Page 7 of 17
IM12.8-10 | Thyroid Diagnostic Testing — SDL Guide
Learning Objectives
- Order and interpret diagnostic investigations for thyroid disease in a logical, tiered sequence based on clinical suspicion
- Interpret thyroid function test results across all major patterns including primary and subclinical hypo/hyperthyroidism, T3 thyrotoxicosis, secondary hypothyroidism, and sick euthyroid syndrome
- Interpret CBC findings in the context of thyroid disease including anaemia types and agranulocytosis risk with antithyroid drugs
- Identify atrial fibrillation, sinus bradycardia with low voltage, and electrical alternans on ECG in the clinical context of thyroid dysfunction
INSTRUCTIONS
This skills-based module covers diagnostic test ordering, interpretation, and integration for thyroid disease — thyroid function tests, CBC, and ECG. It maps to NMC competencies IM12.8, IM12.9, and IM12.10 at the SH and KH levels.
References
- Harrison's Principles of Internal Medicine, 21st ed. — Thyroid Function Tests and ECG in Endocrine Disease (textbook)
- API Textbook of Medicine, 10th ed. — Thyroid Investigation and Monitoring (textbook)
- Davidson's Principles and Practice of Medicine, 24th ed. — Laboratory Assessment in Thyroid Disease (textbook)
- American Thyroid Association — Guidelines for Diagnosis and Management of Hyperthyroidism, 2016 (guideline)
- European Thyroid Association — Guidelines for the Management of Subclinical Hypothyroidism, 2013 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients in the thyroid clinic have had their blood results returned. Patient A has TSH 0.01 mIU/L, FT4 28 pmol/L, FT3 9.8 pmol/L. Patient B has TSH 12.4 mIU/L, FT4 8.2 pmol/L, normal FT3. Patient C has TSH 0.02 mIU/L, FT4 22 pmol/L — but unlike Patient A, their ECG shows atrial fibrillation with a ventricular rate of 136 beats per minute and a QRS complex that is irregularly irregular. The ward nurse asks you which of these patients needs immediate action, which needs a routine outpatient plan, and whether any additional investigations are required. The ability to order the right tests in the right sequence, and to interpret the results — TFTs, CBC, ECG — in the context of the clinical presentation is the core of the IM12.8 to IM12.10 competency set. It is also the skill that prevents three serious errors: missing atrial fibrillation in thyrotoxicosis, misinterpreting subclinical thyroid disease, and ordering unnecessary investigations when the clinical picture is already clear.
WHY THIS MATTERS
Thyroid function test interpretation is one of the highest-yield clinical skills in General Medicine. Abnormal TFTs are encountered in almost every specialty — internal medicine, obstetrics, psychiatry, cardiology — and misinterpretation causes diagnostic delay, unnecessary treatment, and patient harm. The NMC competency IM12.8 requires you to order and interpret CBC, TFTs, ECG, and RAIU in the context of a thyroid diagnosis; IM12.9 requires you to identify atrial fibrillation, pericardial effusion, and bradycardia on ECG in a thyroid context; and IM12.10 requires you to interpret TFTs specifically in hypo- and hyperthyroidism. All three are SH or KH level — meaning you must demonstrate these skills, not merely describe them. This module trains you to perform and interpret each test systematically.
RECALL
Before proceeding, recall the key values from the HPT axis physiology covered in the foundations module. TSH is secreted by anterior pituitary thyrotrophs; normal range approximately 0.4–4.0 mIU/L. It is a sensitive but not always specific indicator of primary thyroid status — its interpretation requires clinical context (see pitfalls). Free T4 (FT4) represents the biologically active, unbound fraction of thyroxine; normal range approximately 9–25 pmol/L (or 0.7–2.0 ng/dL). Free T3 (FT3) is rarely needed routinely but useful when TSH is suppressed with normal FT4 (T3 toxicosis). Also recall: in primary thyroid failure, TSH rises and FT4 falls; in primary hyperthyroidism, TSH falls and FT4/FT3 rise; in secondary hypothyroidism (pituitary), both TSH and FT4 are low. These patterns are now applied to the full diagnostic workup.
