Page 8 of 23
IM11.11-13 | Diabetes Diagnostic Testing — SDL Guide (Part 2)
Interpretation of the Integrated Diagnostic Panel in Clinical Scenarios
Integrating multiple diagnostic tests into a coherent clinical interpretation is a higher-order skill that goes beyond knowing individual reference ranges. In clinical practice, you will rarely receive a single test in isolation — you will be given a full set of results and asked to synthesise them into a diagnostic conclusion and management plan. This section applies the tests covered in the preceding content blocks to representative clinical scenarios, demonstrating the applied interpretation required by IM11.11.
Scenario A — Diagnosing Diabetes in a Symptomatic Patient:
A 54-year-old man with 2-week history of polyuria and polydipsia. CBG at triage: 312 mg/dL. Laboratory results: fasting plasma glucose 274 mg/dL; HbA1c 9.8%; urinary ketones trace; urine ACR 18 mg/mmol; serum creatinine 88 μmol/L; eGFR 78; fasting lipid profile: total cholesterol 6.1, LDL-C 3.8, HDL-C 0.9, triglycerides 3.2 mmol/L.
Interpretation: Unequivocal diabetes: random glucose 312 mg/dL with classic symptoms (no confirmation needed). HbA1c 9.8% confirms longstanding poor glycaemic control. ACR 18 mg/mmol is in the microalbuminuria range (3–30) — early diabetic nephropathy. eGFR 78 = CKD G2. Dyslipidaemia: very high triglycerides (3.2 mmol/L) and low HDL-C (0.9 mmol/L) — the classic diabetic dyslipidaemia pattern; LDL-C 3.8 is above target. Trace ketones in an apparent T2DM patient with 2-week symptoms — likely stress-induced mild ketosis, not DKA (no metabolic acidosis, conscious, not vomiting).
Scenario B — Distinguishing DKA from HHS using the Diagnostic Panel:
Two patients arrive simultaneously:
- Patient 1 (19F, T1DM): glucose 380 mg/dL, urinary ketones 4+, ABG: pH 7.19, HCO₃ 8 mEq/L, anion gap 28 mEq/L; K+ 3.2 mEq/L, Na+ 131 mEq/L (corrected Na = 131 + [1.6 × (380-100)/100] = 131 + 4.5 = 135.5 mEq/L); serum osmolality 298 mOsm/kg
- Patient 2 (74M, known T2DM): glucose 720 mg/dL, urinary ketones negative, ABG: pH 7.38, HCO₃ 22 mEq/L, anion gap 10 mEq/L; Na+ 148 mEq/L (corrected: 148 + [1.6 × (720-100)/100] = 148 + 9.9 = 157.9 mEq/L); serum osmolality 352 mOsm/kg; creatinine 310 μmol/L, eGFR 18
Interpretation: Patient 1 = DKA: high anion gap metabolic acidosis (pH 7.19, HCO₃ 8, anion gap 28), ketonaemia (4+ urinary ketones), moderate hyperglycaemia. K+ 3.2 — critically low despite acidosis (total body K+ depletion); replace K+ before insulin. Corrected Na normal. Patient 2 = HHS: extreme hyperglycaemia (720 mg/dL), no ketosis, no acidosis, markedly elevated osmolality (352 > 320), very high corrected Na (hypernatraemia from free water loss), acute kidney injury (creatinine 310, eGFR 18 — pre-renal from extreme dehydration). Total body water deficit estimated at 10–12 L.
Scenario C — Monitoring DKA Treatment:
A patient with DKA is being treated. Serial ABG and electrolyte results:
| Time | pH | HCO₃ | K+ | Glucose | Ketones (urine) |
|---|---|---|---|---|---|
| 0h | 7.12 | 6 | 5.8 | 510 | 4+ |
| 2h | 7.24 | 10 | 3.9 | 320 | 4+ |
| 4h | 7.33 | 16 | 3.1 | 180 | 4+ |
| 6h | 7.38 | 21 | 2.8 | 130 | 4+ |
Interpretation: pH and bicarbonate are consistently improving (treatment effective). Glucose is falling appropriately. However, the K+ is progressively dropping and is now 2.8 mEq/L — CRITICAL. Insulin drives K+ into cells, worsening the existing total body depletion. At K+ <3.0, insulin must be paused or slowed and K+ replacement must be aggressively increased. The urine ketones remaining 4+ throughout is expected (BHB→acetoacetate conversion; blood BHB would have fallen). This scenario reinforces: follow the pH and K+, not the urine ketone strip, to guide DKA treatment.
