Page 16 of 25
IM1.{21-24,27} | Heart Failure Management and Procedures — SDL Guide (Part 2)
Acute Decompensated Heart Failure: Emergency Management
Acute decompensated heart failure (ADHF) is the most common cardiac cause of emergency hospitalisation and represents a clinical emergency requiring rapid assessment, simultaneous resuscitation and diagnostics, and institution of specific therapies within the first hour. The management of ADHF differs fundamentally from the management of chronic, stable HF — the therapeutic priorities are decongestion (relieving the acute fluid overload), haemodynamic stabilisation (maintaining adequate organ perfusion), and identification and treatment of the precipitating cause. Understanding the emergency management framework is essential for the IM final-year student, who will encounter ADHF on every acute medical intake.
Provided image
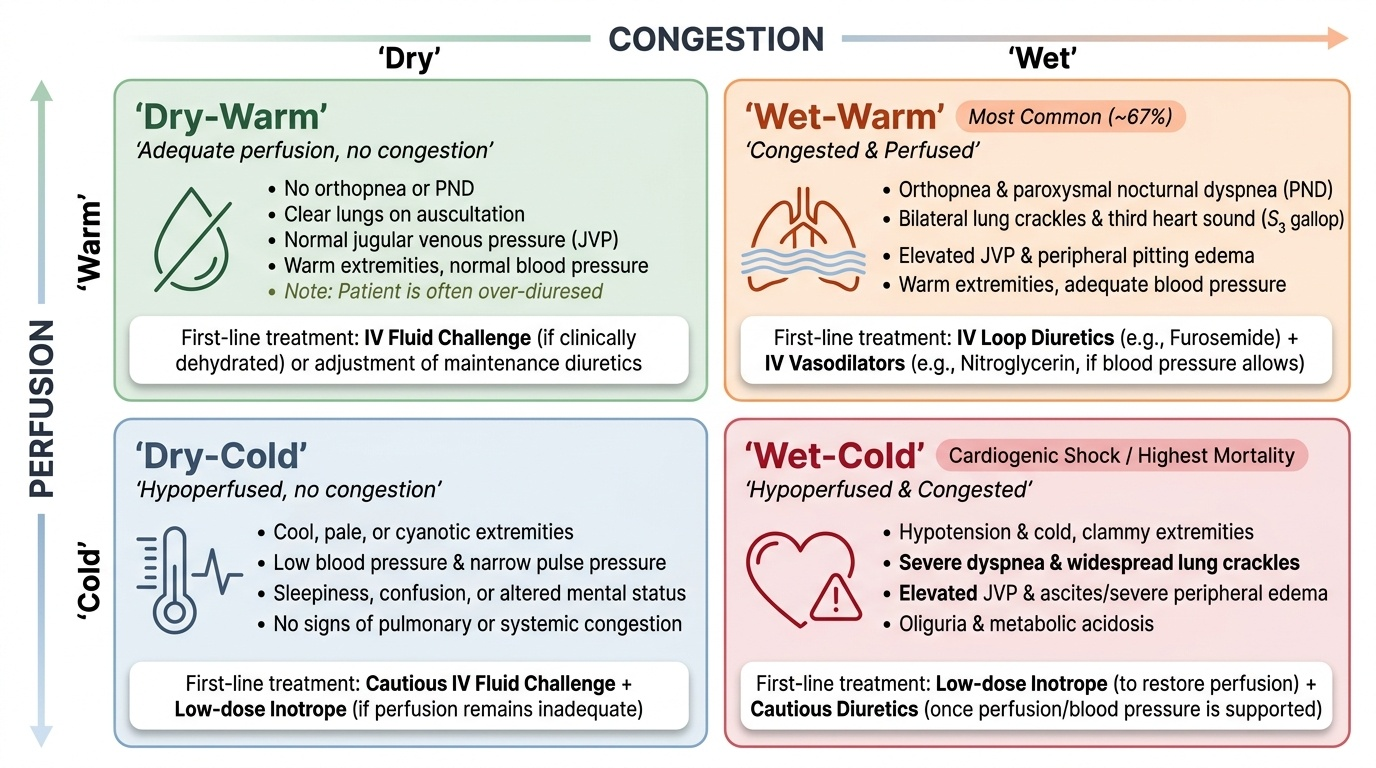
Immediate assessment and monitoring: The patient is assessed using the clinical profile — two axes: (1) congested ('wet') vs non-congested ('dry') based on symptoms (orthopnoea, PND, ankle oedema, elevated JVP, S3, crackles), and (2) low perfusion ('cold') vs adequate perfusion ('warm') based on BP, pulse pressure, cool peripheries, and altered consciousness. The four clinical profiles are: Wet-Warm (congested, good perfusion — most common ~67%); Dry-Warm (not congested, adequate perfusion — usually dehydrated or over-diuresed); Wet-Cold (congested and hypoperfused — cardiogenic shock, highest mortality); Dry-Cold (not congested, low perfusion — low-output failure without congestion). This bedside profiling determines the immediate treatment decision.
