Page 5 of 23
IM11.7-10 | Diabetes Clinical Evaluation — SDL Guide (Part 2)
Generating a Differential Diagnosis and Prioritising by Aetiology
Generating a differential diagnosis for a patient presenting with hyperglycaemia or suspected diabetes requires a structured approach that integrates the history and examination findings to assign probability to different aetiologies and prioritise the most immediately actionable diagnoses. This corresponds to IM11.10. The skill is not simply listing all types of diabetes but applying clinical reasoning to arrive at the most likely type, identify any secondary cause that may be reversible, and flag the emergency presentations that require immediate action.
Step 1 — Is this an emergency or a chronic presentation? Before generating a differential, rapidly assess for evidence of DKA, HHS, or hypoglycaemia. These are not differentials to be contemplated — they are emergencies to be recognised and treated simultaneously with investigation. Kussmaul breathing in a young patient with hyperglycaemia = DKA until proven otherwise. Extreme hyperglycaemia (random glucose >500 mg/dL) in an elderly confused patient = HHS until proven otherwise. Confusion or coma in a patient on insulin/sulphonylurea = hypoglycaemia until proven otherwise.
Step 2 — Classify the likely type using the clinical profile:
| Feature | Suggests T1DM | Suggests T2DM | Suggests MODY | Suggests Secondary |
|---|---|---|---|---|
| Age | <40 (often <20) | >40 (but any age) | <30, young adult | Any |
| BMI | Normal/lean | Overweight/obese | Lean | Varies |
| Onset speed | Acute (days-weeks) | Insidious | Mild, insidious | Varies |
| Family history | Not strong T2DM pattern | Strong T2DM | Autosomal dominant | Depends on cause |
| Ketonuria at diagnosis | Present | Absent/mild | Absent | Absent |
| Response to oral agents | Non-responder | Responder | SU-sensitive (HNF1A) | Varies |
| Associated features | None specific | MetS, acanthosis | None | Cushingoid, acromegalic |
Step 3 — Screen for secondary causes actively:
Ask about: long-term steroid use (Cushing's disease vs exogenous), signs of acromegaly (jaw/hand enlargement, coarsened features — growth hormone excess), haemochromatosis (bronze skin, hepatomegaly, gonadal failure, cardiac disease — screen with serum ferritin and transferrin saturation), chronic pancreatitis (recurrent epigastric pain, alcohol history, malabsorption), phaeochromocytoma (episodic hypertension, sweating, headache — the 'spell' triad), and glucagonoma (necrolytic migratory erythema, weight loss, diarrhoea).
Step 4 — Prioritise based on the clinical urgency and the consequences of missing the diagnosis:
In the differential for hyperglycaemia, always ask: (1) Could this be drug-induced? (Often reversible — stop the offending drug.) (2) Could this be MODY? (Matters for management — HNF1A-MODY responds to tiny SU doses, avoids insulin.) (3) Could there be an underlying adrenal, pituitary, or pancreatic tumour? (Delay in diagnosis has major consequences.) (4) Is the patient in a current hyperglycaemic emergency requiring immediate resuscitation? (This supersedes the diagnostic workup.)
