Page 4 of 23
IM11.7-10 | Diabetes Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit and document a structured diabetic history covering aetiology, risk factors, complications, and medications
- Perform a systematic examination covering skin, cardiovascular system, fundus, peripheral pulses, and detailed foot assessment
- Recognise the clinical features of diabetic emergencies (DKA, HHS, hypoglycaemia)
- Generate a prioritised differential diagnosis based on clinical features suggesting a specific aetiology
INSTRUCTIONS
The clinical evaluation of a diabetic patient is more than measuring glucose — it is a comprehensive systemic survey that detects existing complications, identifies cardiovascular risk factors, and guides individualised management. This skills-arc module develops the structured approach to history-taking and examination that every final-year student must master.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 403–408 — Diabetes Mellitus (textbook)
- API Textbook of Medicine, 10th ed., Ch. 51 — Diabetes Mellitus (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 21 — Clinical Examination in Diabetes (textbook)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are in the diabetes outpatient clinic when Mohan, a 56-year-old man, presents for his first visit having been 'told he has diabetes' by a local GP. He hands you a single sheet: FBG 148 mg/dL. He has no other records. In the 30 minutes you have, you must use history and examination alone to answer: What type of diabetes is this? How long has he likely had it? Are there already complications — in his eyes, kidneys, feet, heart? What medications might be causing or worsening it? What lifestyle and family factors are driving it? And crucially — is he at risk right now of a dangerous hypoglycaemic or hyperglycaemic event? A single glucose value tells you almost nothing. The clinical evaluation that follows it tells you everything.
WHY THIS MATTERS
The diabetic clinical evaluation is one of the highest-frequency clinical encounters in Indian medicine. In the MBBS final examination and the NMC IM competency set, you are expected to elicit a structured history (IM11.7), perform a targeted physical examination including fundoscopy and foot assessment (IM11.8), recognise emergency presentations (IM11.9), and formulate a differential diagnosis (IM11.10). In practice, a thorough initial evaluation of a newly diagnosed diabetic patient can detect advanced-stage complications that change management immediately — an unsuspected grade III retinopathy, a pulseless foot, or autonomic neuropathy masking cardiac ischaemia. Missing these on examination is a clinical and medicolegal hazard.
RECALL
Before proceeding, recall the core pathological targets of chronic hyperglycaemia. Microvascular complications affect small vessels in the retina (retinopathy), glomerulus (nephropathy), and peripheral nerves (neuropathy). Macrovascular complications affect large arteries — coronary arteries, carotid arteries, and peripheral limb arteries. The diabetic foot combines both: peripheral neuropathy removes the pain alarm, peripheral arterial disease removes the healing blood supply, and infection finds a metabolically impaired immune response. This anatomical map of complications directly structures the physical examination. Also recall the key differential distinguishing T1DM from T2DM: age at onset, body habitus, speed of onset, ketonuria, family history, and response to oral agents. These history points are the starting framework for IM11.10 (generating a differential).
