Page 10 of 23
IM11.{16-18,21} | Diabetes Pharmacologic Management — SDL Guide
Learning Objectives
- Describe the pharmacologic classes for diabetes including indications, contraindications, adverse reactions, and interactions
- Outline a stepwise therapeutic approach to T2DM based on presentation, severity, and complications in a cost-effective manner
- Describe drugs used in the prevention and treatment of target-organ damage in T2DM including neuropathy, nephropathy, retinopathy, hypertension, dyslipidaemia, and cardiovascular disease
- Recognise the importance of patient preference in selecting diabetes therapy
INSTRUCTIONS
Pharmacological management of diabetes is one of the most therapeutically complex and rapidly evolving areas in clinical medicine. This module covers the full class-by-class pharmacology of diabetes drugs, a stepwise T2DM treatment algorithm, organ-protective therapies, and the principles of patient-centred prescribing.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 406 — Pharmacological Treatment of Type 2 Diabetes (textbook)
- API Textbook of Medicine, 10th ed., Ch. 51 — Diabetes Mellitus: Management (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed., Ch. 21 — Treatment of Type 2 Diabetes (textbook)
- American Diabetes Association — Standards of Medical Care 2024, Section 9: Pharmacologic Approaches (guideline)
- ADA/EASD Consensus Report on Management of Hyperglycaemia in T2DM, 2022 (guideline)
Version 1.0 | NMC CBUC 2024
CLINICAL SCENARIO
Rajan, 52-year-old accountant, has been on metformin 1000 mg twice daily for 3 years. His HbA1c has drifted from 7.2% to 8.6% despite good dietary compliance. He has a BMI of 29 kg/m², eGFR 58 mL/min/1.73m², and urine ACR 42 mg/mmol. He has no history of cardiovascular events but his LDL-C is 3.4 mmol/L and his BP is 148/92. He tells you he is worried about 'taking too many tablets' and is 'not keen on injections.' Now you must prescribe. Your choice of second-line agent is not arbitrary — there is an agent that simultaneously improves glycaemia, reduces his cardiovascular risk, slows his nephropathy progression, and does not cause hypoglycaemia. There is also an agent that would worsen his kidney function if you ignore his eGFR. There are two agents that require injections and one that would cost him ₹8,000 a month. Every pharmacological decision in diabetes has these dimensions: efficacy, safety, organ protection, cost, and patient acceptability. Learning to navigate all five is the goal of this module.
WHY THIS MATTERS
The pharmacological management of T2DM is among the most high-yield clinical topics in final-year medicine and postgraduate entrance examinations. In routine clinical practice, you will prescribe diabetes medications on your first day as an intern — the wrong drug at the wrong eGFR can cause lactic acidosis (metformin in severe CKD), the wrong dose of insulin can cause fatal hypoglycaemia, and the failure to prescribe a cardioprotective agent in a diabetic patient with CKD can hasten end-stage renal disease. The NMC competencies IM11.16–11.18 and IM11.21 address pharmacology (IM11.16), T2DM treatment algorithms (IM11.17), organ-protective drugs (IM11.18), and patient-centred prescribing (IM11.21) — together covering the full prescribing lifecycle from drug selection to patient counselling.
RECALL
Before proceeding, anchor your understanding in the two core pathophysiological defects of T2DM: insulin resistance (in muscle, liver, and adipose) and progressive beta-cell failure. Pharmacotherapy addresses one or both of these defects or compensates for them by augmenting insulin secretion, reducing glucose absorption, promoting glycosuria, or replacing the absent insulin. Recall also that HbA1c is the primary measure of long-term glycaemic control (target <7% or <53 mmol/mol for most patients; individualised for the elderly, those with hypoglycaemia risk, or advanced CKD). Recall the four classes where hypoglycaemia is a primary risk: insulin, sulphonylureas (SU), meglitinides (glinides), and insulin secretagogues — all other classes carry negligible intrinsic hypoglycaemia risk. The clinical distinction between classes that cause weight gain (insulin, SU, TZD) and those that are weight-neutral or weight-reducing (metformin, GLP-1 RA, SGLT2i, DPP-4i) is highly relevant to patient selection.