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
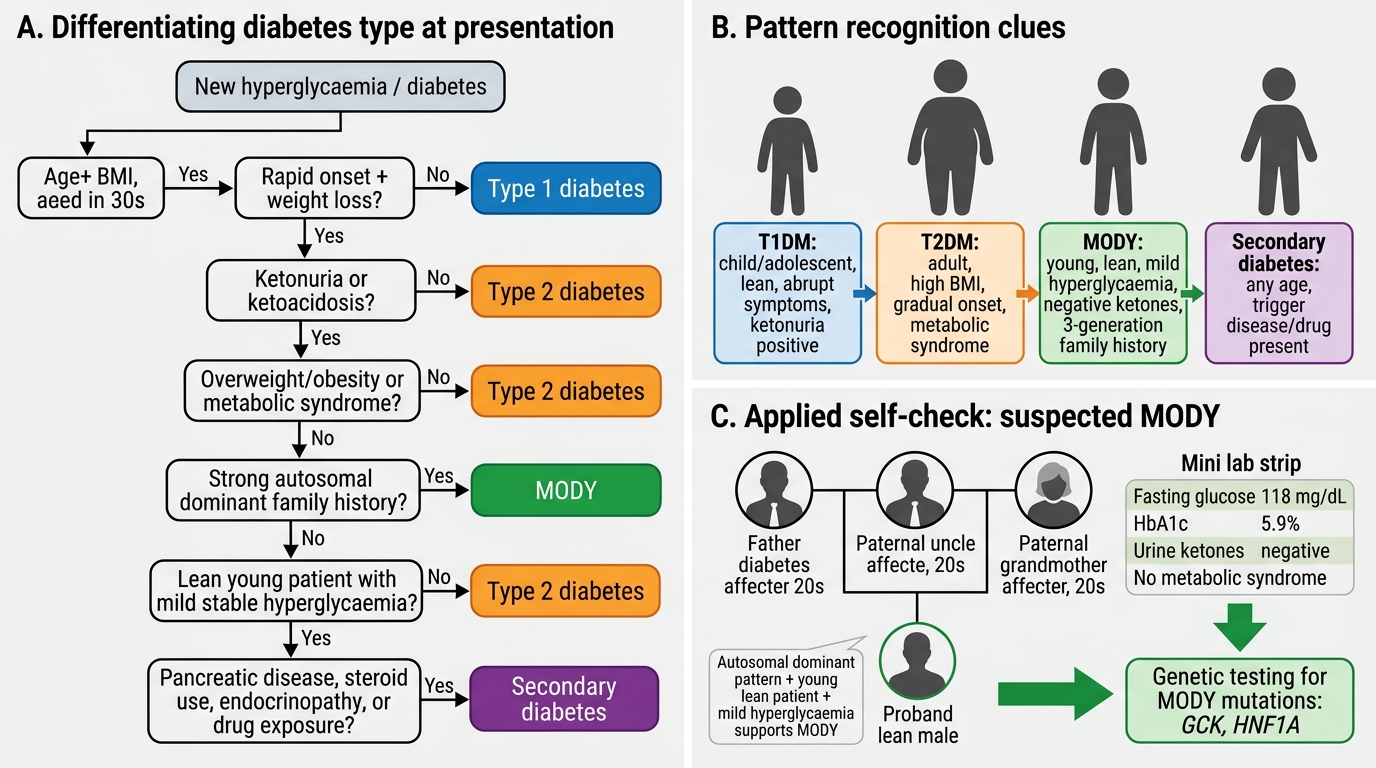
Clinical Algorithm for Differentiating Diabetes Types
SELF-CHECK
A 28-year-old lean man is found to have fasting glucose 118 mg/dL. His father, paternal uncle, and paternal grandmother all have diabetes, diagnosed in their 20s. His HbA1c is 5.9% and urinary ketones are negative. He has no features of metabolic syndrome. What is the MOST appropriate next investigation?
A. Repeat fasting glucose in 3 months and lifestyle advice only
B. Start metformin and review in 6 weeks
C. Genetic testing for MODY mutations (GCK, HNF1A)
D. Order anti-GAD antibodies to exclude LADA
Reveal Answer
Answer: C. Genetic testing for MODY mutations (GCK, HNF1A)
The clinical profile — young, lean, multiple generations with early-onset diabetes in an autosomal dominant pattern, mild hyperglycaemia — is characteristic of MODY (Maturity-Onset Diabetes of the Young), a monogenic form. MODY genetic testing (initially GCK-MODY for mild stable hyperglycaemia, or HNF1A/HNF4A-MODY for progressive hyperglycaemia with SU sensitivity) is the appropriate next investigation. This matters practically: GCK-MODY requires no pharmacological treatment and lifestyle modification alone is appropriate; HNF1A-MODY is exquisitely sensitive to low-dose sulphonylureas. Anti-GAD would be appropriate for LADA (autoimmune T1DM in adults) — the history here has no features of T1DM or autoimmune disease.