Structured Diabetic History: Covering All Domains
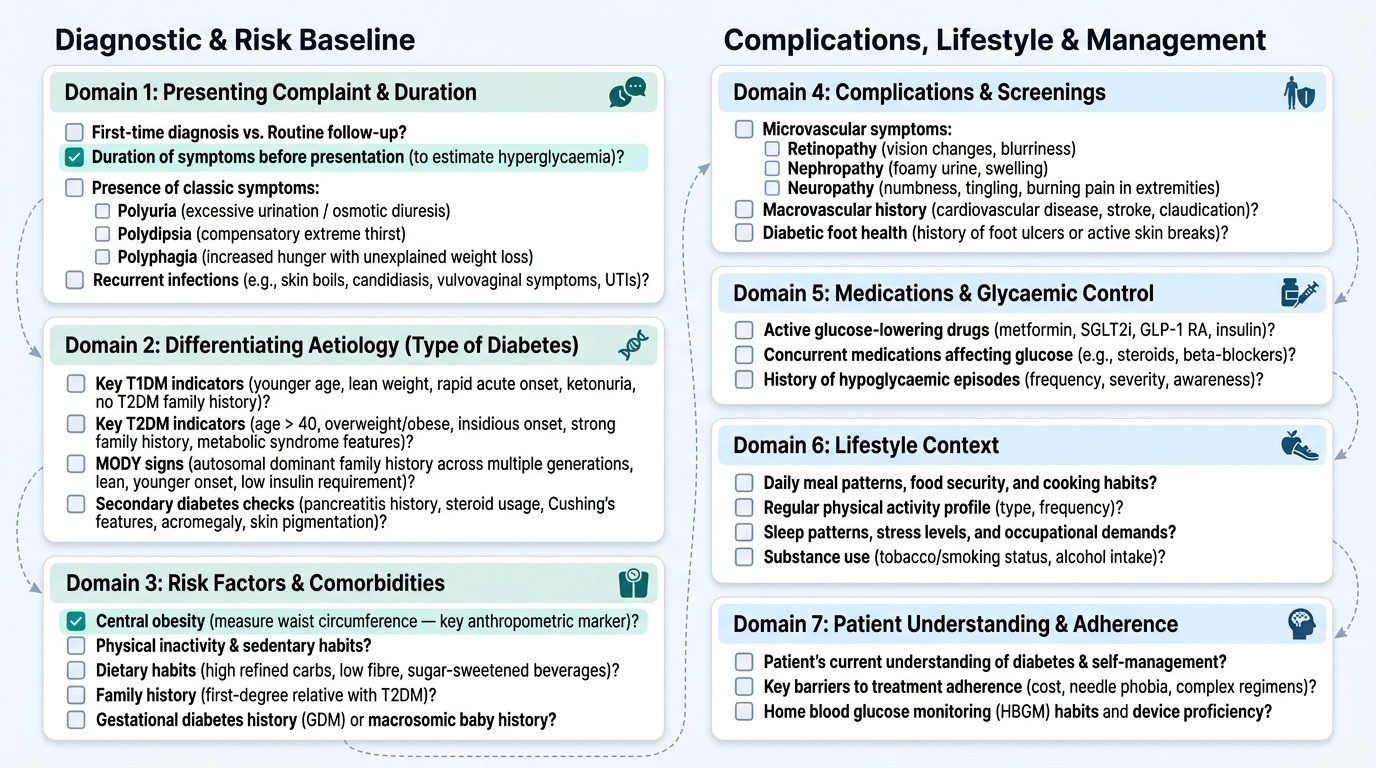
A comprehensive diabetic history is structured around seven domains that collectively answer: What type of diabetes? How long has the patient had it? What complications are present or suspected? What risk factors and comorbidities coexist? What medications are being used and are any relevant to glucose control? What is the lifestyle context? And what is the patient's understanding and adherence?
Provided image
Domain 1 — Presenting Complaint and Duration: Establish the precise nature of the presenting problem. Is this a first diagnosis or a routine review? If first diagnosis, the duration of symptoms before presentation helps estimate how long the patient may have had undetected hyperglycaemia. Classic symptoms of hyperglycaemia are polyuria (osmotic diuresis), polydipsia (compensatory thirst), polyphagia (despite which, weight loss occurs in insulin-deficient states), unexplained weight loss, recurrent skin infections (boils, candidiasis — particularly vulvovaginal candidiasis in women), and recurrent urinary tract infections.
