Page 11 of 23
IM11.{16-18,21} | Diabetes Pharmacologic Management — SDL Guide (Part 2)
Drugs for Prevention and Treatment of Target-Organ Damage
Glycaemic control alone is insufficient to prevent cardiovascular and renal outcomes in T2DM. Multiple additional pharmacological interventions target the non-glycaemic risk factors and organ-specific pathways that drive complications. These drugs are an integral part of the T2DM management plan and their pharmacology is directly addressed by IM11.18.
1. ACE Inhibitors (ACEi) and ARBs — for Nephropathy and Hypertension:
Angiotensin-converting enzyme inhibitors (enalapril, ramipril, lisinopril) and angiotensin receptor blockers (losartan, valsartan, irbesartan, telmisartan) are first-line antihypertensives in diabetic patients for two reasons beyond BP control: (1) they preferentially dilate the efferent arteriole of the glomerulus, reducing intraglomerular pressure and proteinuria, slowing the progression of diabetic nephropathy; (2) they reduce cardiovascular mortality in high-risk patients (HOPE trial: ramipril reduced MI, stroke, and CV death by ~25% in high-risk patients including diabetics). Indicated in ALL patients with diabetes and microalbuminuria or macroalbuminuria regardless of blood pressure. ACEi + ARB combination is NOT recommended (ONTARGET trial: increased renal toxicity without added benefit). Adverse effects: ACEi — dry cough (bradykinin accumulation, 15–20% of Indians — switch to ARB); ARB — no cough; both — hyperkalaemia (avoid if K+ >5.5 mEq/L or eGFR <30 with caution), angioedema (rare with ACEi, very rare with ARB), teratogenicity (avoid in pregnancy).
2. Statins — for Dyslipidaemia and Cardiovascular Risk:
All T2DM patients aged ≥40 years (and younger with additional risk factors — smoking, hypertension, or CKD) should receive statin therapy regardless of baseline LDL-C level, because the cardiovascular risk reduction is primarily driven by LDL-C lowering from baseline, not by achieving a specific absolute level. High-intensity statin (atorvastatin 40–80 mg or rosuvastatin 20–40 mg) is appropriate for most patients with established CVD. Moderate-intensity statin (atorvastatin 10–20 mg, rosuvastatin 10 mg, simvastatin 20–40 mg) for primary prevention. LDL-C targets: <2.6 mmol/L (100 mg/dL) for most diabetic patients; <1.8 mmol/L (70 mg/dL) in those with established ASCVD. Adverse effects: myalgia (most common, dose-dependent), myopathy/rhabdomyolysis (rare but serious — monitor CK if symptomatic), hepatotoxicity (rare, not routinely monitored), new-onset T2DM (small increased risk, approximately 1 per 200 patients treated for 5 years — does not outweigh cardiovascular benefit). Drug interaction: simvastatin + gemfibrozil = high risk of rhabdomyolysis (avoid this combination; use fenofibrate with simvastatin if fibrate needed). Fibrates (fenofibrate) specifically target hypertriglyceridaemia (triglycerides >5.6 mmol/L) — important in diabetic dyslipidaemia.
3. Antiplatelet Therapy — Aspirin:
Low-dose aspirin (75–150 mg daily) is recommended for secondary prevention in all diabetic patients with established ASCVD (prior MI, stroke, PAD). For primary prevention, aspirin is no longer routinely recommended (ASCEND trial: the bleeding risk approximately equals the cardiovascular benefit in T2DM without prior CVD) — use only in patients with high cardiovascular risk after individual risk-benefit discussion. Clopidogrel is an alternative for aspirin-intolerant patients.
4. Treatments for Diabetic Peripheral Neuropathy:
There is no disease-modifying therapy — glycaemic control remains the primary approach to prevent progression. For symptomatic painful neuropathy: first-line agents are tricyclic antidepressants (amitriptyline 25–75 mg at night — effective, inexpensive, but anticholinergic adverse effects: dry mouth, urinary retention, constipation, sedation; avoid in elderly and urinary retention), duloxetine (SNRI, 60–120 mg/day — preferred first-line in many guidelines, with proven efficacy in diabetic neuropathic pain, fewer anticholinergic effects), and pregabalin or gabapentin (anticonvulsants targeting voltage-gated calcium channels in dorsal horn neurons; effective but sedating, weight gain, dizziness). Topical capsaicin 0.075% cream can be used for localised neuropathic pain as adjunctive therapy.
5. Treatment for Diabetic Retinopathy:
Intra-vitreal anti-VEGF agents (ranibizumab, bevacizumab, aflibercept) are now first-line treatment for centre-involving diabetic macular oedema (CI-DMO) and proliferative diabetic retinopathy with high-risk features, replacing the older exclusive reliance on laser. Panretinal photocoagulation (PRP) remains the standard for proliferative DR without macular involvement. The ophthalmologist manages these interventions; the physician's role is to ensure timely referral and optimal systemic control.