Applied Practice: The Complete Diabetic Review
Synthesising history and examination into a structured clinical review is the expected standard for a final-year medical student. In the diabetes clinic or ward, a complete review follows a reproducible framework that ensures no complication is overlooked and no risk factor goes unaddressed. The process of integrating history, examination, and investigation findings into a single coherent picture — and translating that picture into an individualised management plan — is the hallmark of the competent clinician. For the diabetic patient, this integrated review is not a one-time exercise but a recurring encounter at every visit, because the disease evolves over time and the pattern of complications changes. What was absent on last year's review may be present and clinically significant today. The framework below integrates all four NMC competency components (IM11.7–11.10) into a single clinical encounter that can be executed in 30–45 minutes in any outpatient setting. Every component has equal clinical weight — a meticulous history that is not paired with a careful examination provides incomplete information, just as a thorough examination without a structured history misses the contextual factors that determine management. The integration of all four elements into a single, efficient, patient-centred review is the standard of diabetological care expected in Indian clinical practice at the level of a postgraduate-ready intern.
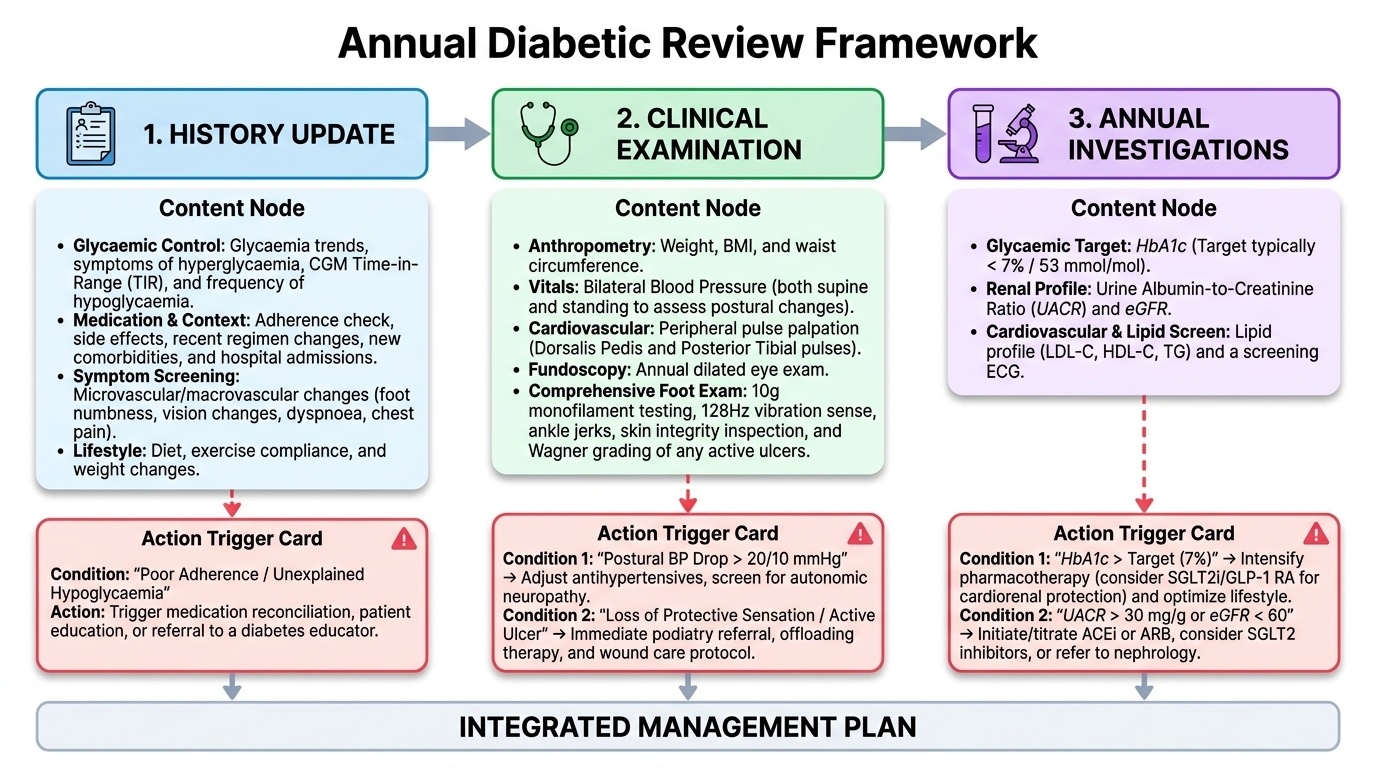
Provided image
The Annual Diabetic Review Framework (applicable to all T2DM patients and T1DM patients in clinic):
History update:
- Glycaemic control since last visit (symptoms of hyperglycaemia, frequency of hypoglycaemia, time in range if using CGM)
- Medication changes and adherence
- New symptoms suggesting complications (foot, eye, kidney, cardiovascular)
- Lifestyle changes (diet, exercise, weight change)
- New medications, comorbidities, or hospital admissions
Examination:
- Weight, BMI, waist circumference
- Blood pressure (bilateral, supine and standing)
- Cardiovascular examination including peripheral pulses
- Fundoscopy (dilated where possible, at least annually)
- Complete foot examination (monofilament, vibration, ankle jerks, DP/PT pulses, skin inspection, Wagner grading of any ulcers)
Investigations to order at annual review:
