Page 2 of 23
IM11.1-6 | Diabetes Foundations — SDL Guide (Part 2)
Microvascular and Macrovascular Complications
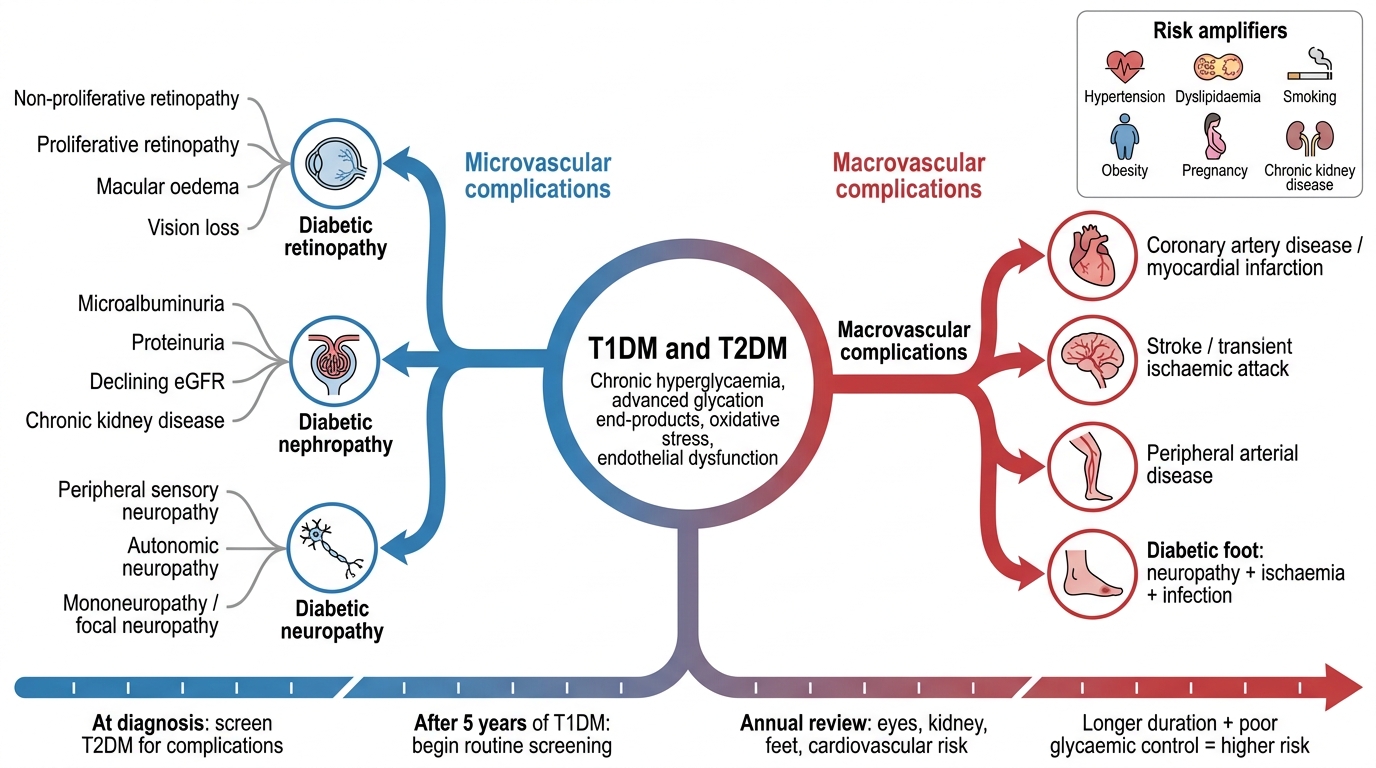
The complications of diabetes mellitus are the principal source of morbidity and mortality and are classified as microvascular (affecting small vessels: retina, kidney, peripheral nerves) and macrovascular (affecting large vessels: coronary arteries, cerebral arteries, peripheral arteries). Both categories arise from the toxic effects of chronic hyperglycaemia on the vascular endothelium and are accelerated by hypertension, dyslipidaemia, smoking, and obesity. The Diabetes Control and Complications Trial (DCCT) for T1DM and the UK Prospective Diabetes Study (UKPDS) for T2DM definitively established that intensive glycaemic control reduces the incidence and progression of microvascular complications by 35–76%; the benefit for macrovascular disease is more modest and emerges over longer timeframes.