Clinical Presentation Prompting Pharmacotherapy in Diabetes
The decision to initiate or intensify pharmacotherapy in diabetes is always triggered by a clinical presentation — either at diagnosis, at a periodic review, or at the onset of a complication. Understanding the range of clinical presentations that precede and justify pharmacotherapy grounds the pharmacology that follows in clinical reality rather than abstract mechanism.
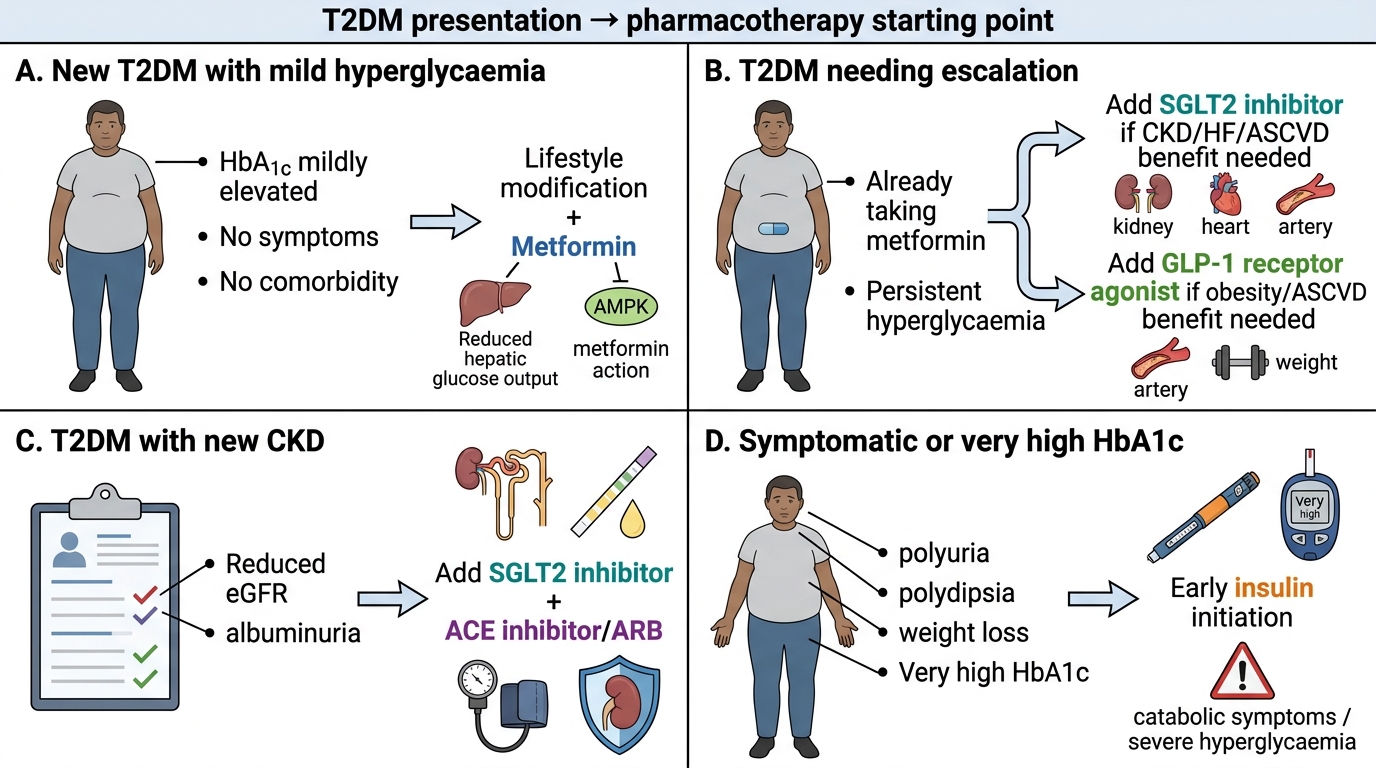
Presentation 1 — Newly Diagnosed T2DM with Mild-Moderate Hyperglycaemia:
The most common scenario in India: a 40–60 year-old overweight patient found to have fasting glucose ≥126 mg/dL or HbA1c ≥6.5% on opportunistic screening, often without symptoms. The clinical decision at this point involves: (a) confirming the diagnosis on repeat testing, (b) assessing for evidence of existing complications that change the drug selection (retinopathy, nephropathy, CVD, neuropathy — from the clinical evaluation), (c) staging the glycaemic severity (HbA1c 6.5–8% = lifestyle ± metformin; HbA1c 8–10% = dual therapy often appropriate from outset; HbA1c >10–11% or symptomatic = consider early insulin), and (d) identifying the comorbidity profile (established CVD, CKD, heart failure, obesity) that now directly drives second-line drug selection under ADA/EASD 2022 guidelines.