Domain 2 — Differentiating the Aetiology (Type of Diabetes): Key discriminating features:
- T1DM: Younger age (<40, often childhood/adolescence), lean or normal weight, acute/subacute onset (days-weeks), ketonuria, absence of family history of T2DM in first-degree relatives, may require insulin from outset, positive autoantibodies (GAD65, IA-2) if tested
- T2DM: Age >40 (though increasingly younger in India), overweight/obese, insidious onset (often asymptomatic until detected on screening), strong family history of T2DM, associated metabolic syndrome features
- MODY: Strong autosomal dominant family history (multiple generations), lean phenotype, often young, minimal glycaemia, does not require insulin initially
- Secondary diabetes: Ask specifically about pancreatitis (chronic abdominal pain, alcohol use), steroid use, Cushing features, acromegaly features, haemochromatosis (skin pigmentation, hepatomegaly, gonadal failure)
Domain 3 — Risk Factors: Elicit modifiable risk factors systematically: central obesity (waist circumference — the single best anthropometric predictor of metabolic risk in Indians), physical inactivity, high-calorie/low-fibre diet (high refined carbohydrate intake, sugar-sweetened beverages), family history (first-degree relative with T2DM doubles risk), history of gestational diabetes or delivery of a macrosomic baby (>4 kg), polycystic ovary syndrome (PCOS — a strong T2DM risk factor through insulin resistance).
Domain 4 — Complications Screen: This is the most clinically consequential part of the history. Screen systematically:
- Eyes: Visual blurring, floaters, sudden visual loss (vitreous haemorrhage), photopsia
- Kidneys: Ankle oedema, frothy urine (proteinuria), nocturia
- Feet/peripheral neuropathy: Numbness, tingling, burning pain in feet/legs (often worse at night — a cardinal feature of painful neuropathy), foot ulcers, trauma not noticed, foot deformity
- Cardiovascular: Chest pain or exertional dyspnoea (may be silent due to autonomic neuropathy — 'silent MI'), palpitations, orthostatic dizziness (autonomic neuropathy)
- Genitourinary autonomic: Erectile dysfunction in men; urinary hesitancy, incomplete emptying (neurogenic bladder)
- Gastrointestinal: Early satiety, post-meal vomiting, bloating (gastroparesis); nocturnal diarrhoea (autonomic neuropathy)
Domain 5 — Medication History: Document current and past diabetes medications (type, dose, duration, tolerability, adherence). Identify drugs that impair glycaemia: corticosteroids (the most common cause of drug-induced hyperglycaemia), thiazide diuretics, beta-blockers (mask hypoglycaemic symptoms), atypical antipsychotics (clozapine, olanzapine), tacrolimus/cyclosporine.
Domain 6 — Lifestyle History: Dietary pattern (timing, carbohydrate load, fat intake), physical activity (type, frequency, duration), alcohol use (hypoglycaemia risk with sulphonylureas/insulin; also contributes to hypertriglyceridaemia and pancreatitis), smoking (major independent cardiovascular risk factor).
Domain 7 — Patient's Understanding and Adherence: Assess health literacy, previous diabetes education, self-monitoring practices, and concerns. In Indian practice, important cultural context includes home diet (rice-dominant diets, festival foods), financial constraints on medications, and family-structured decision-making that may affect adherence.
Systematic Physical Examination of the Diabetic Patient
The physical examination of the diabetic patient must be systematic and target-organ directed. A cursory general examination is insufficient — you are looking for evidence of existing microvascular and macrovascular complications, signs of metabolic syndrome, and clues to the type and duration of diabetes. The examination follows a logical sequence from general inspection to detailed organ-specific assessment.
General Inspection and Anthropometric Assessment:
Document height, weight, and calculate BMI (kg/m²); for Indians, use ≥23 kg/m² as overweight threshold. Measure waist circumference (at the level of the umbilicus): normal <90 cm in Indian men, <80 cm in Indian women — central obesity drives insulin resistance. Assess for acanthosis nigricans — a velvety, hyperpigmented thickening of skin in neck creases, axillae, and groin — pathognomonic of insulin resistance; present in many T2DM patients and PCOS. Look for lipodystrophy at injection sites (lipohypertrophy from repeated injection at the same site, causing erratic insulin absorption). Observe for necrobiosis lipoidica diabeticorum (pretibial plaques with yellow atrophic centre and telangiectatic border). Check for xanthomas (dyslipidaemia). Observe for cushingoid features or acromegalic features if secondary diabetes is suspected.