Indication and Sequence of Diagnostic Testing
The diagnostic workup in thyroid disease is not a reflex panel but a targeted, sequenced investigation strategy guided by the clinical presentation. Ordering the full panel (TSH, FT4, FT3, anti-TPO, TRAb, thyroid ultrasound, RAIU, and scintigraphy) on every patient with a neck lump or fatigue wastes resources, generates false positives, and creates anxiety. The skilled clinician orders tests in tiers, each tier's result directing the next step.
Tier 1 — The screening test: serum TSH. TSH is the single most sensitive test for primary thyroid dysfunction. A normal TSH in a clinically stable patient virtually excludes primary hypo- and hyperthyroidism. Exceptions (where TSH alone is unreliable) are: pituitary/hypothalamic disease (TSH may be low or normal despite low FT4); sick euthyroid syndrome in acutely ill patients; first 6–12 weeks after treatment of hyperthyroidism (TSH suppression persists during recovery); and first trimester of pregnancy (HCG-driven suppression of TSH — normal below 2.5 mIU/L in the first trimester). In these situations, always add FT4 and interpret in context.
Tier 2 — Confirm and characterise: FT4 and FT3. When TSH is abnormal, measure FT4 (and FT3 when TSH is suppressed) to: (a) confirm the direction and magnitude of dysfunction; (b) distinguish overt from subclinical disease (subclinical hypothyroidism: elevated TSH + normal FT4; subclinical hyperthyroidism: suppressed TSH + normal FT4/FT3); (c) identify T3 toxicosis (suppressed TSH, normal FT4, but elevated FT3 — less common form of hyperthyroidism where the toxic gland preferentially secretes T3).
Tier 3 — Identify the cause: autoantibodies and functional tests. Anti-TPO antibodies (anti-thyroid peroxidase): presence confirms autoimmune aetiology (Hashimoto or Graves) — useful for prognosis (elevated anti-TPO in subclinical hypothyroidism predicts progression to overt disease). TRAb (TSH receptor antibodies): essential to confirm Graves disease when clinical diagnosis is uncertain; differentiates Graves from toxic nodular goitre (TRAb positive in Graves, negative in TMNG/toxic adenoma); also useful in pregnancy (high TRAb predicts neonatal thyrotoxicosis).
Tier 4 — Anatomical and functional imaging. Thyroid ultrasound: first-line imaging for structural assessment — characterises goitre (diffuse vs nodular), nodule features (solid/cystic, echogenicity, calcification, margin, vascularity), and cervical lymph nodes; TIRADS classification guides FNA decisions. RAIU and scintigraphy: differentiates the cause of thyrotoxicosis (high vs low uptake; diffuse vs focal pattern) when clinical and antibody assessment is inconclusive — specifically distinguishes Graves from toxic nodular goitre from thyroiditis.
Additional targeted tests:
- Serum calcitonin: if medullary thyroid carcinoma is suspected (neck mass + family history of MEN2 or familial medullary thyroid carcinoma).
- FNAC (ultrasound-guided): for nodules meeting TIRADS-based size criteria for biopsy; Bethesda classification I–VI guides management (I non-diagnostic, II benign, III–IV indeterminate, V suspicious, VI malignant).
- Whole-blood TSH neonatal screening: filter paper test for congenital hypothyroidism; target <3% neonates with TSH >5 mIU/L.

Tiered Investigation Algorithm for Thyroid Dysfunction
CBC and Other Laboratory Investigations in Thyroid Disease
While thyroid function tests are the cornerstone of biochemical diagnosis, a complete blood count (CBC) and other targeted investigations provide important complementary information about the systemic effects of thyroid dysfunction, the severity of the disease, and associated conditions. The NMC IM12.8 competency explicitly requires you to order and interpret CBC alongside TFTs.
