Page 15 of 25
IM1.{21-24,27} | Heart Failure Management and Procedures — SDL Guide
Learning Objectives
- Describe and prescribe non-pharmacological management of heart failure including sodium restriction, fluid management, and physical activity guidelines
- Discuss the pharmacology, indications, and contraindications of drugs used in heart failure — diuretics, ACE inhibitors, beta-blockers, aldosterone antagonists, and cardiac glycosides
- Enumerate the indications for valvuloplasty, valvotomy, coronary revascularisation, and cardiac transplantation
- Develop and document a structured management plan for a patient with heart failure based on EF category and underlying aetiology
- Demonstrate correct technique for intramuscular injection with appropriate patient communication
INSTRUCTIONS
The management of heart failure has been transformed over the past three decades by neurohormonal modulation — the recognition that the compensatory activation of the renin-angiotensin-aldosterone system and the sympathetic nervous system, while transiently adaptive, is ultimately cardiotoxic and accelerates disease progression. This module covers the complete management framework: non-pharmacological measures, the four pillars of pharmacological therapy in HFrEF, device and surgical options, and the procedural skill of intramuscular injection.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 253 — Heart Failure: Treatment (textbook)
- API Textbook of Medicine, 10th ed., Ch. 8 — Cardiac Failure: Management (textbook)
- ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure, 2021 (guideline)
- ACC/AHA/HFSA Heart Failure Guideline 2022 Update (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Rajan, a 58-year-old schoolteacher with hypertension and type 2 diabetes, is discharged from hospital after his first admission for decompensated heart failure. His echocardiogram shows an LVEF of 34% — HFrEF. His physician starts him on four medications: ramipril 2.5 mg, carvedilol 3.125 mg twice daily, spironolactone 25 mg, and furosemide 40 mg. His wife asks why he needs so many tablets when he has only one problem. The physician explains: each drug addresses a different pathological mechanism — the furosemide removes the excess fluid that caused his breathlessness; the ramipril blocks the renin-angiotensin system that was remodelling and shrinking his ventricle; the carvedilol blocks the sympathetic overdrive that was making his heart beat too fast and too hard; and the spironolactone blocks the aldosterone that was causing fibrosis and potassium loss. She also asks about his diet — he eats quite salty food. The physician explains that sodium restriction is as important as any tablet. Three months later, Rajan's LVEF has improved to 42% and his NYHA class has dropped from III to II. This is the power of guideline-directed medical therapy in HFrEF — it reverses remodelling, not just relieves symptoms.
WHY THIS MATTERS
Heart failure management is one of the highest-yield topics in internal medicine finals — the NMC competencies IM1.21 through IM1.27 collectively cover the full management arc from lifestyle to drugs to surgery to intramuscular injection technique. In clinical practice, the ability to draft a correct management plan for a patient with HFrEF (LVEF ≤40%) versus HFpEF (LVEF ≥50%) versus acute decompensated heart failure represents a core skill required of every junior doctor managing inpatients on a medical ward. Understanding not just which drug to prescribe but why — the underlying pharmacological rationale — prevents prescription errors and allows you to anticipate and manage adverse effects and drug interactions.
RECALL
Recall the neurohormonal model of heart failure: reduced cardiac output activates three maladaptive pathways: (1) the renin-angiotensin-aldosterone system (RAAS) — angiotensin II causes vasoconstriction and promotes aldosterone release, causing sodium and water retention; (2) the sympathetic nervous system (SNS) — catecholamines cause tachycardia, vasoconstriction, and direct cardiotoxicity; and (3) arginine vasopressin (ADH) — promotes water retention. Together, these lead to volume overload (causing congestion), increased afterload (causing further LV dysfunction), and adverse cardiac remodelling (LV dilation and fibrosis). Recall also the HF classification by LVEF: HFrEF (≤40%), HFmrEF (41–49%), HFpEF (≥50%). The pharmacological therapies with mortality benefit are predominantly validated in HFrEF. Also recall NYHA classification: Class I (no symptoms with ordinary activity), Class II (mild symptoms with ordinary activity), Class III (symptoms with less-than-ordinary activity), Class IV (symptoms at rest).
Non-Pharmacological Management: Lifestyle and Self-Care
Non-pharmacological management is the foundation upon which all pharmacological and device therapies rest. In clinical practice, patients who do not implement lifestyle modifications have poorer outcomes regardless of medication adherence — sodium intake can negate the diuretic effect, excessive fluid intake can precipitate decompensation, and physical inactivity accelerates deconditioning. Communicating these measures clearly and practically is a core clinical skill at the NMC SH level.