Immediate interventions:
- Positioning: Sit the patient upright (reduces venous return, lowers preload, improves respiratory mechanics).
- Supplemental oxygen: Titrate to SpO₂ ≥94%. Avoid routine high-flow oxygen in non-hypoxic patients (hyperoxia causes vasoconstriction and may be harmful).
- Non-invasive positive pressure ventilation (NIV): CPAP or BiPAP is the most effective non-pharmacological intervention for acute pulmonary oedema — it reduces work of breathing, improves oxygenation, and reduces the need for intubation. Start CPAP 5–7.5 cmH₂O and uptitrate.
- IV loop diuretic: Furosemide 40–80 mg IV (or double the patient's usual oral dose) as the cornerstone of ADHF decongestion. Urine output response guides further doses.
- Vasodilators: In Wet-Warm patients (adequate BP): IV nitroglycerin (glyceryl trinitrate) infusion — reduces preload (primarily) and afterload, rapidly relieves dyspnoea. Contraindicated in hypotension (SBP <90 mmHg) and in patients taking PDE5 inhibitors (sildenafil — synergistic hypotension).
- Positive inotropes: In Wet-Cold patients (cardiogenic shock with SBP <90): dobutamine (beta-1 agonist, increases contractility) or dopamine (low dose = renal vasodilation; high dose = vasopressor). These are short-term stabilising agents, not chronic therapies. They have not been shown to improve survival and may be harmful with prolonged use.
- Vasopressors: Norepinephrine for profound cardiogenic shock with very low BP, to restore perfusion pressure while other interventions take effect.
Precipitating causes must be identified and treated in every ADHF admission. Common precipitants: acute coronary syndrome (ECG, troponin), uncontrolled hypertension, new AF with rapid ventricular rate, medication non-adherence, dietary indiscretion (excess sodium), infection (pneumonia, IE, sepsis), anaemia, thyrotoxicosis, NSAID use (worsen both HF and renal function), and new valvular regurgitation.
Transition to oral therapy: As the patient improves (diuresis adequate, dyspnoea resolving, SpO₂ >94% on room air, weight decreasing toward target), IV therapy is transitioned to oral. GDMT should not be withheld during admission — beta-blockers should be continued or cautiously dose-reduced, not stopped; ACEi/ARB should be restarted at lowest dose as BP allows. Diuretics are rationalised to the lowest effective oral dose that maintains euvolaemia.