Presentation 2 — Established T2DM with Inadequate Glycaemic Control:
A patient already on metformin with HbA1c drifting above target (>7–7.5%) at review. This is Rajan's scenario from the hook. The presentation is not one of acute illness but of progressive therapeutic failure — reflecting the natural history of T2DM as beta-cell reserve declines over time. The pharmacological response is intensification: adding a second (and potentially third) agent, each chosen based on the comorbidity-driven algorithm covered in this module.
Presentation 3 — T2DM with a New Complication Diagnosis:
A patient on metformin and SU who is found at annual review to have urine ACR 65 mg/mmol (macroalbuminuria) and eGFR 52 for the first time. This represents a presentation that changes the pharmacological plan regardless of HbA1c — the complication now drives an SGLT2 inhibitor for renoprotection, an ACEi/ARB for blood pressure and nephroprotection, and potentially an intensified statin for dyslipidaemia. The pharmacological response to this presentation is organ-protective, not primarily glycaemic.
Presentation 4 — Newly Diagnosed T2DM with Very High Glucose or Symptoms:
A patient presenting with HbA1c >10%, polyuria, polydipsia, or weight loss — possibly with a near-DKA picture. The pharmacological plan here often involves early insulin (basal or basal-bolus), sometimes temporarily, to rapidly reduce glucotoxicity and relieve symptoms before transitioning to oral agents once glycaemia is controlled. This presentation also requires ruling out T1DM or LADA (latent autoimmune diabetes in adults) before committing to a pure T2DM regimen.
In all four presentations, the clinical context dictates not just which drug class to choose, but what the therapeutic goal is — HbA1c reduction alone, organ protection, symptom relief, or a combination. The pharmacology sections that follow are organised to serve these clinical goals.