Provided image
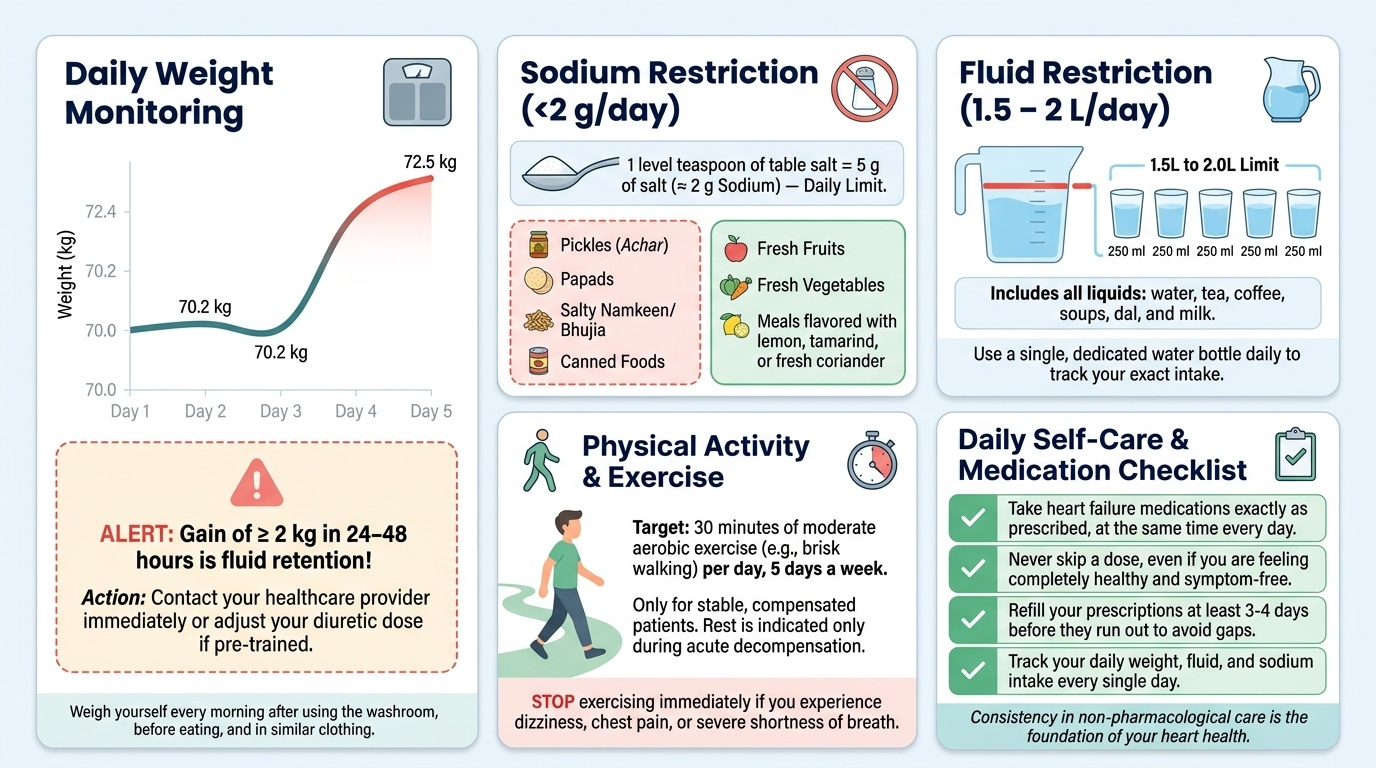
Sodium restriction is the single most important dietary modification in heart failure. Dietary sodium drives fluid retention via the aldosterone pathway, and a high-sodium diet works directly against the diuretic therapy that relieves congestion. The recommended daily sodium intake is <2 g/day (equivalent to <5 g of table salt per day) for patients with symptomatic heart failure (NYHA II–IV). This requires counselling patients to avoid added table salt, processed foods, pickles, papads, canned foods, and salty snacks — all common in the Indian diet. In patients with refractory oedema on high-dose diuretics, sodium restriction may be as effective as increasing the diuretic dose and avoids the nephrotoxicity of escalating loop diuretics.
Fluid restriction is recommended in patients with hyponatraemia (serum sodium <130 mmol/L) or severe decompensated heart failure where dilutional hyponatraemia complicates management. The target is typically <1.5–2 L/day total fluid intake including all beverages. Routine fluid restriction in compensated heart failure without hyponatraemia is not universally recommended and must be individualised. Patients should be taught daily weight monitoring — a gain of >2 kg in 24–48 hours almost always represents fluid retention and should trigger a self-directed increase in diuretic dose (if patient has been educated on flexible dosing) or an urgent clinical review.