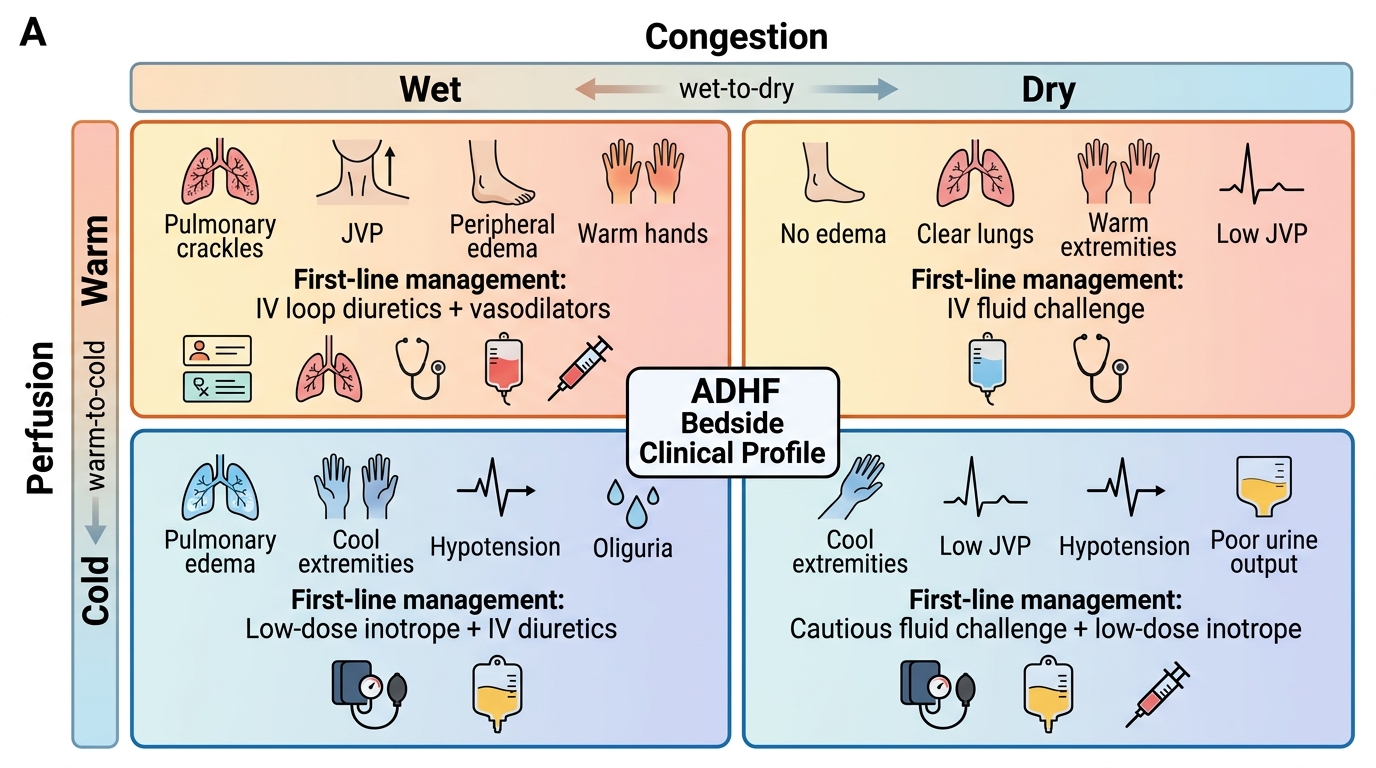
ADHF Clinical Profiling Matrix
Intramuscular Injection: Technique and Patient Communication
The intramuscular (IM) injection is a core procedural skill for every MBBS graduate and is explicitly listed as a competency in the IM curriculum (IM1.27: SH level — perform with hands-on). In the context of heart failure management, IM injections are relevant for the administration of furosemide (when oral absorption is unreliable in oedematous bowel), morphine (in acute pulmonary oedema — now used more cautiously given evidence of harm), anticoagulants (low-molecular-weight heparin), and various other medications in the inpatient setting. The procedure must be performed with precision, aseptic technique, and clear patient communication.
Patient communication before IM injection:
Before performing any procedure, explain to the patient in clear, simple language: what the injection is for, what they will feel (a sharp sting followed by aching), approximately how long it will take, whether they need to do anything (remain still), and what to report afterwards (increasing pain, numbness, swelling). Obtain verbal consent. Confirm patient identity against the drug chart (name, registration number, date of birth). Check the drug prescription for: drug name, dose, route, time, prescriber signature. Check the drug itself: expiry date, integrity of the vial, correct concentration.