Blood Pressure:
Measure supine and standing (to detect orthostatic hypotension — a sign of cardiovascular autonomic neuropathy — defined as systolic BP drop ≥20 mmHg or diastolic ≥10 mmHg on standing). Target BP in diabetes is <130/80 mmHg. Document bilateral arm BP — a >15 mmHg difference suggests subclavian artery disease.
Cardiovascular Examination:
Auscultate for heart sounds, extra sounds (S3 — heart failure), and murmurs. Perform resting ECG (look for evidence of silent MI — Q waves, LBBB, ST changes). Note: in diabetic autonomic neuropathy, the normal heart rate variability with respiration (sinus arrhythmia) is lost — a fixed resting tachycardia is a sign. Palpate for carotid bruits (cerebrovascular disease).
Fundoscopic Examination:
This is a mandatory component of every diabetic examination. Pupils should ideally be dilated with tropicamide for adequate visualisation, though direct ophthalmoscopy through undilated pupils is acceptable as a bedside screen. Systematically examine: the optic disc (pallor, papilloedema, neovascularisation at disc — NVD), the macula (macular oedema appears as retinal thickening; hard exudates near the macula), and the four quadrants for haemorrhages, microaneurysms, cotton-wool spots, and neovascularisation elsewhere (NVE). Grade the retinopathy: No DR / Mild NPDR (microaneurysms only) / Moderate NPDR (+ haemorrhages/hard exudates, but no NV) / Severe NPDR (4-2-1 rule: haemorrhages in all 4 quadrants, venous beading in 2, IRMA in 1) / Proliferative DR (NVD, NVE, vitreous haemorrhage, fibrous proliferation).
Examination of Peripheral Pulses and Peripheral Arterial Disease (PAD):
Palpate all peripheral pulses bilaterally: femoral, popliteal, posterior tibial, and dorsalis pedis. Grade their strength (present, reduced, absent). Note asymmetry. Auscultate femoral arteries for bruits. In the foot, observe for pallor on elevation and dependent rubor (elevation pallor: ischaemic foot turns white when elevated; dependent rubor: turns red when lowered). Calculate the ankle-brachial pressure index (ABPI) when Doppler is available: normal >0.9; <0.9 = PAD; >1.3 = calcified vessels (non-compressible, common in diabetes).