Physical activity and rehabilitation: Bed rest is indicated only in acute decompensated heart failure. In stable, compensated heart failure, regular aerobic exercise is strongly recommended and is associated with improved functional capacity (higher peak VO₂), reduced hospitalisation rates, and improved quality of life. The HF-ACTION trial (2009) demonstrated that a structured aerobic exercise programme in NYHA II–III HFrEF patients reduced hospitalisation and cardiovascular mortality. The recommended programme is moderate-intensity aerobic exercise (e.g., walking, cycling) for 30 minutes, 5 days per week, with gradual progression. High-intensity exercise or competitive sport should be avoided.
Other non-pharmacological measures:
- Smoking cessation: Nicotine is a direct cardiac stimulant and contributes to coronary artery disease progression; cessation is mandatory.
- Alcohol limitation or abstinence: Alcohol is a direct cardiac myotoxin (alcoholic cardiomyopathy). In alcoholic CM, total abstinence can lead to significant LVEF recovery. Even in non-alcoholic HF, alcohol intake should be minimised (<10 g/day).
- Vaccination: Annual influenza vaccine and pneumococcal vaccine are recommended to prevent infections that can trigger acute decompensation.
- Medication adherence: Non-adherence to medications (particularly beta-blockers and diuretics) is a major cause of decompensation. Simple measures — pill boxes, written instructions, family involvement — improve adherence.
- Travel and altitude: Patients should be counselled that high altitude (>2500 m) and long-haul flights carry risks due to hypoxia and immobility (DVT/PE risk); air travel is generally safe in compensated NYHA I–II heart failure.
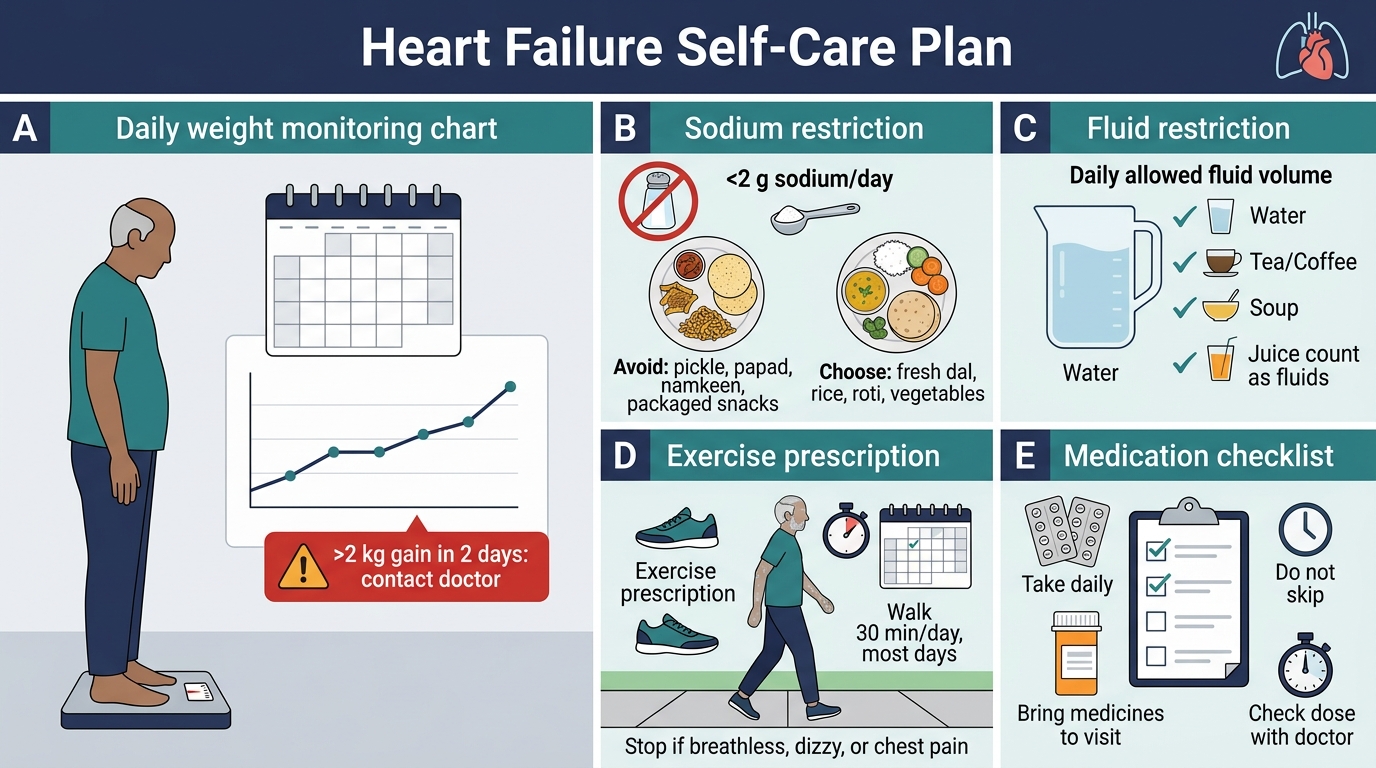
Heart Failure Self-Care Plan
Pharmacological Management: Four Pillars of HFrEF Therapy
The pharmacological management of HFrEF (LVEF ≤40%) is built on four evidence-based pillars, each of which targets a different aspect of the neurohormonal cascade driving disease progression. These four classes together reduce all-cause mortality, reduce hospitalisation, and reverse ventricular remodelling. Every patient with HFrEF who is haemodynamically stable should receive all four unless a specific contraindication exists — this is what current guidelines call guideline-directed medical therapy (GDMT) for HFrEF.