6. BP Target and Drug Choice in Diabetes:
The BP target in diabetes is <130/80 mmHg (ADA 2024). ACEi or ARB is first choice. If additional antihypertensive is needed: CCB (amlodipine, nifedipine — good first-choice add-on; no metabolic adverse effects) or thiazide diuretic (hydrochlorothiazide, chlorthalidone — effective, cheap, but cause mild hyperglycaemia and hypokalaemia). Beta-blockers can be used (if indicated for heart failure or angina) but mask hypoglycaemic symptoms — use cardioselective agents (bisoprolol, atenolol) and warn patients.
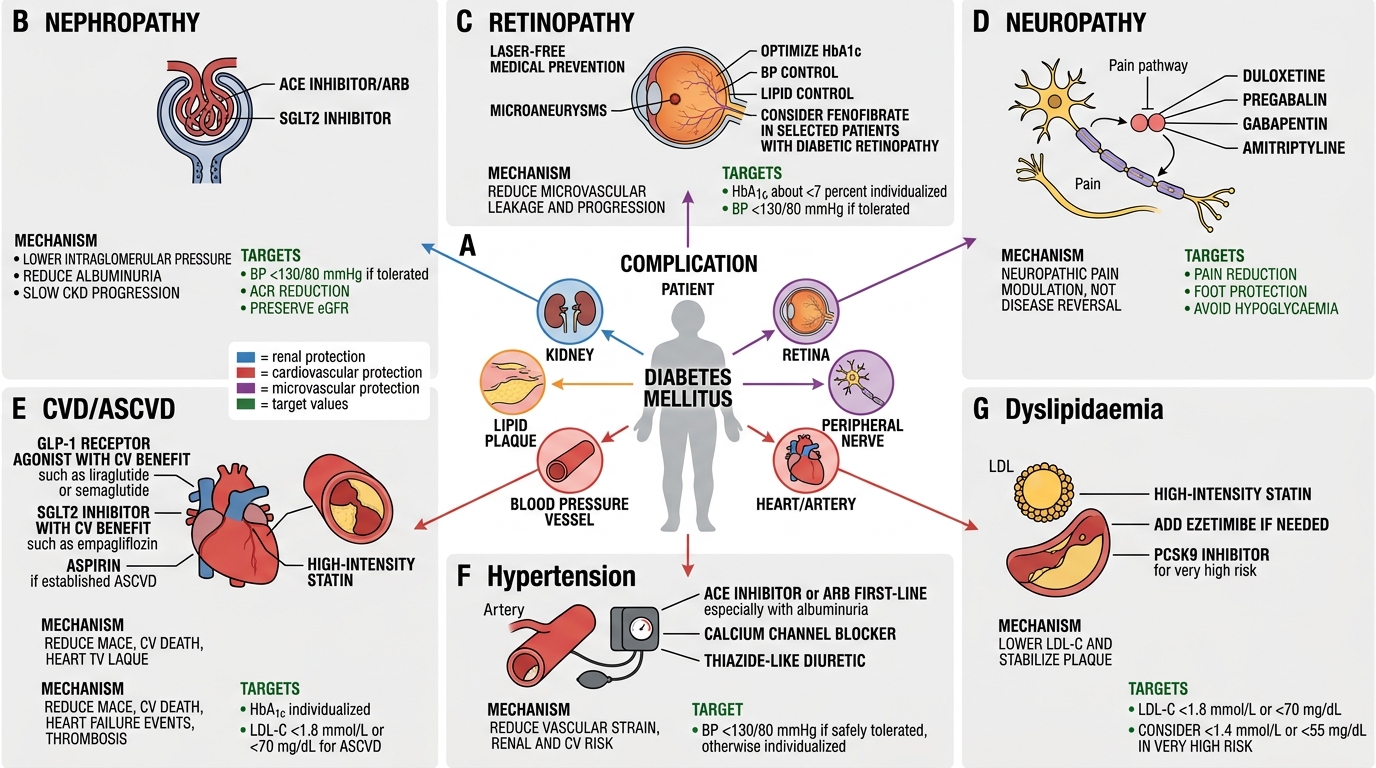
Diabetes Organ-Protection Drug Map
SELF-CHECK
A 65-year-old T2DM patient with established ASCVD (prior MI 2 years ago) is on metformin, aspirin, atorvastatin, and ramipril. His HbA1c is 7.8%, eGFR 55, no significant proteinuria (ACR 12 mg/mmol), BP 128/78, LDL-C 1.6 mmol/L. What is the MOST appropriate addition to intensify glycaemic management?