Sites for intramuscular injection:
- Ventrogluteal site (preferred): Over the gluteus medius and minimus, accessed by placing the heel of the hand on the greater trochanter, index finger pointing to the ASIS (anterior superior iliac spine), middle finger pointing posteriorly along the iliac crest — the injection is given in the V-space between the index and middle fingers. This site has the highest muscle mass, the fewest blood vessels and nerves, and the lowest complication rate — it is the recommended first-choice site in adults.
- Vastus lateralis (anterolateral thigh): The middle third of the anterolateral thigh, one handbreadth below the greater trochanter and one handbreadth above the knee. Preferred in infants and toddlers, and acceptable in adults.
- Dorsogluteal site (upper outer quadrant of buttock): Historically the most commonly used site, but now DISCOURAGED because of proximity to the sciatic nerve (running through the lower inner quadrant) and superior gluteal vessels. If used, it must be the upper outer quadrant, confirmed with the 'safe zone' anatomical landmarks.
- Deltoid: Small muscle, limited volume (≤2 mL), suitable for vaccines and small-volume IM drugs. Over the deltoid muscle belly, 2–3 fingerbreadths below the acromion process.
Procedure steps:
1. Perform hand hygiene (WHO five moments).
2. Gather equipment: correct syringe (usually 2–5 mL) and needle (21–23 gauge, 38–50 mm for adults), alcohol swab, gloves, cotton ball.
3. Prepare the drug: draw up the correct dose using aseptic technique; change the needle after drawing up (the drawing-up needle may have microscopic burrs from penetrating the rubber bung).
4. Position the patient appropriately (lateral or prone for gluteal sites; seated or supine for vastus lateralis or deltoid).
5. Identify the correct site using anatomical landmarks (see above).
6. Cleanse the site with an alcohol swab using a circular motion (centre outward), and allow to dry for 30 seconds (wet alcohol is irritant and can carry surface bacteria into the muscle).
7. Don non-sterile gloves.
8. Stretch the skin slightly taut (not bunched — that is for subcutaneous technique) — this reduces resistance to needle entry.
9. Insert the needle at 90 degrees to the skin in a single, dart-like movement to the hub.
10. Aspirate (pull the plunger back for 5–10 seconds) — if blood returns, withdraw the needle, apply pressure, and start again with a fresh needle and syringe (intravascular injection). Note: aspiration is still recommended in clinical practice despite some guideline variation for vaccines; for drug administration, aspiration should be performed.
11. Inject the drug at a steady, slow rate (approximately 1 mL per 10 seconds — avoids pain from rapid tissue distension).
12. Withdraw the needle rapidly at the same angle as insertion.
13. Apply gentle pressure with a dry cotton ball (do NOT massage — this disperses the drug unpredictably and can cause tissue irritation).
