analysed. If you were that physician, what would be your legal exposure under the NMC Act 2020 and CPA 2019? What quality assurance system could a hospital mortuary implement to prevent this specific error? And at a systems level: India has hundreds of district hospital mortuaries. Given the known frequency of this preservation error in the literature, what is the single highest-impact intervention — training, checklist, procurement policy, or regulatory change — that would most effectively eliminate formalin from toxicological sample containers across the country?