A. Glibenclamide 5 mg daily — effective and inexpensive second-line agent
B. Pioglitazone 30 mg daily — improves insulin sensitivity without hypoglycaemia
C. Liraglutide 0.6 mg subcutaneous daily — GLP-1 RA with proven CV mortality reduction
D. Insulin glargine 10 units at bedtime — most reliable glycaemic lowering
Reveal Answer
Answer: C. Liraglutide 0.6 mg subcutaneous daily — GLP-1 RA with proven CV mortality reduction
In a T2DM patient with established ASCVD (prior MI), ADA/EASD guidelines recommend a GLP-1 RA with proven cardiovascular benefit (liraglutide — LEADER trial: 13% relative risk reduction in CV death, non-fatal MI, and stroke) or an SGLT2i with proven MACE benefit as preferred add-on to metformin. There is no significant proteinuria to specifically drive SGLT2i choice over GLP-1 RA here. Glibenclamide carries hypoglycaemia risk and is not cardioprotective. Pioglitazone has some cardiovascular benefit (reduced stroke in PROactive) but causes fluid retention — less preferred in a post-MI patient. Insulin is reserved for later intensification when oral/injectable non-insulin agents fail.
Self-Assessment: Integrating Pharmacological Decision-Making
Putting the pharmacological framework together requires integrating drug mechanisms, clinical priorities, and patient preferences into individualised prescribing decisions. The scenarios below each represent a distinct clinical situation that tests a specific pharmacological decision point covered in this module. Work through each case before reading the analysis.
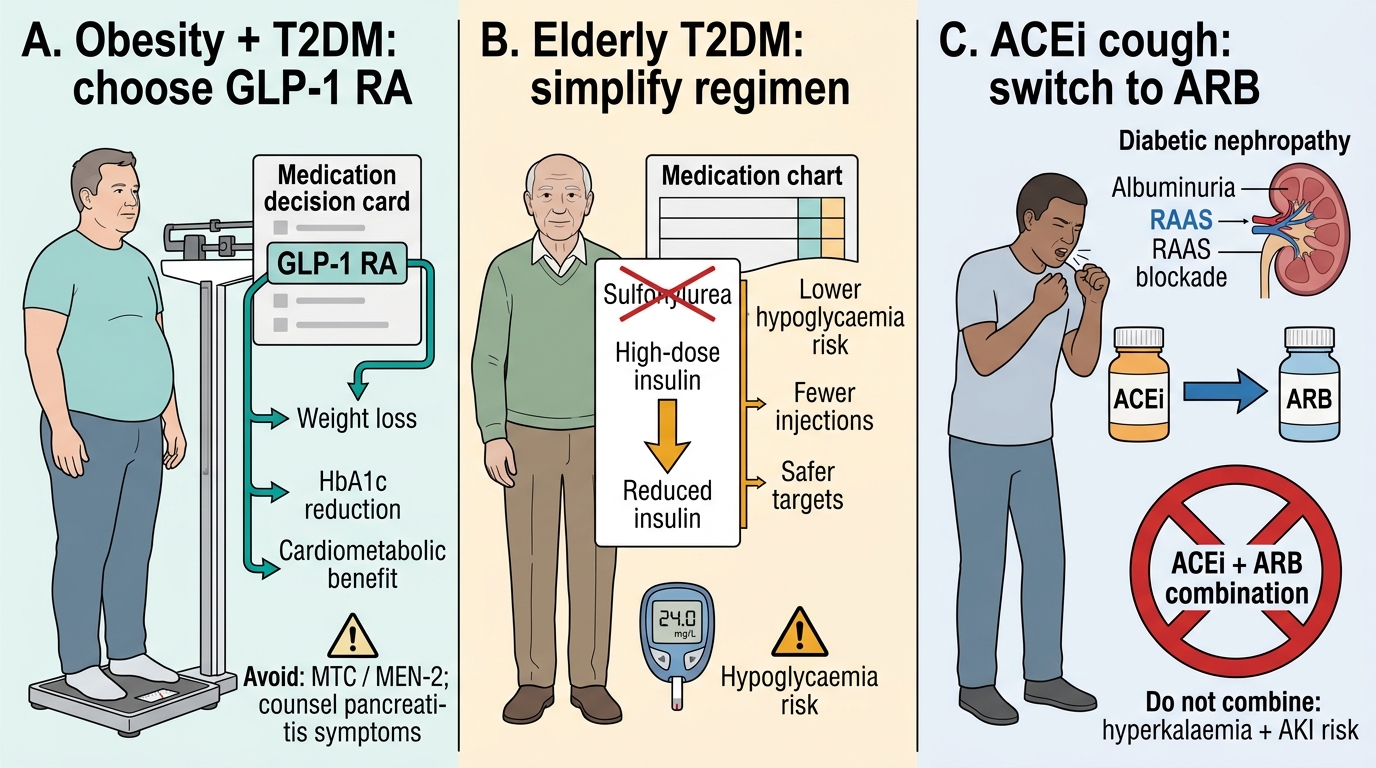
Scenario A: A 45-year-old woman with T2DM (HbA1c 9.1%) is started on metformin 1000 mg twice daily and counselled about lifestyle. At 3-month review her HbA1c is 8.6% — improved but still above target. She has no CVD, eGFR 78, ACR 12 mg/mmol, BMI 33 kg/m², no financial constraints. She is highly motivated to lose weight. Which add-on agent is best aligned with her priorities?