14. Activate the needle safety shield and dispose of the sharps in the sharps bin immediately.
15. Document the administration on the drug chart (site, time, signed).
Common errors and complications to avoid: Injection into scar tissue or haematoma (poor absorption), hitting the sciatic nerve in the dorsogluteal site (avoid this site), air embolism from inadequate aspiration technique, injection at 45 degrees instead of 90 (medication deposited in subcutaneous fat rather than muscle — poor absorption), failing to allow alcohol to dry before injection, and reusing a needle after drawing up.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
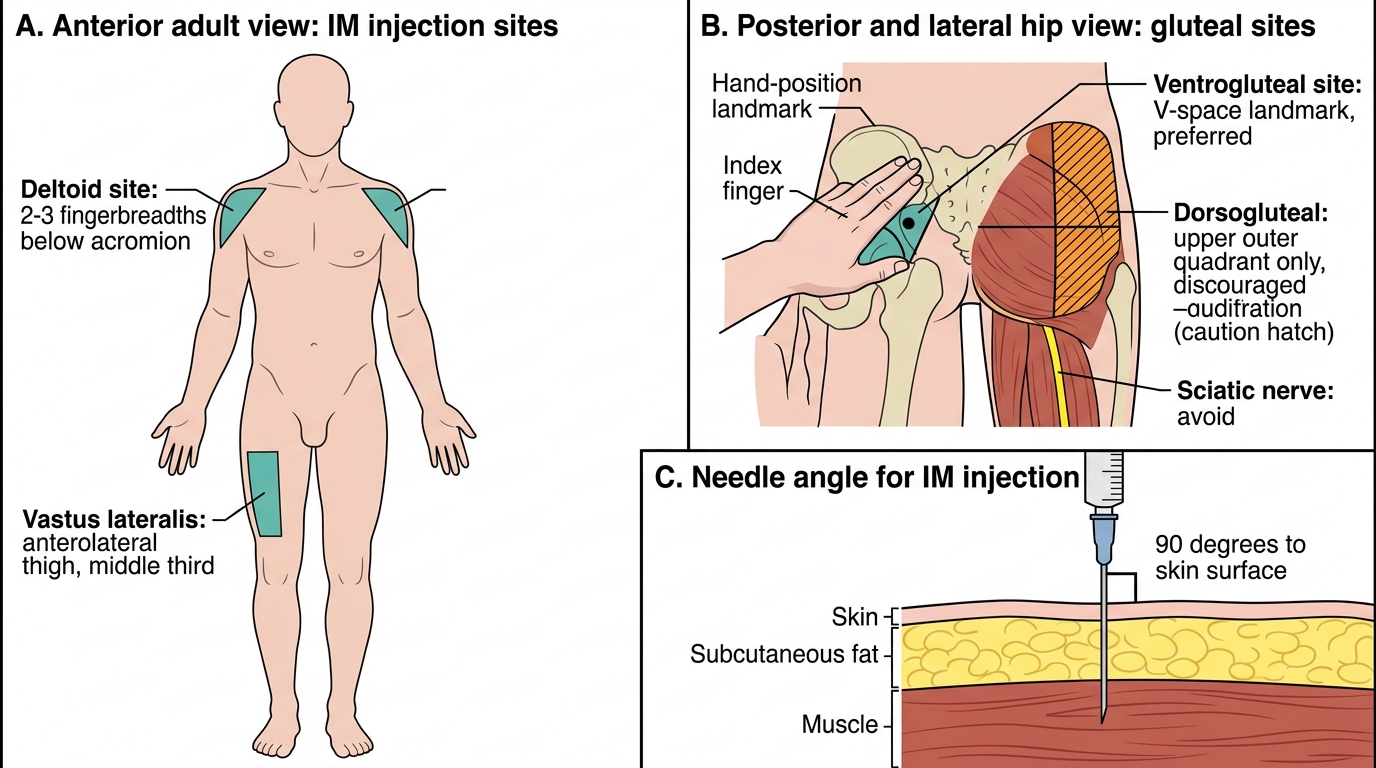
Intramuscular Injection Sites and Needle Angle
SELF-CHECK
During an IM injection into the ventrogluteal site, the nurse withdraws the plunger for 5 seconds and blood appears in the syringe. What is the CORRECT next action?
A. Inject the medication slowly despite the blood return — the drug will still be absorbed
B. Remove the needle immediately, apply pressure, and prepare a new syringe and needle for a fresh injection attempt
C. Flush the syringe with saline to clear the blood and then inject
D. Advance the needle further to ensure it is in muscle rather than a vessel
Reveal Answer
Answer: B. Remove the needle immediately, apply pressure, and prepare a new syringe and needle for a fresh injection attempt
Blood return on aspiration during IM injection indicates the needle tip is intravascular — injecting into a blood vessel can cause rapid systemic delivery of the drug (bypassing intended slow muscle absorption), potential overdose, or thrombophlebitis. The correct action is to withdraw the needle immediately without injecting, apply gentle pressure to the site, and then prepare a completely new syringe and needle (the existing one is contaminated by blood contact and may have a blunted tip) for a new injection at a different site. Never inject when blood has been aspirated.