T2DM Clinical Presentations and Starting Pharmacotherapy
Drug Classes for Diabetes: Mechanisms, Indications, and Adverse Effects
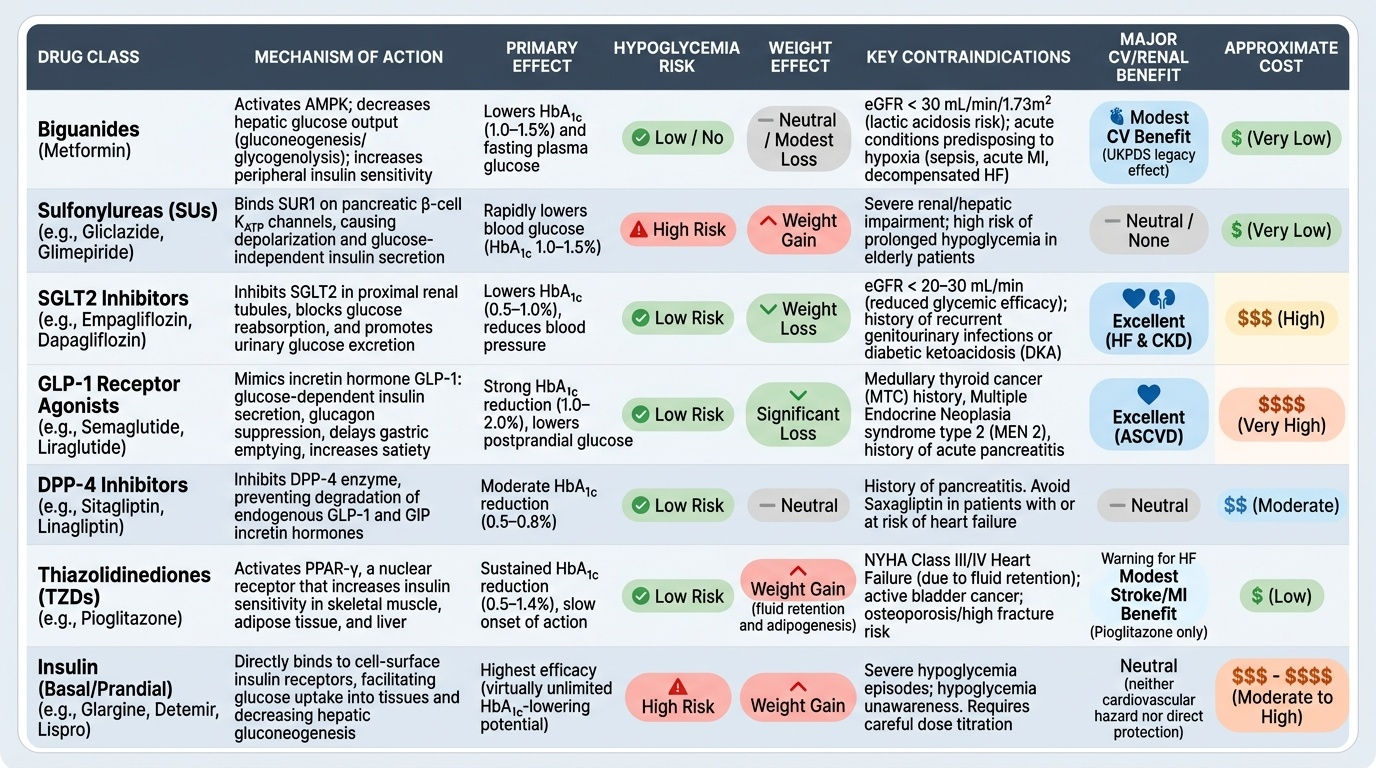
Antidiabetic drugs are classified by their mechanism of action. Understanding the mechanism is the key to understanding the indications, contraindications, and adverse effects — all of which flow logically from mechanism rather than requiring rote memorisation.
Provided image
1. Biguanides — Metformin:
Metformin is the first-line pharmacological agent for T2DM in all major guidelines (ADA, EASD, API). It is a biguanide that acts primarily by reducing hepatic glucose output (gluconeogenesis and glycogenolysis) via activation of AMPK (AMP-activated protein kinase), secondarily by improving peripheral insulin sensitivity. It does NOT stimulate insulin secretion — therefore it does not cause hypoglycaemia as monotherapy. Additional benefits: modest weight reduction or weight neutrality, cardiovascular benefit (UKPDS legacy effect), and very low cost. Standard dose: 500–1000 mg twice daily with meals.
Contraindications/cautions: The most important is renal impairment: metformin is renally cleared and accumulates in CKD, predisposing to lactic acidosis — a rare but serious adverse effect. Metformin should not be started if eGFR <30 mL/min/1.73m²; withhold temporarily if eGFR 30–45; use with caution and reduce dose if eGFR 45–60. Withhold before iodinated contrast procedures and in conditions causing tissue hypoxia (sepsis, acute MI, hepatic failure) because hypoxia independently impairs lactate clearance. Common adverse effects: GI symptoms (nausea, diarrhoea, metallic taste) — minimised by slow dose titration and taking with food. Long-term use can cause vitamin B12 deficiency (monitor annually).