Pillar 1 — ACE Inhibitors (ACEi) / Angiotensin Receptor Blockers (ARBs) / ARNI:
ACE inhibitors block the conversion of angiotensin I to angiotensin II, reducing vasoconstriction, lowering preload and afterload, reducing aldosterone-mediated sodium retention, and attenuating cardiac fibrosis and remodelling. They reduce all-cause mortality in HFrEF by approximately 16–23% and hospitalisation by ~26% (CONSENSUS, SOLVD trials). Starting dose: enalapril 2.5 mg BD or ramipril 2.5 mg OD, uptitrated over weeks to target dose (enalapril 10–20 mg BD; ramipril 10 mg OD). Key contraindications: bilateral renal artery stenosis, pregnancy, history of angioedema with ACEi. Adverse effects: dry cough (bradykinin accumulation, 10–15% of Indian patients — switch to ARB if intolerable), hyperkalaemia, worsening renal function (monitor at 1–2 weeks after initiation and each dose increase), first-dose hypotension. ARBs (valsartan, losartan, candesartan) are used when ACEi is not tolerated; they block the angiotensin II receptor directly. ARNI (sacubitril/valsartan, brand Entresto) combines ARB + neprilysin inhibitor; neprilysin inhibition raises natriuretic peptide levels, enhancing natriuresis, vasodilation, and anti-fibrotic effects. The PARADIGM-HF trial showed ARNI reduced cardiovascular death and hospitalisation by 20% vs enalapril in HFrEF (NYHA II–III, LVEF ≤40%). ARNI is now preferred over ACEi/ARB alone in tolerant patients. Contraindication: do NOT combine with ACEi (angioedema risk); a 36-hour washout period is required when switching from ACEi to ARNI.
Pillar 2 — Beta-Blockers:
Beta-blockers reduce sympathetic cardiac stimulation — slowing heart rate (allowing more complete diastolic filling), reducing afterload, and preventing the direct catecholamine toxicity that promotes cardiomyocyte death and adverse remodelling. Only three beta-blockers have proven mortality benefit in HFrEF: carvedilol (non-selective beta-1/2/alpha-1 blocker), metoprolol succinate (selective beta-1, extended release), and bisoprolol (selective beta-1). Starting doses: carvedilol 3.125 mg BD; bisoprolol 1.25 mg OD; metoprolol succinate 12.5–25 mg OD. Target doses: carvedilol 25–50 mg BD; bisoprolol 10 mg OD; metoprolol succinate 200 mg OD. Uptitration should be slow (double dose every 2 weeks as tolerated). Contraindications: severe bradycardia, high-degree AV block, decompensated heart failure requiring IV positive inotropes, severe reactive airway disease. A critical clinical point: beta-blockers must NOT be started during acute decompensation (they can worsen haemodynamics) but must NOT be stopped in a patient who develops acute decompensation while already on a beta-blocker (abrupt cessation causes rebound tachycardia and worsening outcome).