- HbA1c (glycaemic control target typically <7% or <53 mmol/mol for most patients, individualised)
- Fasting lipid profile (LDL-C target <2.6 mmol/L / 100 mg/dL for most; <1.8 mmol/L / 70 mg/dL if established CVD)
- Urinary ACR (albumin-creatinine ratio — early nephropathy screen)
- Serum creatinine and eGFR
- Urine routine (for proteinuria, infection)
- ECG (annual in patients >40 years or those with hypertension)
Key examination integration example:
A patient with: (1) absent ankle jerks + reduced monofilament sensation bilaterally = sensorimotor neuropathy (high foot ulcer risk → foot care education, footwear referral); (2) absent DP and PT pulses + ABPI 0.7 = peripheral arterial disease (refer vascular surgery); (3) hard exudates near the macula + 2 areas of neovascularisation = proliferative diabetic retinopathy (urgent ophthalmology referral for panretinal photocoagulation); (4) ACR 85 mg/mmol + eGFR 52 = macroalbuminuria + CKD G3a → start/titrate ACE inhibitor or ARB, consider SGLT2i for renoprotection.
SELF-CHECK
During a diabetic foot examination, a 68-year-old T2DM patient is unable to detect the 10 g monofilament at 6 of 10 sites on the right plantar surface. Her right dorsalis pedis pulse is absent and her right posterior tibial pulse is reduced. She has a 2 cm ulcer on the right first metatarsal head that penetrates to the tendon sheath. What is the Wagner grade of this ulcer, and what is the MOST urgent referral?
A. Wagner Grade 1 ulcer; refer to podiatry for offloading
B. Wagner Grade 2 ulcer; refer to both ophthalmology and vascular surgery
C. Wagner Grade 2 ulcer; urgent referral to vascular surgery and wound management
D. Wagner Grade 3 ulcer; immediate surgical debridement required
Reveal Answer
Answer: C. Wagner Grade 2 ulcer; urgent referral to vascular surgery and wound management
A 2 cm ulcer penetrating to the tendon sheath without evidence of osteomyelitis or abscess is a Wagner Grade 2 ulcer (deep ulcer to tendon or joint capsule, without bone involvement). Wagner Grade 3 would require osteomyelitis or abscess. The absent DP pulse and reduced PT pulse indicate significant peripheral arterial disease coexisting with neuropathy — a neuroischaemic foot ulcer, which is the highest-risk category. The most urgent referral is vascular surgery (to assess for revascularisation) plus specialist wound management. Ophthalmology is important but not the most urgent referral for this acute foot situation.