2. Sulphonylureas (SU):
Sulphonylureas — glibenclamide (glyburide), glipizide, gliclazide, glimepiride — act by binding to SUR1 subunits of ATP-sensitive K+ channels in pancreatic beta cells, causing depolarisation and insulin secretion in a glucose-independent manner. This mechanism explains their most important adverse effect: hypoglycaemia (insulin is secreted regardless of blood glucose level). Risk is highest with the long-acting agents glibenclamide (avoid in elderly and renal impairment) and lower with gliclazide and glimepiride, which are preferred. Weight gain is common (increased insulin levels promote anorexia suppression and lipogenesis). Cost is very low — important for resource-limited settings.
Contraindications: Renal impairment (especially glibenclamide — active metabolites accumulate); hepatic impairment; allergy to sulphonamides (cross-reactivity). Interactions: NSAIDs, warfarin, fluconazole, and alcohol potentiate SU hypoglycaemia.
3. Thiazolidinediones (TZDs) — Pioglitazone:
Pioglitazone activates PPARγ (peroxisome proliferator-activated receptor gamma) in adipose tissue, liver, and muscle, improving insulin sensitivity by redistributing fat from visceral to subcutaneous depots and improving intracellular insulin signalling. It does not cause hypoglycaemia. Advantages: durable glycaemic control, reduction in NASH/fatty liver, possible cardiovascular benefit (PROactive trial: reduced stroke recurrence).
Adverse effects: Fluid retention and oedema (contraindicated in heart failure NYHA class III/IV); weight gain; increased risk of bladder cancer with prolonged use (avoid if active bladder cancer or haematuria); increased fracture risk in postmenopausal women (osteoclast activation). Use with caution in heart failure.
4. DPP-4 Inhibitors (Gliptins) — Sitagliptin, Vildagliptin, Saxagliptin, Alogliptin:
Dipeptidyl peptidase-4 (DPP-4) inhibitors prevent the degradation of GLP-1 (glucagon-like peptide-1) and GIP (incretin hormones), thereby potentiating their glucose-lowering effects: increased glucose-stimulated insulin secretion and reduced glucagon. Because the action is glucose-dependent, hypoglycaemia risk is very low. Weight-neutral. Well tolerated — main adverse effect is nasopharyngitis and upper respiratory tract infections (immunological mechanism). Saxagliptin is associated with increased hospitalisation for heart failure (SAVOR-TIMI trial — avoid in high heart failure risk). Dose adjustment required in renal impairment (sitagliptin dose halved at eGFR <45; linagliptin requires no dose adjustment even in severe CKD, making it the preferred gliptin in renal failure).
5. GLP-1 Receptor Agonists — Liraglutide, Semaglutide, Dulaglutide, Exenatide:
GLP-1 receptor agonists mimic the action of endogenous GLP-1: glucose-dependent insulin secretion, glucagon suppression, delayed gastric emptying (reducing postprandial glucose), and satiety signalling (leading to substantial weight loss). They are injectable (subcutaneous), except oral semaglutide. Their cardiovascular benefits are proven in multiple trials (LEADER for liraglutide, SUSTAIN-6 and PIONEER-6 for semaglutide): reduced major adverse cardiovascular events (MACE) in patients with established cardiovascular disease. This makes them the preferred second- or third-line agent after metformin in T2DM patients with established CVD (in conjunction with or instead of SGLT2i).
Adverse effects: Nausea and vomiting (most common, particularly on initiation — dose escalation protocol needed); pancreatitis (rare but contraindicated if history of pancreatitis); contraindicated in personal/family history of medullary thyroid carcinoma (MTC) or MEN-2 (based on rodent data of thyroid C-cell tumours). Renal considerations: liraglutide and semaglutide can be used down to eGFR 15; exenatide should not be used if eGFR <30.