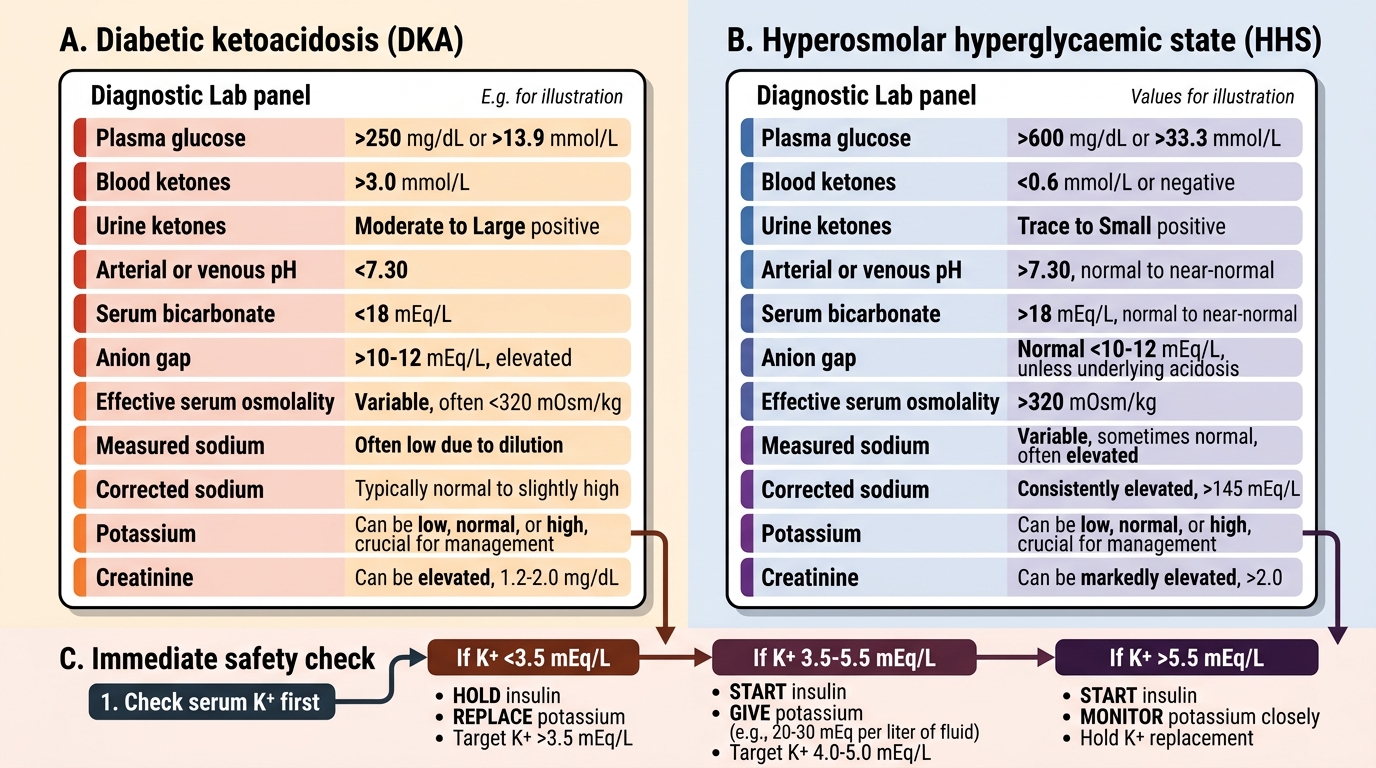
DKA versus HHS: Diagnostic Panel Comparison
SELF-CHECK
A patient with DKA has the following results at initial assessment: glucose 480 mg/dL, pH 7.21, bicarbonate 9 mEq/L, sodium 136 mEq/L, potassium 5.6 mEq/L, chloride 104 mEq/L. You are about to start insulin infusion. What is the MOST important action to take FIRST?