Pillar 3 — Mineralocorticoid Receptor Antagonists (MRA):
Spironolactone and eplerenone block aldosterone at the mineralocorticoid receptor in the kidney and myocardium, reducing sodium retention and fibrosis. Spironolactone reduced all-cause mortality by 30% in severe HFrEF (LVEF ≤35%, NYHA III–IV) in the RALES trial. Eplerenone reduced mortality in post-MI HF (EPHESUS) and milder HFrEF (EMPHASIS-HF). Dose: spironolactone 25–50 mg OD. Contraindications: eGFR <30 mL/min/1.73 m², serum potassium >5.0 mmol/L. Risk: hyperkalaemia (especially when combined with ACEi/ARB — monitor K⁺ and renal function at 1 week and monthly for 3 months). Spironolactone also has anti-androgenic effects (gynaecomastia in men — switch to eplerenone if intolerable).
Pillar 4 — SGLT2 Inhibitors:
Empagliflozin (EMPEROR-Reduced) and dapagliflozin (DAPA-HF) are sodium-glucose cotransporter-2 inhibitors originally developed as glucose-lowering agents for diabetes. They reduce cardiovascular death and HF hospitalisation in HFrEF by approximately 25% regardless of diabetic status. Their mechanisms in HF are osmotic diuresis/natriuresis, reduction in cardiac preload and afterload, possible direct myocardial metabolic effects (shift to ketone metabolism), and anti-inflammatory and anti-fibrotic effects. Dose: empagliflozin 10 mg OD; dapagliflozin 10 mg OD. Contraindication: eGFR <20 mL/min. Adverse effects: genital mycotic infections, urinary tract infections, rare euglycaemic diabetic ketoacidosis (hold before major surgery).
Diuretics — symptomatic relief, not prognosis:
Loop diuretics (furosemide, torsemide) are the mainstay of symptom relief in heart failure — they rapidly relieve fluid congestion and dyspnoea. However, they have NOT been shown to improve survival in heart failure (unlike the four pillars above). Furosemide 20–80 mg OD/BD is the standard starting point, uptitrated based on volume status. Key points: oral bioavailability is variable; in oedematous bowel, IV furosemide (initial dose 20–40 mg IV) achieves more reliable response. Monitor urea, creatinine, and potassium — loop diuretics cause hypokalaemia and hypomagnesaemia, increasing arrhythmia risk. The goal of diuresis is euvolaemia, not maximum diuresis — over-diuresis causes renal impairment and activates the neurohormonal axis.
Cardiac glycosides — digoxin:
Digoxin inhibits Na⁺/K⁺-ATPase, increasing intracellular calcium and contractility (positive inotropy), and reduces sinus rate and AV conduction (negative chronotropy/dromotropy via enhanced vagal tone). In HFrEF, the DIG trial showed digoxin reduces hospitalisation but does NOT reduce mortality. Its role is therefore adjunctive — improving symptoms and reducing hospitalisation in patients who remain symptomatic despite GDMT, and rate control in AF with HFrEF. Dosing: digoxin 0.125–0.25 mg OD (lower doses in elderly and renal impairment). Narrow therapeutic index — serum level 0.5–0.9 ng/mL (aim for the lower range in HF; higher levels associated with increased mortality). Toxicity: nausea, vomiting, visual disturbances (yellow-green halos), arrhythmias (PAT with block, bidirectional VT, AF with regularisation). Hypokalaemia potentiates digoxin toxicity — monitor K⁺ carefully when using digoxin with loop diuretics.