The pathogenic mechanisms underlying diabetic vascular disease operate through four principal biochemical pathways activated by intracellular hyperglycaemia, particularly in cells that cannot limit glucose uptake (endothelial cells, pericytes, mesangial cells, Schwann cells): (1) Polyol pathway activation — excess glucose is converted to sorbitol by aldose reductase, depleting NADPH and reducing glutathione, causing oxidative stress and osmotic cell damage; (2) Advanced glycation end products (AGEs) — glucose reacts non-enzymatically with proteins to form AGEs, which crosslink collagen (increasing basement membrane thickness), activate RAGE receptors (inducing inflammatory cytokine release), and quench nitric oxide (causing endothelial dysfunction); (3) Protein kinase C (PKC) activation — via diacylglycerol accumulation, leading to abnormal vascular permeability, angiogenesis (in retinopathy), and contractility; (4) Hexosamine pathway — excess glucose enters the hexosamine pathway, producing reactive intermediates that impair signalling and increase TGF-β, contributing to fibrosis (in nephropathy).
Diabetic Retinopathy (DR): The most common cause of new blindness in working-age adults in developed countries. The temporal sequence is: background/non-proliferative DR (NPDR) → pre-proliferative DR → proliferative DR (PDR). NPDR features include microaneurysms (earliest sign), dot-blot haemorrhages, hard exudates (lipid deposits from leaking vessels), and cotton-wool spots (nerve-fibre layer infarcts, marking pre-proliferative stage). The hallmark of PDR is neovascularisation — new fragile vessels grow in response to ischaemia-driven VEGF release; these new vessels can bleed (vitreous haemorrhage), causing sudden visual loss, and contract to cause traction retinal detachment. Macular oedema (any grade) can impair central vision independently.
Diabetic Nephropathy (DN): The leading cause of end-stage renal disease (ESRD) in India. The temporal sequence follows a predictable progression: glomerular hyperfiltration (early, asymptomatic, eGFR elevated) → microalbuminuria (30–300 mg/day or ACR 3–30 mg/mmol — the earliest clinical sign) → proteinuria/macroalbuminuria (>300 mg/day) → declining GFR → ESRD (eGFR <15 mL/min/1.73m²). The pathological correlate is Kimmelstiel-Wilson nodular glomerulosclerosis — the pathognomonic lesion of diabetic nephropathy on renal biopsy. All patients with diabetes should have annual urinary ACR (albumin:creatinine ratio) and eGFR monitoring.
Diabetic Neuropathy (DNP): The most prevalent complication overall, affecting up to 50% of people with diabetes of long duration. The distal symmetric sensorimotor peripheral polyneuropathy is the most common form — a length-dependent, 'stocking-and-glove' pattern loss of protective sensation beginning in the feet. This creates the substrate for the diabetic foot — painless ulceration, infection, and Charcot neuroarthropathy. Autonomic neuropathy affects the cardiovascular system (resting tachycardia, orthostatic hypotension, loss of heart rate variability), gastrointestinal tract (gastroparesis, diarrhoea, constipation), genitourinary system (erectile dysfunction, neurogenic bladder), and sudomotor system (anhidrosis).
Macrovascular Complications: Diabetes confers a 2–4-fold increased risk of coronary artery disease (CAD), often presenting atypically or silently due to cardiac autonomic neuropathy. Risk of stroke and peripheral arterial disease (PAD) is similarly elevated. The combination of neuropathy, ischaemia, and impaired healing in the foot produces the diabetic foot syndrome, the leading cause of non-traumatic lower-limb amputation worldwide. Aggressive management of all cardiovascular risk factors — BP <130/80 mmHg, LDL-C <1.8 mmol/L (70 mg/dL) with statin therapy, antiplatelet agents in established CVD — is integral to diabetes management.