A. Start insulin infusion immediately at 0.1 units/kg/hr and recheck potassium in 2 hours
B. Administer sodium bicarbonate to correct the metabolic acidosis before insulin
C. Recheck serum potassium and hold insulin until potassium is confirmed ≥3.5 mEq/L
D. Calculate the corrected sodium and start normal saline at 1 L/hr
Reveal Answer
Answer: C. Recheck serum potassium and hold insulin until potassium is confirmed ≥3.5 mEq/L
In DKA, the serum potassium is typically elevated or normal despite severe total body potassium depletion (insulin deficiency causes extracellular shift of K+; acidosis worsens this). When insulin is given, it rapidly drives K+ into cells — if the serum K+ is already borderline (3.5–5.0 mEq/L) or low (<3.5), insulin can precipitate dangerous hypokalaemia causing cardiac arrhythmias. Standard protocol: if K+ <3.5 mEq/L, hold insulin and replace K+ first. If K+ 3.5–5.5 mEq/L, start insulin with concurrent K+ replacement. If K+ >5.5 mEq/L, start insulin without immediate K+ replacement but monitor closely. The initial K+ here is 5.6 — borderline high — so insulin can start with close K+ monitoring. However, the question is testing the principle: always confirm K+ ≥3.5 before starting insulin. Sodium bicarbonate is not routinely recommended even in severe DKA (reserved for pH <6.9).
Applied Practice: Common Diagnostic Pitfalls and Decision Points
Translating knowledge of individual diagnostic tests into sound clinical decision-making requires awareness of the situations where tests mislead — and what to do when they do. This section covers the most clinically consequential applied scenarios that arise when using the diabetes diagnostic panel, and trains you to make the right call when standard interpretations break down or conflict.
Provided image
Pitfall 1 — Conflicting FPG and HbA1c results:
A patient has FPG 131 mg/dL (meets diabetes threshold) but HbA1c 5.9% (below the 6.5% diabetes threshold). This apparent contradiction occurs when: (a) the hyperglycaemia is relatively recent and HbA1c has not yet caught up (HbA1c reflects 8–12 weeks of average glucose; a few weeks of hyperglycaemia may not elevate it above 6.5%); or (b) the patient has iron deficiency anaemia (falsely low HbA1c — needs checking); or (c) the FPG was not truly fasting. Resolution: establish fasting status, check a full blood count and iron studies, repeat the FPG. Use laboratory confirmation on two separate occasions. If iron deficiency is found, treat it and repeat HbA1c.
Pitfall 2 — Normal glucose, positive urine ketones:
A patient on an SGLT2 inhibitor has urine ketones 2+ but blood glucose 142 mg/dL. The classic DKA presentation (glucose >250) does not apply here. SGLT2 inhibitors promote glycosuria and shift metabolism toward fat oxidation. Euglycaemic DKA is a real risk with intercurrent illness, prolonged fasting, reduced insulin dose, or surgery in SGLT2i users. Action: measure blood beta-hydroxybutyrate; if elevated (>3.0 mmol/L), treat as DKA regardless of glucose level; stop SGLT2i immediately and do not restart until the episode is fully resolved.
Pitfall 3 — Haematocrit effects on CBG accuracy:
A patient with sickle cell disease has a haematocrit of 20% (severe anaemia). His glucometer reads 148 mg/dL but the laboratory plasma glucose is 118 mg/dL. In severe anaemia, the ratio of plasma to red cell volume is altered, causing most glucose oxidase electrochemical glucometers to overestimate glucose. Conversely, polycythaemia may cause underestimation. In patients with known haemolytic conditions, laboratory plasma glucose is always the reference standard and glucometer readings must be interpreted cautiously.
Pitfall 4 — K+ interpretation in DKA with alkalosis:
Occasionally DKA coexists with metabolic alkalosis (e.g., from prolonged vomiting or diuretic use). When the pH is relatively normal despite severe DKA, the serum K+ may be deceptively low because alkalosis promotes intracellular K+ shift independently. The total body K+ depletion may be greater than the serum level suggests. This reinforces the rule: check K+ at every stage of DKA management and never assume the initial K+ reflects the trajectory once treatment begins.