Self-Assessment: Integrating the Diabetic Evaluation
The four competencies of the diabetic clinical evaluation — history, examination, emergency recognition, and differential diagnosis — are best consolidated through integrated case scenarios that mirror the clinical encounter. The scenarios below require you to apply all four competency domains simultaneously, as you would in a real ward or clinic setting. For each scenario, work through your response before reading the analysis. Focus on the logical sequence: emergency recognition first, then history interpretation, then examination findings, then differential formulation.
Scenario A: A 19-year-old student with known T1DM for 4 years is brought to casualty at 2 am by a friend. She is rousable but confused. Her breath smells sweet. She is tachycardic at 112/min and her respiratory rate is 24/min with deep breaths. Blood glucose on a glucometer is 420 mg/dL. What emergency do you suspect, and what are the three bedside investigations you would order immediately?
Analysis: The constellation of hyperglycaemia (420 mg/dL) + deep Kussmaul breathing + sweet acetone breath + confusion in a young T1DM patient = DKA until proven otherwise. Immediate bedside investigations: (1) Urine dipstick for ketones — expected 3+ or 4+, (2) Venous blood gas or ABG for pH and bicarbonate — expected pH <7.3, HCO₃ <18 mEq/L, (3) Serum electrolytes for potassium — essential before insulin administration (hypokalaemia must be corrected first or insulin will worsen it). Blood glucose is already known. Blood cultures and urine culture should follow to identify precipitating infection.
Scenario B: A 72-year-old retired teacher with T2DM on metformin, not seen in clinic for two years, presents to your general medicine OPD for a routine check-up. His HbA1c was last recorded at 8.9%. He reports no specific symptoms but on direct questioning mentions 'his feet feel like wood.' On examination you find bilateral absent ankle jerks, inability to detect the 10 g monofilament at 7 of 10 sites on each foot, bounding dorsalis pedis pulses bilaterally, and on fundoscopy (undilated): several dot haemorrhages and hard exudates in the right temporal field. What complications have you identified, and what is the most urgent referral today?
Analysis: Complications identified: (1) Peripheral sensorimotor neuropathy — absent ankle jerks, loss of protective sensation bilaterally (high foot ulcer risk); (2) Non-proliferative diabetic retinopathy — dot haemorrhages and hard exudates on undilated fundoscopy (urgent dilated fundoscopy required to rule out macular involvement or pre-proliferative change). No PAD (bounding DP pulses). The most urgent action is urgent ophthalmology referral for dilated retinal examination — undilated fundoscopy in a dim OPD may have missed proliferative changes or clinically significant macular oedema. Foot care education, footwear assessment, and podiatry referral are the next priorities.
Scenario C: A 45-year-old bank manager is referred to you with fasting glucose 112 mg/dL and HbA1c 5.8% — 'borderline prediabetes' in the referral letter. On taking a structured history you find: his father, paternal aunt, and one of his two brothers all have diabetes, diagnosed before age 35, none were obese. The patient himself is lean (BMI 21 kg/m²), physically active, and has no features of metabolic syndrome. His waist circumference is 79 cm. How does this history change your differential, and what next investigation would confirm your suspicion?
Analysis: This is NOT straightforward prediabetes or T2DM risk. The multigenerational, autosomal-dominant pattern of early-onset diabetes in lean individuals raises strong suspicion for MODY (Maturity-Onset Diabetes of the Young), most likely GCK-MODY (glucokinase mutation) given the mild stable hyperglycaemia. Confirming investigation: molecular genetic testing for GCK and HNF1A/HNF4A mutations. GCK-MODY is important to identify because it requires only lifestyle modification — no pharmacological treatment is needed and the hyperglycaemia is mild and non-progressive. Treating it as T2DM risk and starting preventive pharmacotherapy would be inappropriate.