Complications of Diabetes Mellitus
Diabetic Emergencies: Overview and Recognition
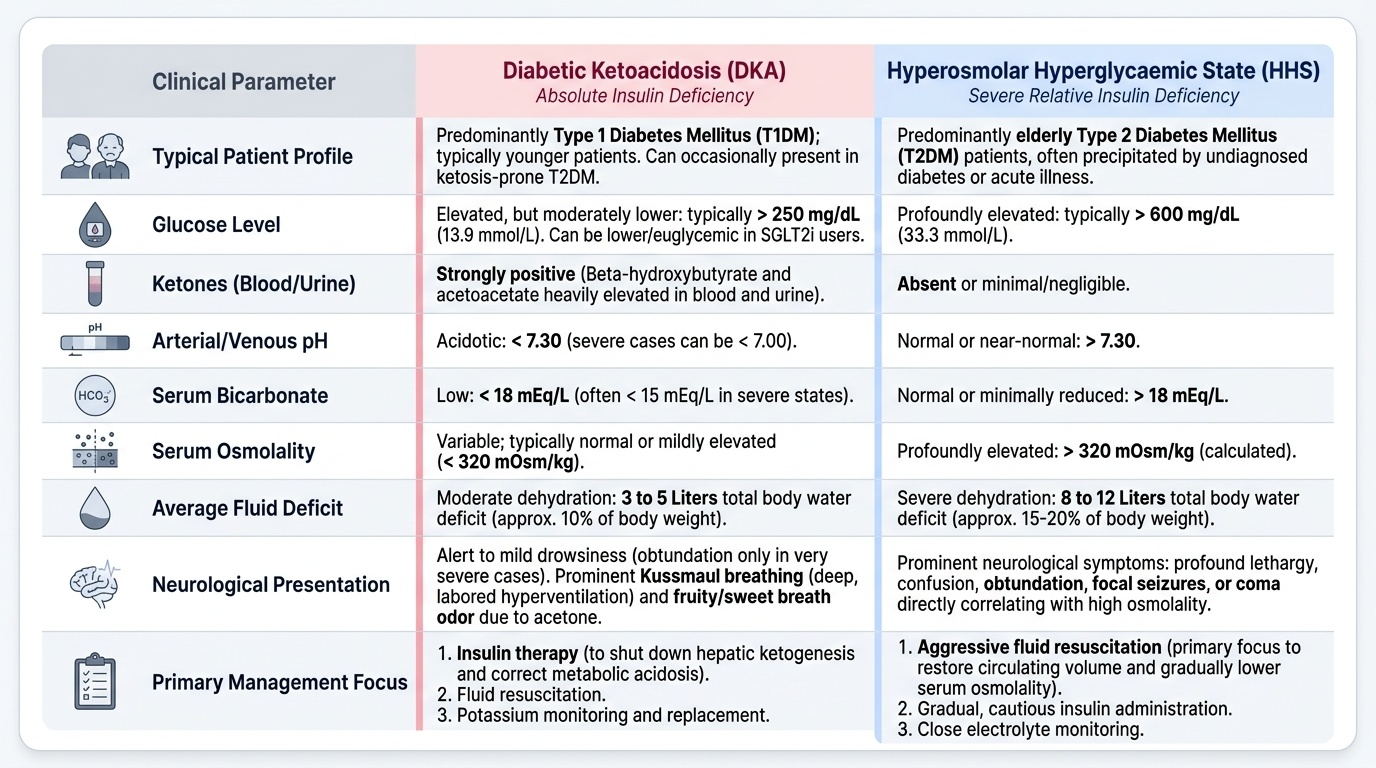
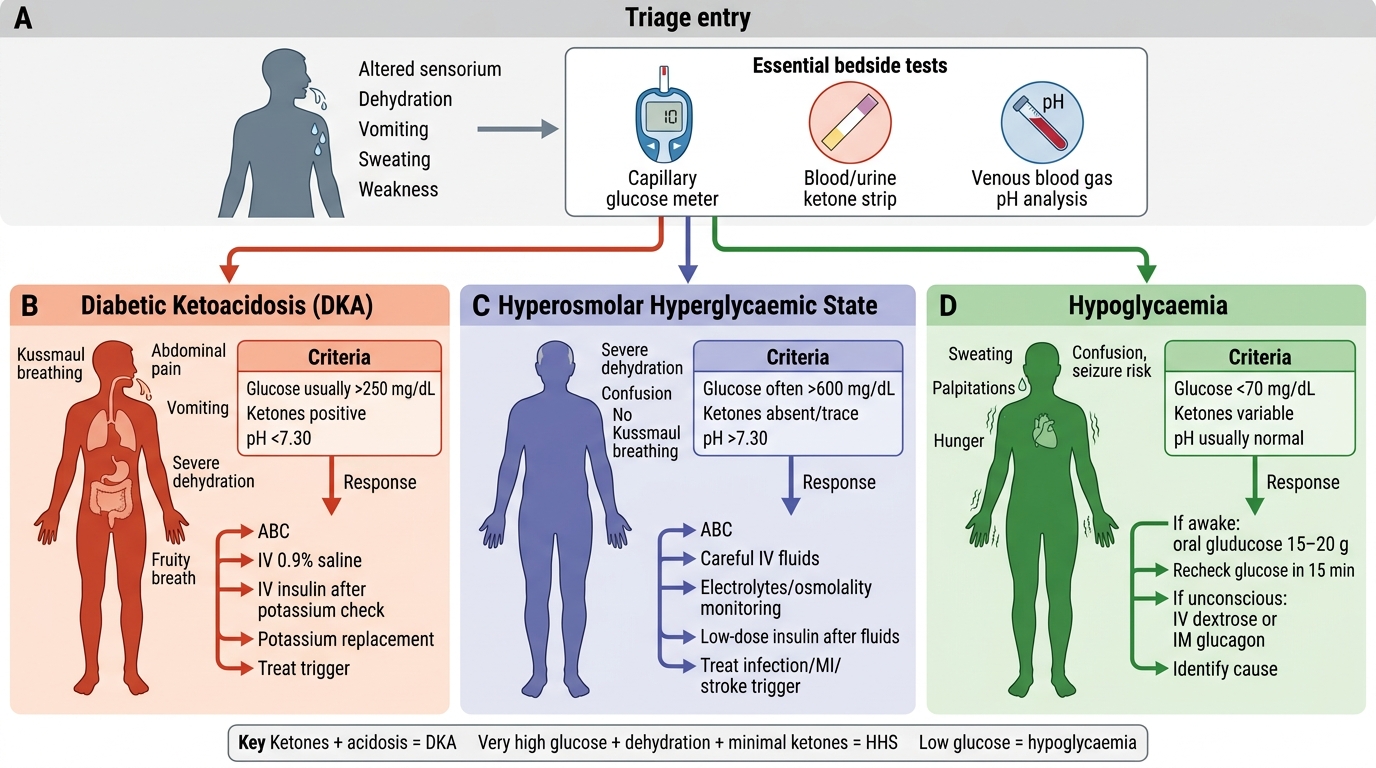
The three principal acute diabetic emergencies are diabetic ketoacidosis (DKA), hyperosmolar hyperglycaemic state (HHS), and hypoglycaemia. Each has a distinct pathophysiology, typical patient profile, and management approach, though they can occasionally coexist or overlap (euglycaemic DKA in SGLT2i users, or mixed DKA-HHS in elderly T1DM patients). Rapid recognition and structured management are lifesaving — mortality for untreated HHS approaches 20% and for severe hypoglycaemia can be equivalent. While the full management of each emergency is covered in the dedicated SDL (IM11.14–11.15, 11.22–11.24), this section provides the pathogenic framework and clinical recognition skills essential to the Diabetes Foundations competency set (IM11.6).