6. SGLT2 Inhibitors — Empagliflozin, Dapagliflozin, Canagliflozin:
Sodium-glucose cotransporter-2 (SGLT2) inhibitors block glucose reabsorption in the proximal convoluted tubule of the kidney, causing glycosuria of approximately 60–80 g of glucose per day regardless of plasma glucose level. This lowers blood glucose, reduces blood pressure (osmotic diuresis), promotes weight loss (caloric loss), and reduces cardiac preload and afterload. Cardiovascular and renal benefits are now proven across multiple RCTs: EMPA-REG OUTCOME (empagliflozin — 38% relative risk reduction in CV death), CREDENCE (canagliflozin — significant reduction in renal endpoints), DAPA-CKD (dapagliflozin — renal protection in CKD regardless of diabetes status).
Contraindications and cautions: Renal impairment — SGLT2i require adequate renal function for their glycosuric effect; empagliflozin and dapagliflozin can be started if eGFR ≥20 for their cardio/renoprotective effects (even though the glycaemic lowering is attenuated at lower eGFR); canagliflozin can be used down to eGFR ≥30 for renal protection. Do NOT use in T1DM (risk of euglycaemic DKA). Key adverse effects: genital mycotic infections (Candida — particularly in women), urinary tract infections, euglycaemic DKA (rare, higher risk with intercurrent illness/surgery/fasting), Fournier's gangrene (rare necrotising fasciitis of perineum — stop if suspected), lower limb amputations (canagliflozin specifically — slightly increased risk).
7. Insulin:
Insulin is discussed comprehensively in the Diabetes Patient Skills module (insulin technique) and the Diabetic Emergencies module (emergency dosing). From a pharmacology perspective: insulin types are classified by onset and duration — rapid-acting (lispro, aspart, glulisine — onset 15 min, peak 1–2h, duration 3–5h), short-acting (regular/soluble insulin — onset 30 min, duration 6–8h), intermediate-acting (NPH/isophane — onset 1–2h, duration 12–18h), long-acting basal (glargine, detemir, degludec — onset 1–4h, duration 20–42h, no pronounced peak). Hypoglycaemia and weight gain are universal adverse effects of insulin therapy. In T2DM, basal insulin (glargine or NPH) is typically added to oral agents when HbA1c remains above target.