Building the Management Plan: A Structured Approach
Constructing a comprehensive management plan for heart failure requires integration of the type of failure, the underlying aetiology, the severity (NYHA class), the presence of comorbidities, and the patient's specific situation. A structured management plan at the level expected in final MBBS (and the NMC IM1.24 competency at SH level) contains six domains: (1) diagnosis statement, (2) non-pharmacological measures, (3) pharmacological therapy stratified by EF category, (4) device/surgical therapy if indicated, (5) comorbidity management, and (6) follow-up plan.
Provided image
The following template illustrates a complete plan for a typical HFrEF patient — the most exam-tested scenario:
Case summary: A 60-year-old man with ischaemic cardiomyopathy, LVEF 30% (HFrEF), NYHA class II–III, eGFR 55, K⁺ 4.1 mmol/L, sinus rhythm HR 82 bpm, no AF, BP 130/82, no significant renal artery stenosis.
Domain 1 — Diagnosis: HFrEF (LVEF 30%), ischaemic aetiology (prior anterior MI), NYHA II–III, no current decompensation.
Domain 2 — Non-pharmacological: Dietary sodium restriction <2 g/day; daily weight monitoring (GP review if >2 kg gain in 2 days); moderate aerobic exercise 30 min × 5 days/week (after clinical stability confirmed); complete alcohol and smoking cessation; annual influenza + pneumococcal vaccination; medication adherence counselling.
Domain 3 — Pharmacological (GDMT — all four pillars):
- ACEi: Ramipril 2.5 mg OD → uptitrate to 10 mg OD over 4–8 weeks (or switch to sacubitril/valsartan if tolerated for additional mortality benefit).
- Beta-blocker: Bisoprolol 1.25 mg OD → uptitrate to 10 mg OD.
- MRA: Spironolactone 25 mg OD (check K⁺ and creatinine at 1 and 4 weeks).
- SGLT2i: Dapagliflozin 10 mg OD.
- Diuretic (symptom control): Furosemide 40 mg OD — titrate to maintain euvolaemia.
Domain 4 — Device/surgical therapy: ECG at next visit to assess QRS width. If QRS ≥150 ms with LBBB → refer for CRT-D assessment. Regardless of QRS: LVEF ≤35% after ≥3 months of GDMT → discuss ICD for primary SCD prevention. Coronary angiography if not previously done — assess for revascularisation target.
Domain 5 — Comorbidity management: Treat hypertension with GDMT overlap (ACEi + beta-blocker sufficient). Diabetes management with SGLT2i (dual benefit in HFrEF + T2DM). Anaemia assessment (Hb, iron studies — iron deficiency anaemia is common in HFrEF and IV iron ferric carboxymaltose improves symptoms and reduces hospitalisation even in non-anaemic iron-deficient patients).
Domain 6 — Follow-up: Review in 2 weeks for BP, renal function, electrolytes after GDMT initiation. Repeat echocardiogram at 6 months to assess LVEF response to GDMT (some patients recover to HFmrEF or HFpEF range — 'LVEF recovery' or 'HF with improved EF'). Structured HF nurse-led clinic review at 3 months.