Provided image
Diabetic Ketoacidosis (DKA) occurs predominantly in T1DM (and occasionally in T2DM, especially LADA or ketosis-prone variants). The precipitating factors include infection (pneumonia, urinary tract infection — the commonest precipitants), missed insulin doses, new-onset T1DM, surgery, trauma, myocardial infarction, pancreatitis, and certain drugs (SGLT2 inhibitors can cause normoglycaemic DKA). The pathophysiology stems from absolute insulin deficiency combined with counter-regulatory hormone excess (glucagon, cortisol, adrenaline): hepatic ketogenesis (acetoacetate and beta-hydroxybutyrate production from unrestrained FFA oxidation) overwhelms peripheral ketone utilisation, causing an increased anion gap metabolic acidosis (pH <7.3, bicarbonate <18 mEq/L). The clinical triad is: hyperglycaemia (usually >250 mg/dL but occasionally lower), ketonuria/ketonaemia, and metabolic acidosis. Clinically, patients present with nausea and vomiting, abdominal pain (especially in children), Kussmaul breathing (deep, laboured breathing compensating for metabolic acidosis), and the sweet/fruity odour of acetone on the breath. Progressive dehydration (total body water deficit often 3–5 L) leads to obtundation and coma in severe DKA.
Hyperosmolar Hyperglycaemic State (HHS), previously called HONK (hyperosmolar non-ketotic coma), occurs predominantly in elderly T2DM patients, often as the presenting event of undiagnosed diabetes. HHS involves profound hyperglycaemia (typically >600 mg/dL), extreme hyperosmolality (calculated serum osmolality >320 mOsm/kg), and severe dehydration (total body water deficit up to 10–12 L), but with minimal or absent ketosis because residual insulin is sufficient to suppress hepatic ketogenesis while being inadequate to control hepatic glucose output. Neurological features — confusion, seizures, focal deficits, coma — dominate the clinical picture due to hyperosmolality-induced cerebral dehydration. The absence of acidosis means patients may be deceptively stable-appearing initially.
Hypoglycaemia — blood glucose typically <70 mg/dL — is the most common acute complication in treated diabetes (especially in insulin-dependent patients and those on sulphonylureas). Counter-regulatory symptoms (sweating, tremor, palpitations, pallor — mediated by adrenaline release at ~60–65 mg/dL) precede neuroglycopenic symptoms (confusion, slurred speech, focal deficits, seizures, coma — at glucose <50 mg/dL). Unawareness of hypoglycaemia (hypoglycaemia unawareness) — loss of the adrenergic warning symptoms — develops in some patients with longstanding T1DM after repeated hypoglycaemic episodes, dramatically increasing the risk of severe events.
SELF-CHECK
A 55-year-old man with known T2DM is found confused at home. Blood glucose is 680 mg/dL. Serum osmolality is calculated at 338 mOsm/kg. Urinary ketones are trace-negative. Arterial pH is 7.36. Which is the MOST ACCURATE characterisation of his condition?
A. Diabetic ketoacidosis (DKA) with minimal ketonaemia
B. Hyperosmolar hyperglycaemic state (HHS) without significant ketosis
C. Lactic acidosis complicating metformin toxicity
D. Mixed DKA and HHS requiring both insulin and bicarbonate
Reveal Answer
Answer: B. Hyperosmolar hyperglycaemic state (HHS) without significant ketosis
This is the classic presentation of hyperosmolar hyperglycaemic state (HHS): elderly T2DM, extreme hyperglycaemia (>600 mg/dL), elevated osmolality (>320 mOsm/kg), confusion (neurological feature from hyperosmolality), and absence of significant ketosis and acidosis (pH 7.36 is normal). The residual insulin in T2DM suppresses hepatic ketogenesis. DKA requires pH <7.3 and significant ketonaemia/ketonuria. Lactic acidosis would cause a high anion gap metabolic acidosis. Bicarbonate is not routinely indicated in HHS.
Self-Assessment: Integrating Diabetes Foundations
At this point you have a comprehensive grasp of the pathogenic mechanisms, epidemiological burden, and complication profile of diabetes mellitus. The scenarios below are designed to test the integration of this knowledge at the KH (applied knowledge) level required by the NMC IM11.1–11.6 competencies. Work through each scenario before reading the analysis; focus on using pathogenetic reasoning rather than pure memorisation.