Stepwise T2DM Treatment Algorithm
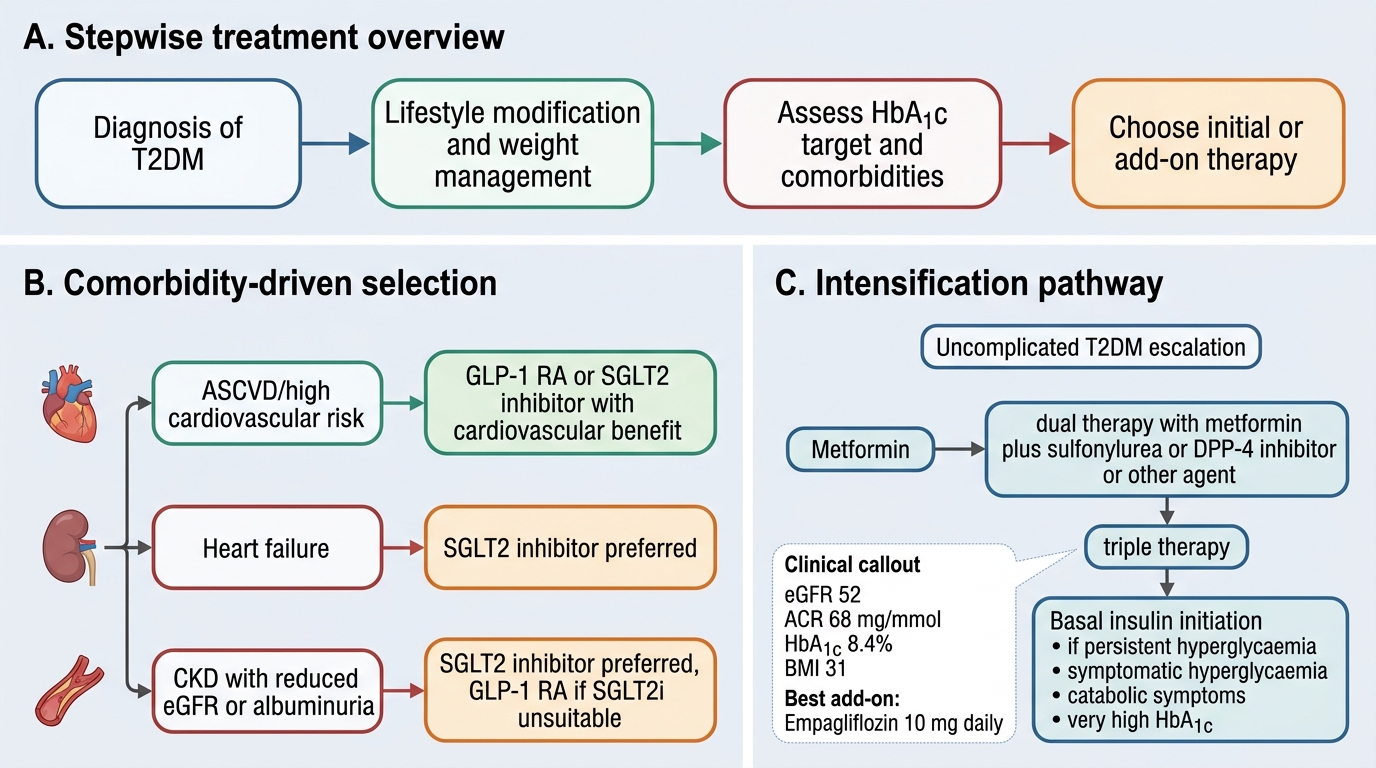
The stepwise treatment of T2DM is no longer a purely HbA1c-driven ladder. Modern guidelines (ADA 2024, ADA/EASD Consensus 2022) incorporate cardiovascular risk, renal risk, weight, hypoglycaemia risk, cost, and patient preference as co-equal determinants of drug selection alongside glycaemic control. This represents a fundamental shift from the older 'treat-to-target HbA1c' model to a 'treat-to-benefit' model where organ-protective outcomes take precedence.
Step 1 — Lifestyle Modification (Always the Foundation):
Medical nutrition therapy (reduce total carbohydrate, increase fibre, caloric restriction for weight loss) combined with aerobic exercise (at least 150 minutes/week of moderate intensity) and smoking cessation. For newly diagnosed T2DM with mild hyperglycaemia (HbA1c <8%), lifestyle alone for 3 months is a reasonable initial strategy before pharmacotherapy. Weight loss of 5–10% improves glycaemia, lipids, and BP in overweight patients.
Step 2 — First-line Pharmacotherapy: Metformin + Comorbidity-Driven Co-prescription:
Metformin remains the first-line pharmacological agent for most patients (unless contraindicated — eGFR <30, or intolerant). However, the ADA/EASD 2022 consensus now recommends that if a patient has established ASCVD (atherosclerotic cardiovascular disease), CKD, or heart failure at diagnosis, an SGLT2 inhibitor or GLP-1 RA with proven cardiovascular/renal benefit should be initiated concurrently with or even instead of metformin, as these organ-protective benefits are independent of baseline HbA1c and are not achieved by metformin.