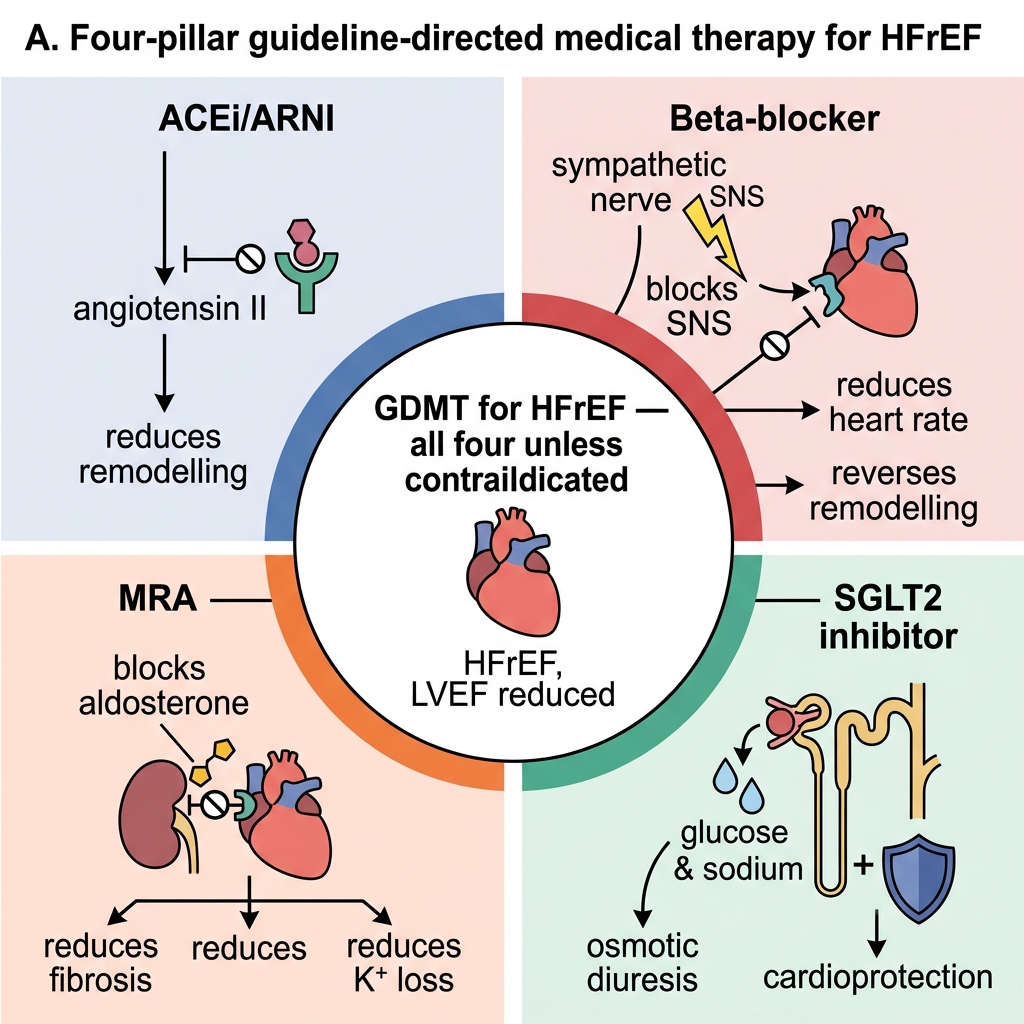
Four Pillars of GDMT for HFrEF
SELF-CHECK
A 55-year-old man with HFrEF (LVEF 32%) is on furosemide 40 mg OD and ramipril 5 mg OD. He is euvolaemic and haemodynamically stable (BP 118/74, HR 88 bpm sinus rhythm). His eGFR is 52 mL/min and potassium is 4.2 mmol/L. According to GDMT for HFrEF, which TWO drug classes should be added at this clinic visit?
A. Digoxin and amlodipine
B. Bisoprolol and spironolactone
C. Hydralazine and isosorbide dinitrate
D. Ivabradine and eplerenone
Reveal Answer
Answer: B. Bisoprolol and spironolactone
This patient is stable, euvolaemic, on ACEi (ramipril) and diuretic but missing two of the four GDMT pillars: a beta-blocker and an MRA. Bisoprolol (or carvedilol or metoprolol succinate) is indicated as the beta-blocker pillar; spironolactone (or eplerenone) is the MRA pillar — both have proven mortality benefit in HFrEF. eGFR 52 and K+ 4.2 do not contraindicate spironolactone. Digoxin is adjunctive (symptom/hospitalisation reduction only, no mortality benefit). Amlodipine has no mortality benefit in HFrEF and dihydropyridine CCBs are generally avoided. Hydralazine-isosorbide dinitrate is an alternative to ACEi/ARB (e.g., in ACEi/ARB-intolerant Black patients or in patients with eGFR <20) — not an additive fourth agent. Ivabradine is for rate reduction when HR remains ≥70 bpm despite max beta-blocker.
Surgical and Procedural Interventions
While pharmacological therapy is the cornerstone of heart failure management, a significant proportion of patients have an underlying structural or coronary aetiology that requires surgical or catheter-based correction. Identifying which patients need intervention — and what type — requires integration of the clinical picture, echocardiographic findings, and angiographic data. The key principle is that surgical intervention should be considered before irreversible LV dysfunction develops, because once the ventricle has undergone severe fibrotic remodelling, correcting the structural cause may not restore function.
Coronary revascularisation (CABG or PCI):
In patients with HFrEF where the aetiology is ischaemic cardiomyopathy — reduced LVEF caused by CAD, prior MI, or hibernating myocardium — revascularisation can improve ventricular function and symptoms. The STICH trial (Surgical Treatment for Ischaemic Heart Failure) showed that CABG + GDMT reduced cardiovascular mortality compared to GDMT alone over 10 years in patients with LVEF ≤35% and significant CAD. Indications for revascularisation in HFrEF with CAD: (1) reversible perfusion defects on nuclear MPI (viable, hibernating myocardium that can recover after revascularisation), (2) significant CAD (multivessel or left main) on angiography, (3) ongoing angina despite optimal medical therapy. PCI is appropriate for single-vessel or limited multivessel disease; CABG is preferred for multivessel CAD (particularly with left main or proximal LAD disease) or in the setting of significant valve disease requiring concurrent repair.