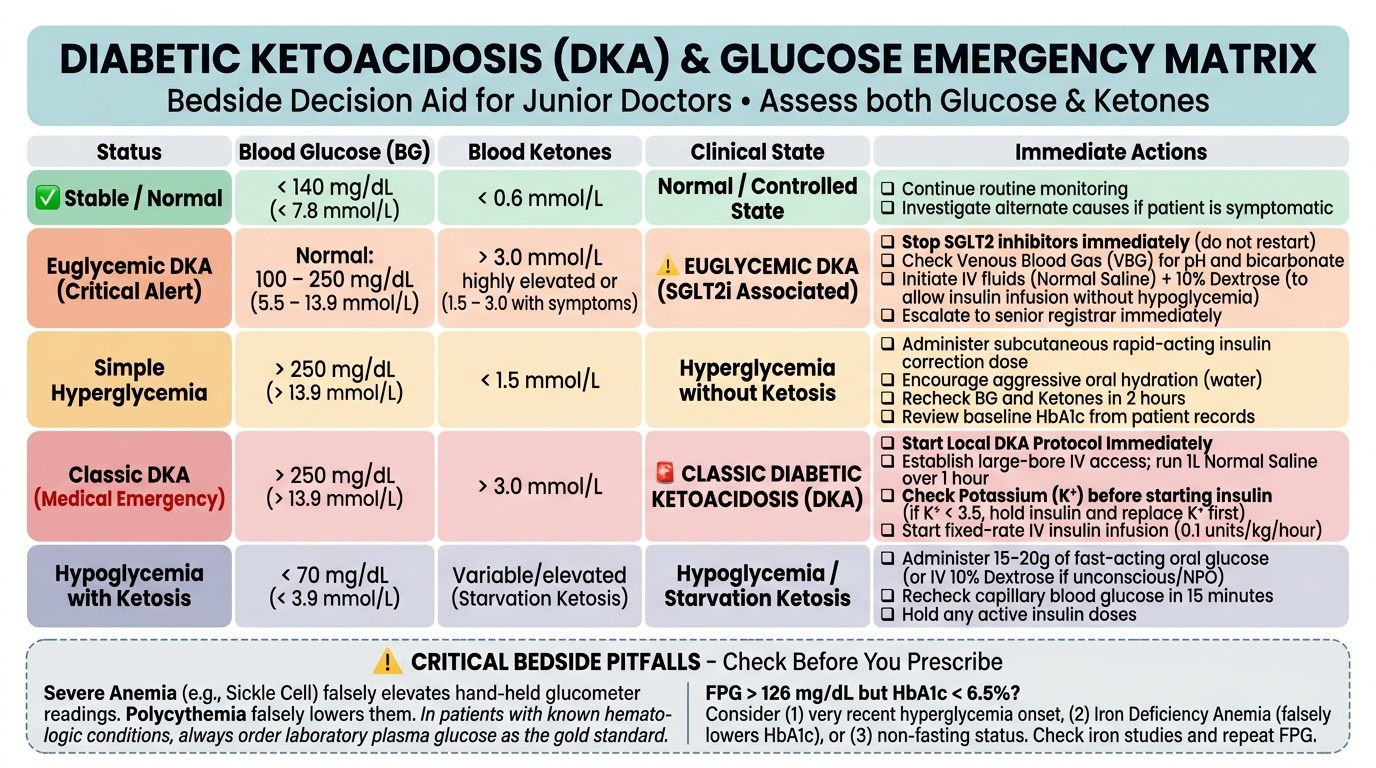
Making the '15-minute decision' at the bedside:
In an emergency, you will not always have laboratory confirmation before you must act. The following bedside algorithm uses only the glucometer and urine dipstick to guide immediate action:
| Glucose (CBG) | Urine Ketones | Clinical Status | Immediate Action |
|---|---|---|---|
| <70 mg/dL | Negative | Conscious | 15 g fast-acting carbs, recheck in 15 min |
| <70 mg/dL | Negative | Unconscious | IV 50% dextrose 25 mL or IM glucagon |
| 250–600 mg/dL | 2+ or more | Tachycardic, Kussmaul | Treat as DKA: IV fluids, check electrolytes and ABG urgently |
| >600 mg/dL | Negative | Confused, dehydrated | Treat as HHS: IV fluids (0.9% NaCl), electrolytes urgently |
| Any level | Any | On SGLT2i + unwell | Check blood BHB; treat as DKA if BHB >3.0 regardless of glucose |
Self-Assessment: Test Interpretation in Clinical Context
The diagnostic testing competencies (IM11.11–11.13) require you to be fluent not only in the technical steps of each test but in the contextual interpretation that converts a laboratory number into a clinical action. The scenarios and questions below reinforce this applied level of reasoning. Attempt each question before reading the analysis.