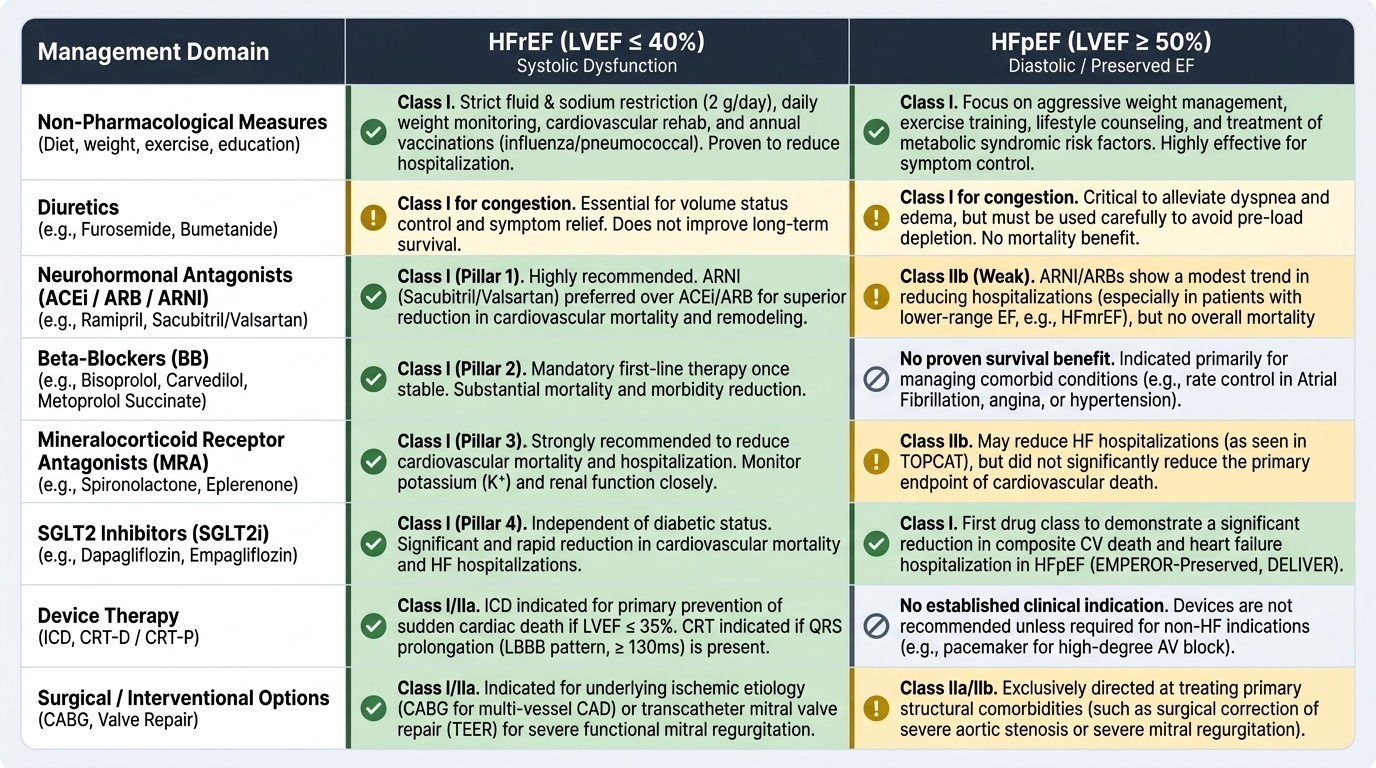
A note on HFpEF management: Unlike HFrEF, there is no established pharmacological treatment that reduces mortality in HFpEF. Management focuses on: (1) treating the underlying cause (tight BP control — target <130/80; manage AF; treat obesity and diabetes), (2) symptom relief with diuretics, and (3) SGLT2 inhibitors, which are now the first pharmacological agents with evidence of hospitalisation reduction in HFpEF (EMPEROR-Preserved and DELIVER trials). The absence of a proven mortality-reducing therapy in HFpEF is a key contrast with HFrEF that frequently appears in exam questions.