Analysis: She has no CKD, no CVD, no heart failure — so there is no single organ-protective indication driving a specific drug class. However, her BMI 33 with weight loss motivation makes a GLP-1 RA (liraglutide, semaglutide) the most aligned choice: GLP-1 RA are the most weight-reducing class (semaglutide 2.4 mg/week in STEP trials: 15–17% weight loss; liraglutide 3.0 mg/day in SCALE trial: 8–10%). SGLT2i is also reasonable (3–5 kg weight loss). DPP-4i is weight neutral. SU causes weight gain. If cost is relevant: SGLT2i is more affordable than GLP-1 RA in India.
Scenario B: A 78-year-old man with long-standing T2DM and cognitive impairment is on glibenclamide 5 mg twice daily and insulin NPH 20 units at night. His daughter reports several episodes of hypoglycaemia (found confused, blood glucose 45 mg/dL on one occasion). His HbA1c is 6.9%. How should his regimen be modified?
Analysis: An HbA1c of 6.9% in a 78-year-old with cognitive impairment and recurrent hypoglycaemia indicates overtreated diabetes. The ADA recommends a less stringent HbA1c target (7.5–8.5%) in elderly patients with limited life expectancy, multiple comorbidities, or hypoglycaemia unawareness. Immediate changes: (1) Stop glibenclamide — long-acting SU is the most dangerous drug in this setting; (2) Switch to DPP-4i or linagliptin (dose-safe in any eGFR, no hypoglycaemia); (3) Reduce or discontinue NPH — consider switching to safer basal analogue (degludec has lowest hypoglycaemia risk among basal insulins). The goal is simplification and hypoglycaemia prevention, not tight glycaemic control.
Scenario C: A 52-year-old man develops dry cough 4 weeks after starting ramipril 5 mg for diabetic nephropathy. His ACR has improved from 62 to 38 mg/mmol. Should ramipril be continued, and if not, what should replace it?
Analysis: ACEi-induced dry cough (bradykinin-mediated) occurs in 15–20% of Indians (higher than in Caucasians — possible pharmacogenomic difference). It is a class effect of all ACEi and resolves on stopping. ARB (losartan 50–100 mg, telmisartan 40–80 mg, irbesartan 150–300 mg) provides equivalent or superior nephroprotection (RENAAL trial: losartan; IDNT trial: irbesartan) without cough, because ARBs do not inhibit bradykinin breakdown. Switch from ramipril to an ARB — the nephroprotective benefit is maintained and the cough resolves within 1–2 weeks.
High-Yield Diabetes Pharmacotherapy Case Choices
CLINICAL PEARL
Four high-yield pharmacological rules for the final-year examination and clinical practice:
- Metformin and eGFR: Do not start metformin if eGFR <30 mL/min; withhold if eGFR 30–45; dose-reduce if eGFR 45–60. Before iodinated contrast procedures, withhold metformin and restart only after confirming normal renal function 48 hours post-procedure.
- SGLT2i renal thresholds: The glycosuric effect of SGLT2i is attenuated at low eGFR, but the cardio-renoprotective effects persist and the drug is now recommended down to eGFR 20 (empagliflozin/dapagliflozin) or eGFR 30 (canagliflozin) for organ-protection, even if the glucose-lowering contribution is minimal.
- GLP-1 RA and pancreatitis: GLP-1 RA are contraindicated in patients with personal or family history of medullary thyroid carcinoma (MTC) or MEN-2. Pancreatitis is a rare but serious adverse effect — counsel patients to stop the drug and seek assessment if they develop severe upper abdominal pain.
- ACEi vs ARB in diabetic nephropathy: Both are effective; ARBs have the advantage of no cough and are preferred in ACEi-intolerant patients. Do NOT combine ACEi + ARB (increased hyperkalaemia and acute kidney injury risk). If a patient with diabetic nephropathy needs maximum RAAS blockade, use high-dose ARB monotherapy rather than combination.