Decision matrix for first-line or early add-on agent:
- Established ASCVD: GLP-1 RA (liraglutide, semaglutide) or SGLT2i (empagliflozin, canagliflozin) for MACE reduction
- CKD (eGFR 20–60, ACR >30 mg/mmol): SGLT2i for renoprotection (primary choice); GLP-1 RA if SGLT2i not tolerated
- Heart failure (HFrEF or HFpEF): SGLT2i (proven hospitalisation reduction in EMPEROR-Reduced, DAPA-HF)
- Need for weight loss: GLP-1 RA (semaglutide — up to 15–17% body weight reduction in STEP trials) or SGLT2i
- High hypoglycaemia risk: Avoid SU, meglitinides; prefer DPP-4i, GLP-1 RA, SGLT2i
- Cost constraints: Metformin + SU (gliclazide or glimepiride) is the most cost-effective two-drug regimen
Step 3 — Intensification When HbA1c Remains Above Target:
If HbA1c remains above the individualised target after 3 months of first-line therapy, a second agent is added. The choice follows the same comorbidity-driven matrix above. Adding two agents (triple therapy) may be needed for HbA1c >9%. Key combinations:
- Metformin + SGLT2i: complementary mechanisms (hepatic glucose reduction + renal glycosuria + weight loss + CV/renal protection)
- Metformin + GLP-1 RA: powerful combination for high HbA1c with obesity or CVD history
- Metformin + DPP-4i: well tolerated, weight neutral, low hypoglycaemia risk — good in elderly patients
- Metformin + SU: most affordable; hypoglycaemia risk (especially glibenclamide — avoid); prefer gliclazide/glimepiride
Step 4 — Insulin Initiation in T2DM:
Insulin is added (not necessarily permanently) when:
- HbA1c very high at diagnosis (>10–11%), symptomatic hyperglycaemia, or ketonuria at presentation
- Failure of dual/triple oral therapy (progressive beta-cell exhaustion)
- Major illness, surgery, or pregnancy
In T2DM, basal insulin (bedtime NPH or glargine/degludec) added to metformin is the standard approach. The starting dose is 10 units (or 0.1–0.2 units/kg) at bedtime, titrated upward by 2 units every 3 days based on the fasting glucose target (target fasting glucose 80–130 mg/dL). Premixed insulin (e.g., 30/70 — 30% regular + 70% NPH, or 25/75 biphasic aspart) twice daily before breakfast and dinner is a convenient option for T2DM patients who prefer fewer injections but have both fasting and postprandial hyperglycaemia.
Cost-effectiveness considerations in India:
The monthly drug cost range in India (approximate): metformin = ₹50–150; SU (gliclazide) = ₹100–200; DPP-4i = ₹800–1,500; SGLT2i = ₹1,500–3,000; GLP-1 RA = ₹6,000–15,000; insulin glargine = ₹1,800–3,500/pen. For patients with financial constraints, metformin + gliclazide remains a fully evidence-based, safe, and effective regimen. Patient adherence to a regimen they can afford is superior to non-adherence to a regimen they cannot.
Stepwise Treatment Algorithm for Type 2 Diabetes Mellitus
SELF-CHECK
A 58-year-old T2DM patient has HbA1c 8.4% on metformin 2 g/day. He has eGFR 52 mL/min/1.73m², urinary ACR 68 mg/mmol, no history of cardiovascular events, and no symptoms of heart failure. BMI is 31 kg/m². Which agent is the MOST appropriate add-on based on current guidelines?
A. Glibenclamide 5 mg once daily — effective and inexpensive
B. Sitagliptin 50 mg once daily (dose-adjusted for eGFR <60)
C. Empagliflozin 10 mg once daily — renal protection plus glycaemic benefit
D. Insulin glargine 10 units at bedtime — HbA1c is above target
Reveal Answer
Answer: C. Empagliflozin 10 mg once daily — renal protection plus glycaemic benefit
This patient has CKD (eGFR 52, ACR 68 — macroalbuminuria, CKD stage G3a A3). Current ADA/EASD guidelines recommend an SGLT2 inhibitor as the preferred add-on to metformin in T2DM with CKD, because of proven renoprotective effects (slowing eGFR decline and reducing proteinuria) independent of glycaemic lowering. Empagliflozin (and dapagliflozin) can be initiated at eGFR ≥20 for cardio/renoprotection even when the glycosuric effect is attenuated. Glibenclamide is dangerous in renal impairment (active metabolite accumulates → hypoglycaemia). Sitagliptin dose-adjusted is reasonable but lacks renoprotective benefit. Insulin is not indicated yet — oral intensification should be tried first.