Integrated Diabetic Evaluation
CLINICAL PEARL
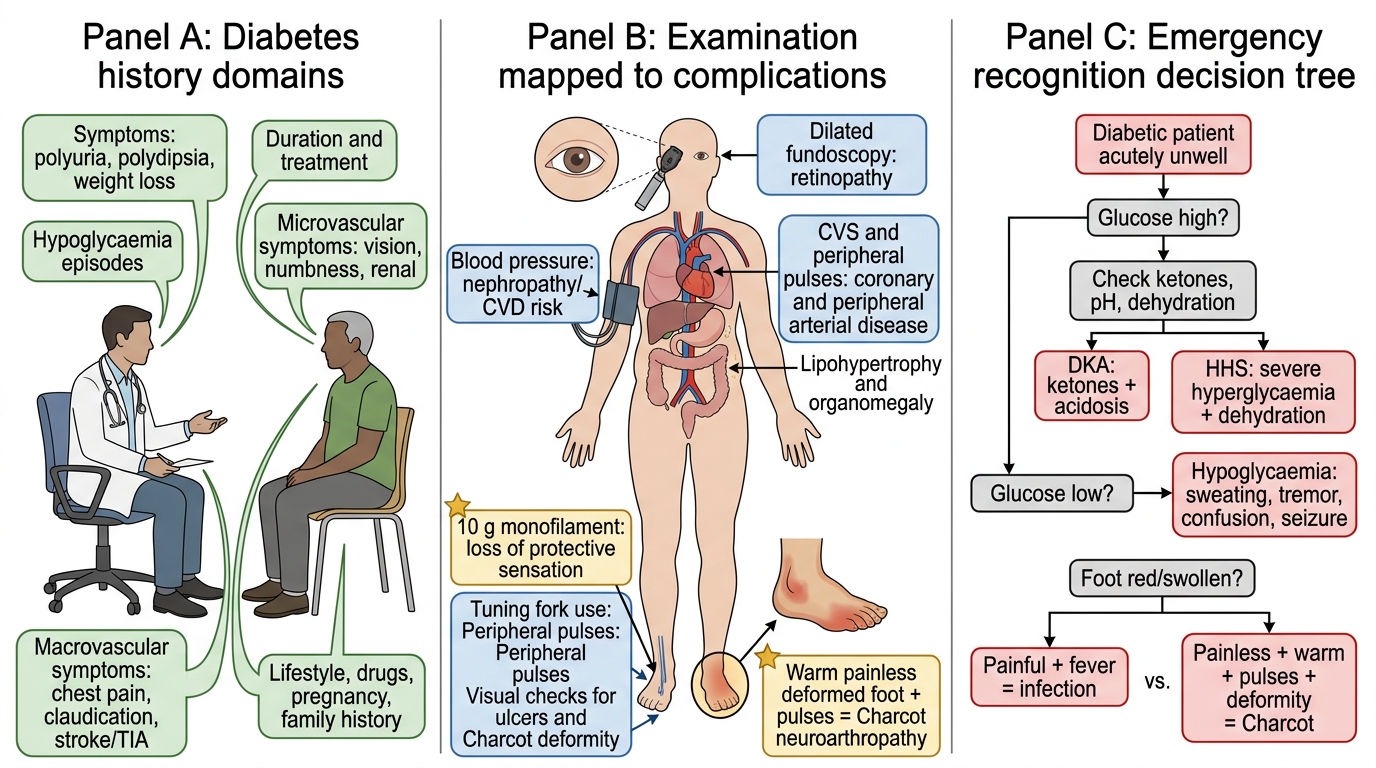
The diabetic foot examination is one of the most neglected and highest-yield clinical skills in diabetology. Three pearls to remember:
- The 10 g monofilament is the single most important screening tool for loss of protective sensation. A patient who cannot feel the monofilament at 4 or more of 10 sites has lost protective sensation and is at high risk of a painless ulcer. This is entirely asymptomatic — the patient cannot tell you they have this problem.
- A warm, painless, deformed foot with palpable pulses = Charcot neuroarthropathy — NOT infection. These patients get misdiagnosed and treated for gout or cellulitis, and the Charcot foot collapses further. Correct management is non-weight-bearing immobilisation and urgent orthopaedic/diabetology referral.
- Fundoscopy must be performed with dilated pupils whenever possible. Non-dilated fundoscopy misses peripheral retinopathy and is inadequate for diabetic screening. If you cannot dilate in the clinic, refer to ophthalmology — do not leave fundoscopy unperformed.