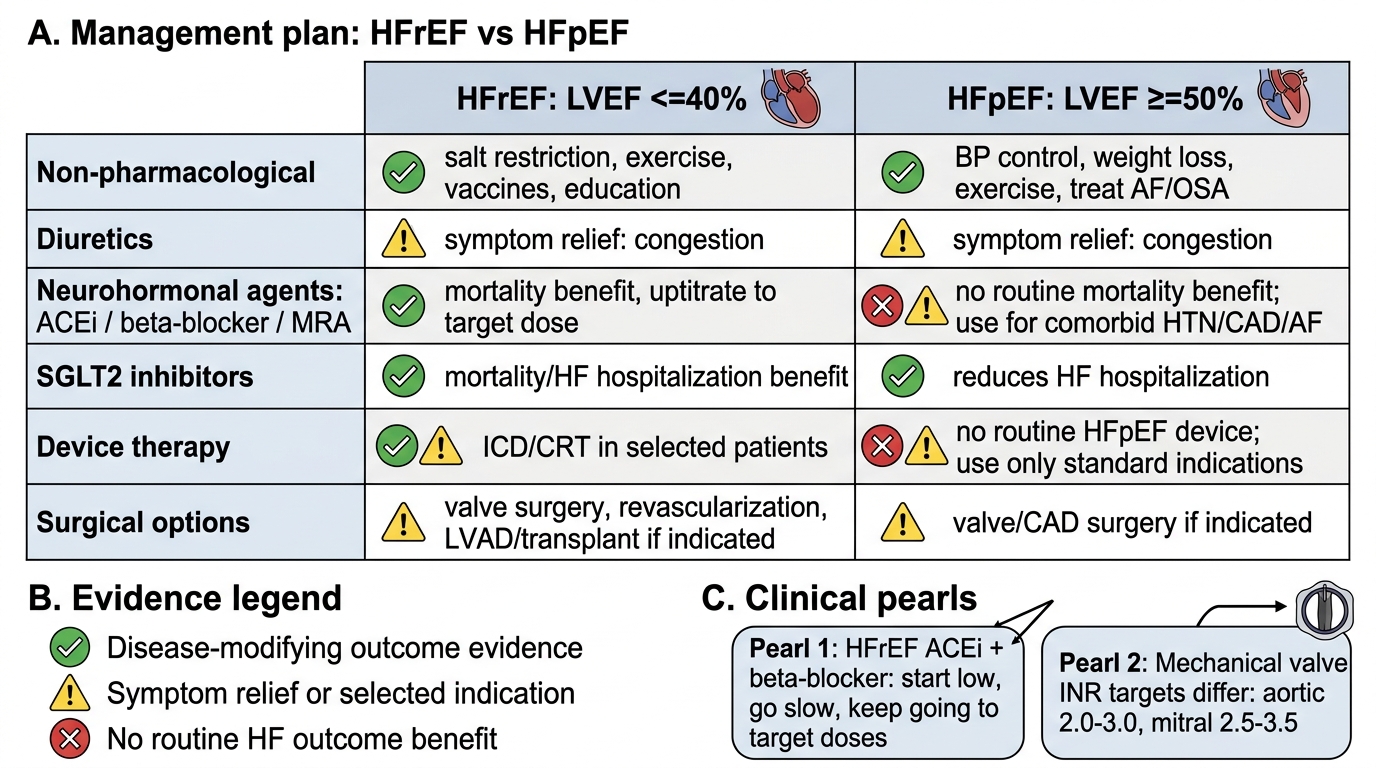
Management Summary: HFrEF vs HFpEF
CLINICAL PEARL
Two critical clinical pearls for heart failure management:
Pearl 1 — Uptitrate to target doses, not just minimum tolerated doses: The mortality benefit of ACE inhibitors and beta-blockers in HFrEF was demonstrated in trials using target doses (e.g., enalapril 10–20 mg BD; carvedilol 25–50 mg BD). Many clinicians initiate these drugs and never uptitrate beyond the starting dose, citing tolerability concerns. In the absence of specific contraindications (low BP, bradycardia, worsening renal function), patients should be uptitrated at each clinic visit. The principle is: start low, go slow — but keep going.
Pearl 2 — INR targets for mechanical valves are NOT interchangeable: The INR target for a mechanical aortic valve is 2.0–3.0, while for a mechanical mitral valve the target is 2.5–3.5 — a full 0.5 unit higher across the range. The mitral position carries higher thrombotic risk because of lower flow velocity and larger valve area. A common error is applying the aortic target to a mitral valve patient, which under-anticoagulates and risks valve thrombosis. Confirm the valve position whenever writing a warfarin prescription.