Scenario A: A 35-year-old lean Indian man presents with a 6-month history of modest polyuria and fasting glucose of 118 mg/dL. His father and paternal grandfather both had diabetes diagnosed before age 40. He has no other metabolic risk factors and a BMI of 22 kg/m². An OGTT at 2 hours gives 158 mg/dL and his HbA1c is 5.9%. What diagnosis best fits, and what is the most appropriate next investigation?
Analysis: Fasting 118 mg/dL (IFG range 100–125), 2-hour 158 mg/dL (IGT range 140–199), HbA1c 5.9% (prediabetes range 5.7–6.4%). This is a pre-diabetic state. However, the strong family history with autosomal-dominant pattern (multiple generations, early onset, lean phenotype) raises the possibility of MODY (Maturity-Onset Diabetes of the Young). The most appropriate next step is genetic testing for MODY mutations (GCK-MODY or HNF1A-MODY are the most common). MODY has important management implications — GCK-MODY may not require pharmacological treatment, while HNF1A-MODY is exquisitely sensitive to sulphonylureas.
Scenario B: Ravi, 48-year-old T2DM for 8 years on metformin and glipizide, presents for his annual review. His HbA1c is 8.1%. On fundoscopy, there are bilateral microaneurysms and a few hard exudates, but no neovascularisation. His ACR is 52 mg/mmol and eGFR is 62 mL/min/1.73m². Peripheral sensation is diminished bilaterally in a stocking distribution. What stage of each complication does he have, and what are the immediate management priorities?
Analysis: Non-proliferative diabetic retinopathy (NPDR) — microaneurysms, hard exudates, no new vessels. Diabetic nephropathy stage with macroalbuminuria (ACR 52 > 30 mg/mmol threshold) and mildly reduced eGFR (CKD G3a by KDIGO). Distal symmetric diabetic peripheral neuropathy. Management priorities: intensify glycaemic control (target HbA1c ~7%), start/optimise RAAS blockade (ACE inhibitor or ARB for nephroprotection), refer to ophthalmology for retinal laser consideration, perform detailed neuropathic foot assessment, and add SGLT2 inhibitor (proven renoprotective benefit regardless of baseline glycaemic control).
Scenario C: A 16-year-old girl presents to the emergency department after being found unconscious. She is known to have T1DM for 3 years and was recently started on continuous subcutaneous insulin infusion (insulin pump). Blood glucose at the scene was 24 mg/dL. On examination she is unresponsive with diaphoresis and tachycardia. IV access is obtained. What is the immediate management?
Analysis: Severe hypoglycaemia with neuroglycopenia (unconscious). Immediate treatment: IV dextrose 25–50 mL of 50% dextrose (or 2 mL/kg of 10% dextrose in children), repeat blood glucose in 10–15 minutes and repeat if still low. If IV access not available: intramuscular or intranasal glucagon. Once conscious, give long-acting carbohydrate. Investigate the cause — pump malfunction, missed meal, exercise, alcohol, and review recent insulin dose history.
⚑ AI image — pending faculty review (auto-QA score 8/10; best of 3 attempts)
Acute Diabetic Emergencies: Bedside Recognition and Response
CLINICAL PEARL
The diagnostic criteria for diabetes mellitus require precision — memorise these exact numbers and their tests:
- Fasting plasma glucose ≥126 mg/dL (fasting = no caloric intake for ≥8 hours)
- 2-hour plasma glucose ≥200 mg/dL during a standard 75 g oral glucose tolerance test (OGTT)
- HbA1c ≥6.5% (using a NGSP/IFCC-certified method)
- Random plasma glucose ≥200 mg/dL with classic symptoms of hyperglycaemia (polyuria, polydipsia, unexplained weight loss)
In the absence of unequivocal hyperglycaemia with symptoms, any single positive result must be confirmed by a REPEAT test on a different day. HbA1c is unreliable in conditions that affect red cell survival (haemolytic anaemia, haemoglobinopathies, iron deficiency) — use glucose-based criteria instead.
A key India-specific trap: the 'thin-fat Indian' phenotype means Indians develop T2DM at lower BMI than Europeans. Use India-specific BMI thresholds (overweight ≥23, obese ≥25 kg/m²) and screen all adults ≥45 years (or ≥35 with risk factors) with fasting plasma glucose annually.