Detailed Foot Examination (the Diabetic Foot Screen):
The diabetic foot examination is a distinct clinical skill that must be performed at every diabetic review. It has four components:
1. Inspection: Skin colour (pallor, cyanosis, redness), temperature (cool = ischaemic; warm = infected or Charcot), moisture (dry/anhidrotic skin = autonomic neuropathy), calluses (pressure points at risk for breakdown), nail changes (onychomycosis, ingrowing nails), deformities (hammer toes, hallux valgus, Charcot neuroarthropathy — warm, swollen, painless foot with bony destruction), ulcers (document site, size, depth, base, edge, surrounding skin, and Wagner grade)
2. Vascular assessment: Capillary refill time, palpation of DP and PT pulses
3. Neurological assessment (neuropathy screen): Use the 10 g monofilament (Semmes-Weinstein) — applied to 10 sites on the plantar surface; inability to detect the monofilament predicts loss of protective sensation. Test vibration sense with a 128 Hz tuning fork (hallux and medial malleolus). Test pin-prick sensation (pain). Elicit the ankle jerk (absent or diminished = early sensory neuropathy)
4. Classification of ulcers: Use the Wagner Classification: Grade 0 (no ulcer, high risk foot) → Grade 1 (superficial ulcer) → Grade 2 (deep ulcer to tendon/capsule/bone) → Grade 3 (deep ulcer with osteomyelitis/abscess) → Grade 4 (partial gangrene) → Grade 5 (full foot gangrene)
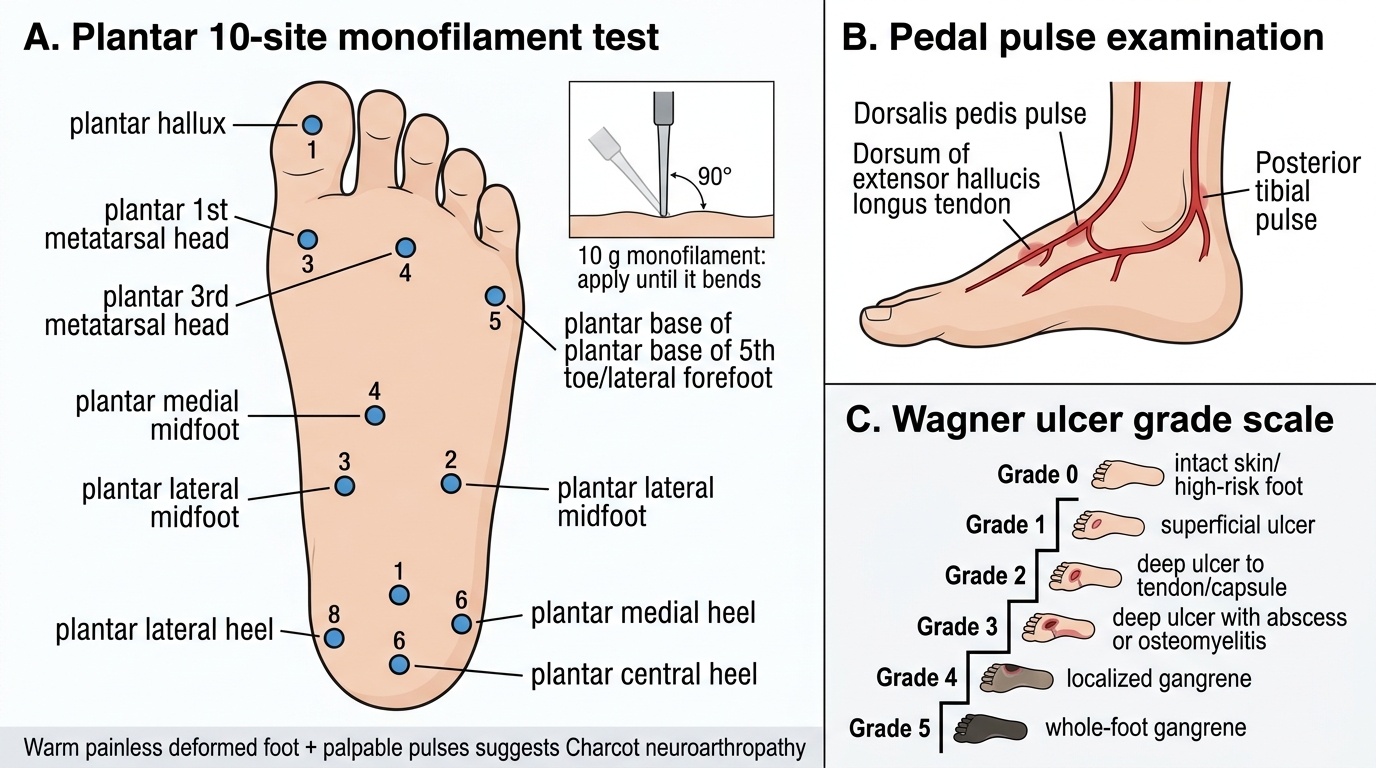
Diabetic Foot Examination: Sensory Testing, Pulses, and Wagner Grades
SELF-CHECK
During examination of a 62-year-old man with 15-year T2DM, you find the following in the right foot: skin is warm, the foot appears deformed with mid-foot bossing, but he reports NO pain despite an obvious bony deformity. His foot pulses are palpable. What is the MOST LIKELY diagnosis?