Valvuloplasty and valvotomy:
Percutaneous mitral balloon valvotomy (PMBV) is the treatment of choice for rheumatic mitral stenosis with favourable anatomy (Wilkins score ≤8, no significant MR, no LA thrombus). It is performed by introducing an Inoue or double-balloon catheter through a transseptal puncture and inflating the balloon across the mitral valve to split the fused commissures. Success is defined as MVA post-procedure ≥1.5 cm² or doubling of MVA with MR ≤2+. Aortic balloon valvuloplasty (for aortic stenosis) provides only temporary relief (restenosis within months) and is reserved as a bridge to TAVR/SAVR in haemodynamically unstable patients.
Surgical valve repair and replacement:
- Mitral valve repair (for degenerative MR — posterior leaflet prolapse, chordal rupture): ring annuloplasty + leaflet repair; preferred over replacement to preserve LV function; feasible in 95% of posterior prolapse cases at expert centres.
- Mitral valve replacement (MVR): for rheumatic MS with unfavourable anatomy, severe rheumatic MR, or when repair is not feasible. Bioprosthetic valves (tissue) have limited durability (~10–15 years) but do not require anticoagulation beyond 3 months. Mechanical valves are durable but require lifelong anticoagulation with warfarin — target INR 2–3 for aortic mechanical valve, 2.5–3.5 for mitral mechanical valve (mitral position has higher thrombotic risk).
- Aortic valve replacement (SAVR or TAVR): For severe symptomatic AS (Stage D). SAVR preferred for patients <65 years with low surgical risk; TAVR for high-surgical-risk or intermediate-risk patients ≥65 years.
Cardiac resynchronisation therapy (CRT):
Indicated for LVEF ≤35% + NYHA II–III on GDMT + LBBB with QRS ≥150 ms. Biventricular pacing restores the normal interventricular synchrony that LBBB disrupts. CRT improves symptoms, increases LVEF by ~6–8% absolute, reduces hospitalisation, and reduces mortality (CARE-HF, COMPANION trials). CRT-D (combined with ICD) is preferred in patients with LVEF ≤35% who are also candidates for primary prevention ICD.
Implantable cardioverter-defibrillator (ICD):
For primary prevention of sudden cardiac death in LVEF ≤35% + NYHA II–III + at least 3 months of GDMT. Reduces all-cause mortality by approximately 23% (SCD-HeFT trial). Not indicated if life expectancy is <1 year or if the patient has refractory NYHA IV symptoms (transplant is then the priority).
Left ventricular assist device (LVAD):
A mechanical pump surgically implanted to augment or replace LV pump function. Used as: (1) bridge to transplantation (BTT) — to keep the patient alive and clinically stable while awaiting a donor heart; (2) destination therapy (DT) — permanent implantation in patients who are not transplant candidates (REMATCH trial). Complications: device thrombosis, stroke, infection of the drive-line, right heart failure.
Cardiac transplantation:
The definitive treatment for end-stage heart failure refractory to all other therapies. Indications: NYHA IV symptoms, peak VO₂ <12–14 mL/kg/min on CPET, refractory cardiogenic shock requiring escalating inotropes/IABP/LVAD, refractory life-threatening arrhythmias despite ICD. Contraindications (absolute): irreversible pulmonary hypertension (PVR >6 Wood units unresponsive to vasodilators), active malignancy, active systemic infection, significant irreversible non-cardiac organ failure, substance abuse. Five-year survival post-transplantation is approximately 70%. The major limitation is the shortage of donor hearts — in India, organ donation rates remain very low despite the Transplantation of Human Organs Act 1994 amendments.