Scenario A: A 38-year-old woman is screened for diabetes at her annual check-up. Her fasting plasma glucose (FPG) is 131 mg/dL. She is asymptomatic. She is sent home and returns 10 days later for a repeat test: FPG is 129 mg/dL. Her HbA1c from the same sample is 6.8%. Does she have diabetes, and on the basis of which tests?
Analysis: Yes, she has diabetes. The ADA diagnostic criteria require any ONE of the four criteria on two occasions (absent unequivocal hyperglycaemia with symptoms). Here: FPG ≥126 mg/dL confirmed on two separate days (131 and 129), and HbA1c ≥6.5% (6.8%). Any one of these, confirmed, establishes the diagnosis. Three positive tests on two separate occasions provide unequivocal confirmation. Note that FPG 129 mg/dL on repeat (the threshold is 126) — both readings meet the diagnostic criterion.
Scenario B: A 28-year-old T1DM patient uses a glucometer to check her glucose before lunch: the result is 62 mg/dL. She feels well with no symptoms. Should she treat this reading, and what is the correct first-line treatment?
Analysis: Yes, this is hypoglycaemia (glucose <70 mg/dL) and should be treated even in an asymptomatic patient, because absence of symptoms may reflect hypoglycaemia unawareness or simply the early neuroglycopenic threshold not yet reached. The first-line treatment is the 15–15 rule: give 15 g of fast-acting carbohydrate (e.g., 150 mL of fruit juice, 3–4 glucose tablets, or 4–5 sugar sachets dissolved in water), recheck glucose in 15 minutes, and repeat if still <70 mg/dL. Once glucose is back in the normal range, a small snack with complex carbohydrate + protein should be taken if the next meal is more than an hour away, to prevent recurrence.
Scenario C: A urine dipstick on a 45-year-old T2DM patient on an SGLT2 inhibitor (empagliflozin) shows trace ketones, glucose negative, and no protein or blood. The patient's blood glucose is 138 mg/dL. How do you interpret the ketone finding?
Analysis: SGLT2 inhibitors (empagliflozin, dapagliflozin, canagliflozin) promote glycosuria and can shift metabolism towards fat oxidation and mild ketogenesis even at near-normal blood glucose levels. Euglycaemic DKA is a recognised rare complication of SGLT2 inhibitors — DKA with blood glucose <250 mg/dL (sometimes as low as normal). Trace urinary ketones in an SGLT2i user with normal or mildly elevated glucose requires clinical assessment: Is the patient unwell? Any precipitating illness, surgery, or prolonged fasting? If asymptomatic with trace ketones and no precipitant, this can be monitored. However, if the patient has any symptoms (nausea, vomiting, fatigue, dyspnoea), blood ketones must be measured and SGLT2i should be withheld. The classic DKA warning (glucose >250) does not apply here — index of suspicion must be higher.