A. Acute gout causing painless arthropathy in immunocompromised diabetic
B. Peripheral arterial disease with bone remodelling from chronic ischaemia
C. Charcot neuroarthropathy (Charcot foot) due to severe peripheral neuropathy
D. Osteomyelitis of the mid-foot secondary to a penetrating ulcer
Reveal Answer
Answer: C. Charcot neuroarthropathy (Charcot foot) due to severe peripheral neuropathy
Charcot neuroarthropathy (Charcot foot) is the classic triad of: (1) a warm, (2) painless, (3) deformed foot in a patient with severe peripheral neuropathy and intact or preserved pulses. The warmth reflects increased blood flow from autonomic neuropathy causing arteriovenous shunting. The pain is absent because sensory neuropathy has eliminated protective pain. The deformity results from repeated microfractures that the patient cannot feel, leading to bony collapse and mid-foot 'rocker-bottom' deformity. This contrasts with ischaemic foot (cool, painful, pulseless) and osteomyelitis (usually associated with an overlying ulcer and fever).
Recognising the Clinical Features of Diabetic Emergencies
Recognising a diabetic emergency is a time-critical clinical skill. The three main emergencies — diabetic ketoacidosis (DKA), hyperosmolar hyperglycaemic state (HHS), and hypoglycaemia — each have a characteristic clinical signature that must be identified promptly. This section focuses on the bedside recognition skills corresponding to IM11.9.
Diabetic Ketoacidosis (DKA) — Clinical Recognition:
The classic picture is a young T1DM patient (though increasingly seen in T2DM and LADA) with a history of polyuria, vomiting, and abdominal pain over hours to a day or two. A precipitating event — infection, missed insulin, new diagnosis — is identifiable in over 80% of cases. On general inspection: ill-looking, dehydrated (dry mucous membranes, reduced skin turgor, sunken eyes), tachycardic, and hypotensive in severe cases. The pathognomonic respiratory finding is Kussmaul breathing — a very deep, regular, non-laboured respiratory pattern with slightly increased rate, representing maximal respiratory compensation for metabolic acidosis. The patient may have a sweet or fruity breath odour from acetone. Abdominal pain and tenderness (sometimes mimicking an acute abdomen — important to recognise as metabolic, not surgical, in the DKA context) are particularly prominent in children. Consciousness is preserved in mild-moderate DKA but deteriorates in severe DKA (pH <7.0, glucose >500 mg/dL, bicarbonate <5 mEq/L). Fever, if present, suggests a precipitating infection.
Hyperosmolar Hyperglycaemic State (HHS) — Clinical Recognition:
The typical picture is an elderly T2DM patient — often with another acute illness (pneumonia, stroke, MI, UTI) or undiagnosed diabetes — presenting after a prolonged period (days to a week) of increasingly poor oral intake and polyuria. On examination: profoundly dehydrated (skin turgor markedly reduced, dry mucous membranes, tachycardia, oliguria or anuria), but the respiratory pattern is NOT Kussmaul (no acidosis, pH normal). The dominant clinical feature is neurological impairment — ranging from confusion and agitation to focal neurological deficits (hemiparesis, aphasia, seizures — which can be focal or generalised), and coma in severe cases. These neurological features result from cerebral dehydration secondary to extreme hyperosmolality. The absence of Kussmaul breathing and ketotic breath (no significant ketones) distinguishes HHS from DKA at the bedside — though in practice, a mixed picture occurs in approximately 30% of cases.
Hypoglycaemia — Clinical Recognition:
Hypoglycaemia (blood glucose <70 mg/dL) presents with two overlapping clusters of symptoms that reflect the underlying physiology. Adrenergic (autonomic) symptoms — sweating, tremor, palpitations, pallor, and hunger — result from counter-regulatory adrenaline release at approximately 60–65 mg/dL and serve as the warning signs. Neuroglycopenic symptoms — confusion, difficulty concentrating, slurred speech, focal neurological deficits (hemiparesis, visual disturbances), seizures, and coma — develop as cerebral glucose supply becomes inadequate at lower glucose levels (<50 mg/dL). A critical bedside distinction: in patients with hypoglycaemia unawareness (autonomic neuropathy from longstanding T1DM, or recurrent hypoglycaemia), the adrenergic warning symptoms are absent and the patient passes directly to neuroglycopenia without warning, making severe hypoglycaemia particularly hazardous. Any patient on insulin or sulphonylurea who is confused, combative, or unconscious has hypoglycaemia until proven otherwise — immediate bedside glucose measurement before any other investigation.