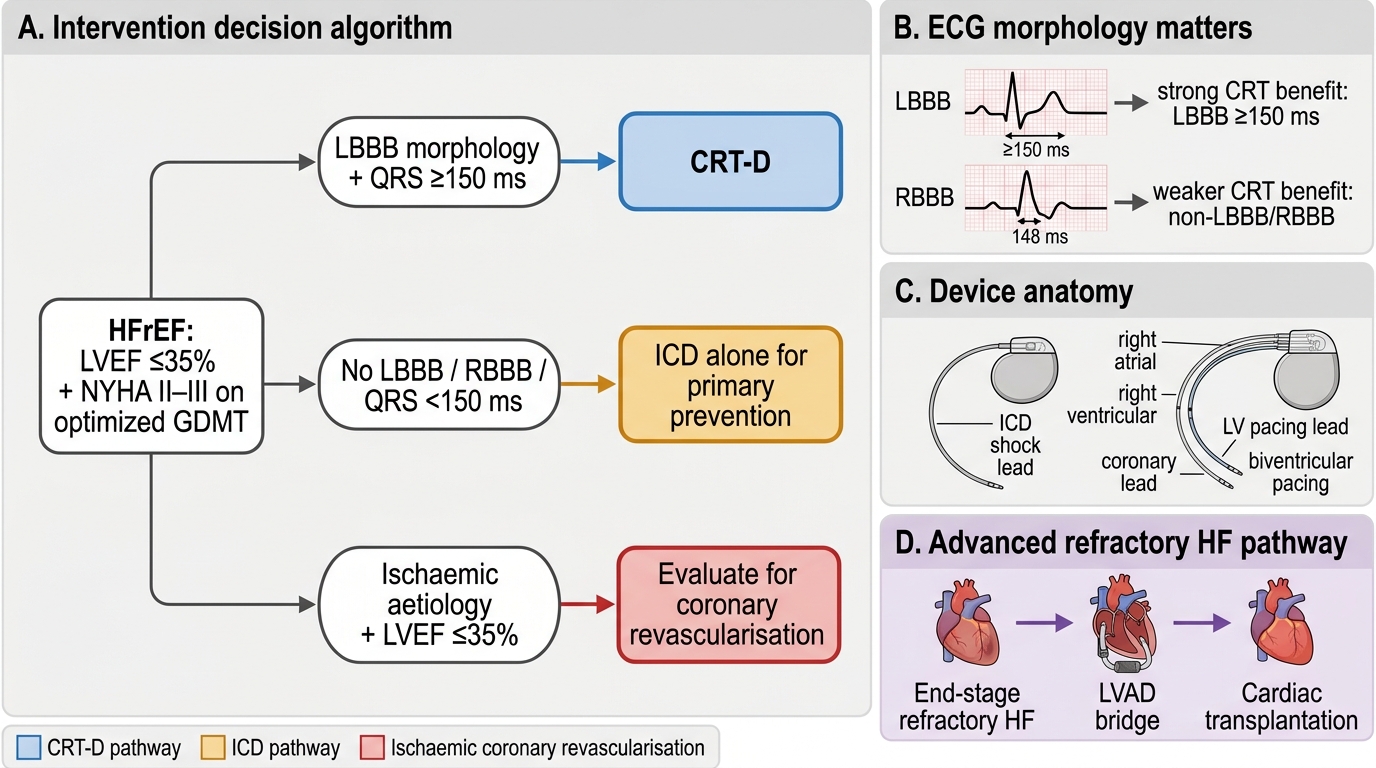
Device and Surgical Intervention Pathway in HFrEF
SELF-CHECK
A 62-year-old man with ischaemic cardiomyopathy and LVEF 28% has been on optimised GDMT (ramipril, bisoprolol, eplerenone, dapagliflozin, furosemide) for 6 months. His ECG shows sinus rhythm, QRS 148 ms with RBBB morphology. His NYHA class remains III. He has no significant CAD amenable to revascularisation. Which of the following is the MOST appropriate next intervention?
A. Cardiac resynchronisation therapy (CRT) — QRS ≥150 ms with RBBB qualifies for CRT
B. Implantable cardioverter-defibrillator (ICD) alone for primary prevention of sudden cardiac death
C. Cardiac transplantation listing as first-line device therapy
D. Digoxin add-on for additional rate control
Reveal Answer
Answer: B. Implantable cardioverter-defibrillator (ICD) alone for primary prevention of sudden cardiac death
CRT has Class I indication for LBBB morphology with QRS ≥150 ms. For RBBB or non-LBBB conduction delay, the evidence for CRT is weaker (Class IIb indication) — RBBB does not produce the same degree of interventricular mechanical dyssynchrony as LBBB, and the landmark CRT trials showed lesser benefit in non-LBBB patients. This patient with QRS 148 ms RBBB does not meet the primary CRT indication. The correct intervention is ICD alone (primary prevention of SCD) — LVEF ≤35%, NYHA II–III, on optimal GDMT for >3 months. Transplantation is not first-line device therapy; it is reserved for end-stage refractory disease after devices and GDMT have been optimised. Digoxin provides only symptom/hospitalisation reduction in sinus rhythm and is not an intervention for this device-eligibility decision.