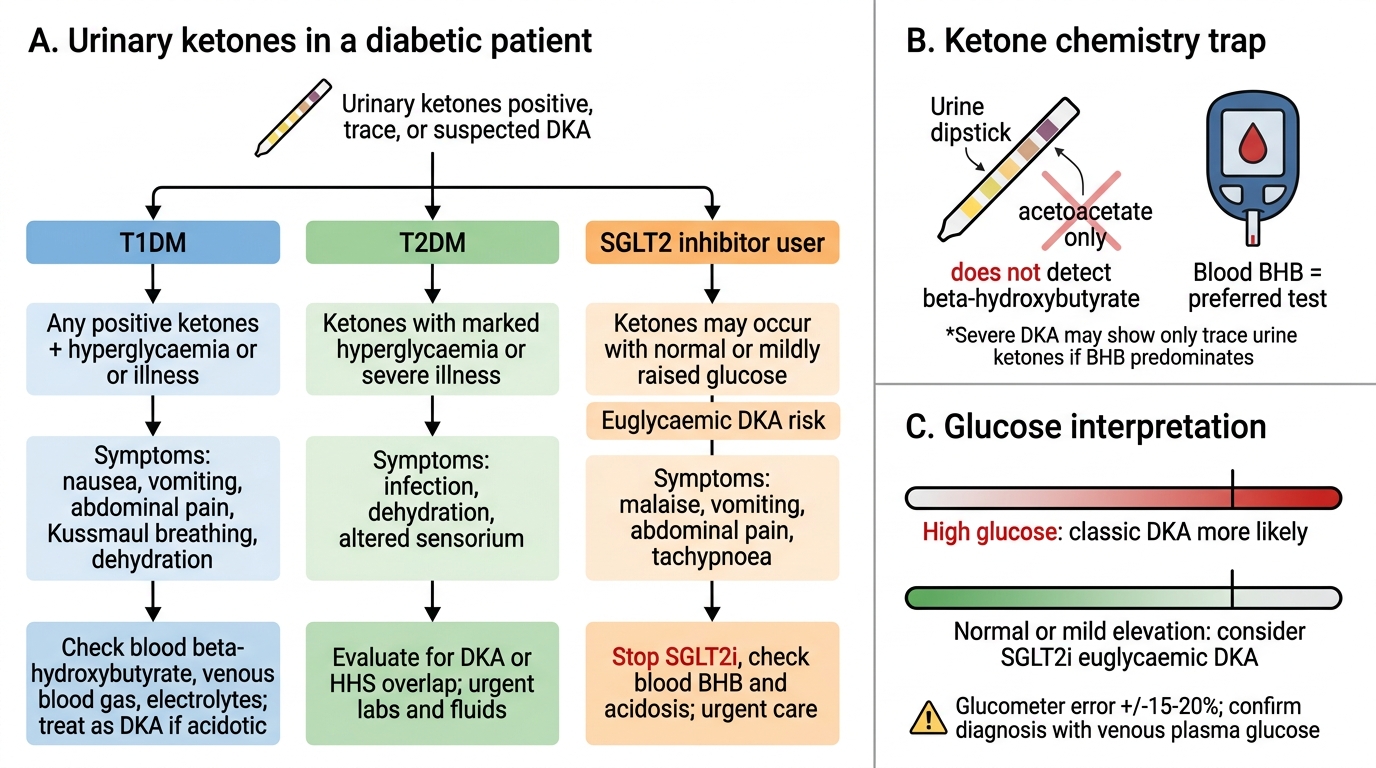
Interpreting Urinary Ketones in Diabetes
CLINICAL PEARL
Three diagnostic testing traps that cause clinical errors:
- HbA1c is not reliable in all patients. Never use it as the sole diagnostic test in patients with haemoglobinopathies (sickle cell, thalassaemia), haemolytic anaemia, iron deficiency, or recent blood transfusion. Iron deficiency can falsely elevate HbA1c by up to 1–2 percentage points — treating iron deficiency alone may dramatically lower an apparently high HbA1c.
- The urine ketone dipstick does not detect beta-hydroxybutyrate. In severe or prolonged DKA, the predominant ketone is BHB, which the dipstick misses. A patient can be in severe DKA with only trace urinary ketones if BHB predominates. Blood BHB measurement (target: <0.6 mmol/L for DKA resolution) is the gold standard for monitoring.
- Glucometer results are NOT diagnostic. The permissible error for glucometers is ±15–20% of the true glucose. A glucometer reading of 128 mg/dL could represent a true glucose of 109–147 mg/dL. Always use laboratory venous plasma glucose (or HbA1c) for the formal diagnosis of diabetes.