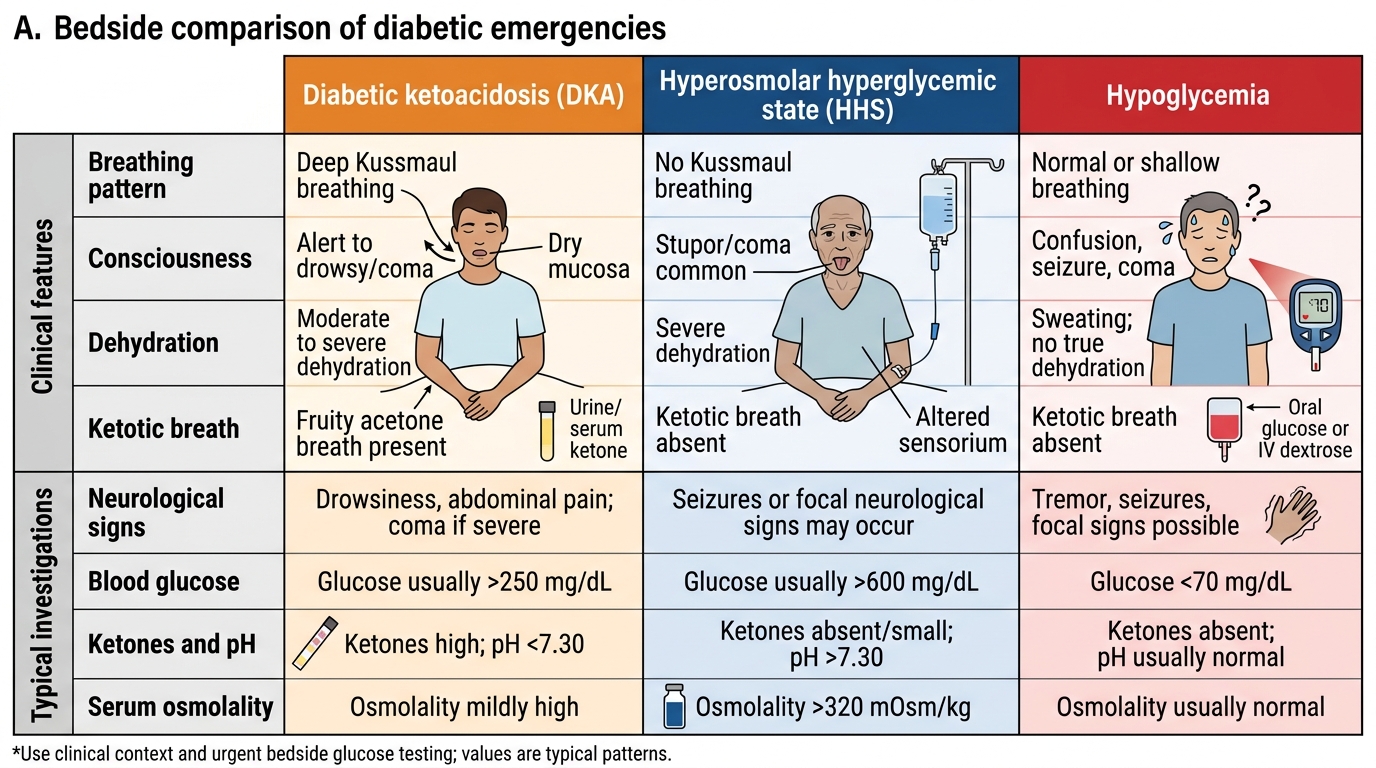
Bedside Recognition of Diabetic Emergencies