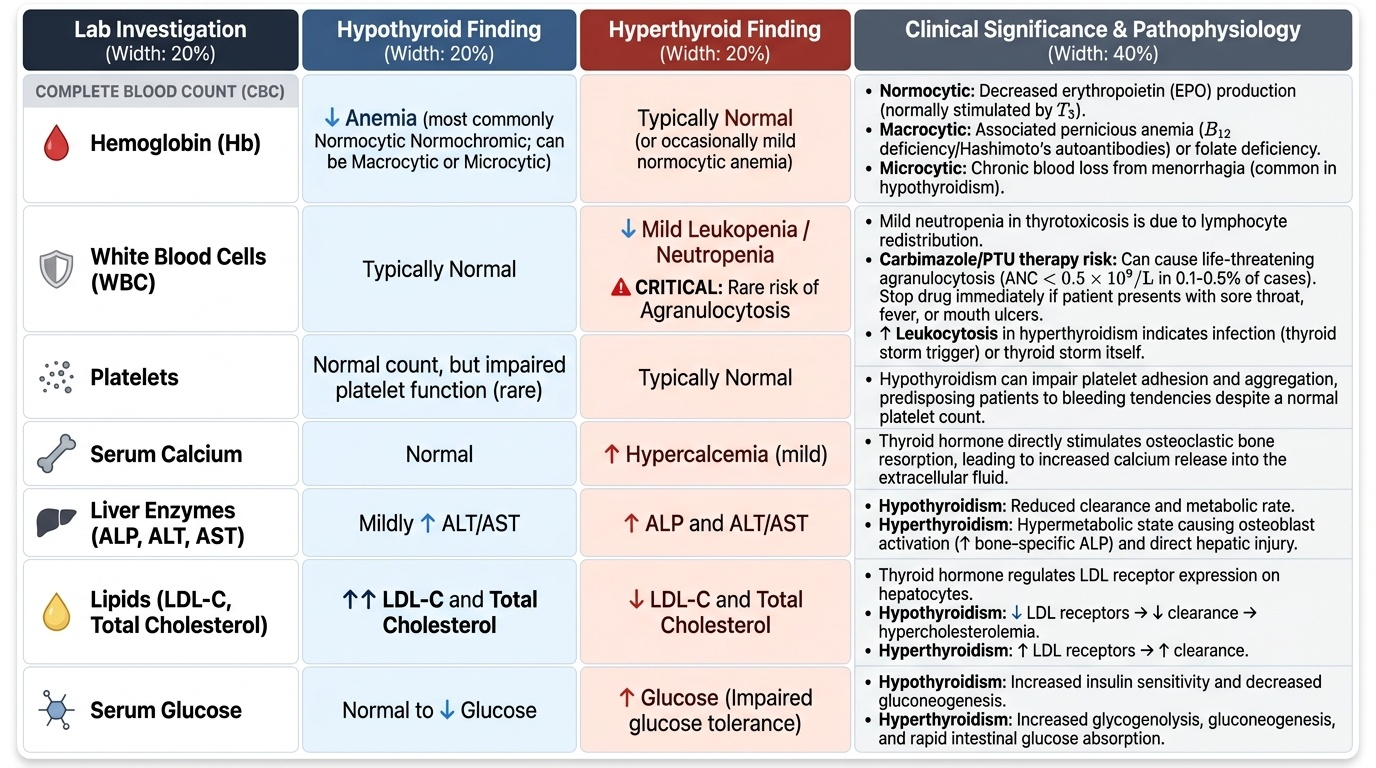
Provided image
CBC in hypothyroidism: Several haematological abnormalities may accompany hypothyroidism. Normocytic normochromic anaemia is the most common finding, reflecting reduced erythropoiesis driven by thyroid hormone deficiency (T3 normally stimulates erythropoietin production). Macrocytic anaemia may result from associated pernicious anaemia (Hashimoto thyroiditis is associated with other organ-specific autoimmune diseases, including pernicious anaemia causing B12 deficiency) or from folate deficiency. Microcytic anaemia may occur if menorrhagia (a common feature of hypothyroidism) has led to iron deficiency. Rarely, hypothyroidism impairs platelet function, predisposing to bleeding. The WBC count is typically normal in primary hypothyroidism.
CBC in thyrotoxicosis: Thyrotoxicosis is associated with leukopenia (reduced WBC, particularly neutropenia), typically mild, due to redistribution of lymphocytes. This is clinically important because it may unmask an underlying susceptibility to infection. More dramatically, the antithyroid drug carbimazole can cause agranulocytosis (absolute neutrophil count <0.5 × 10⁹/L) as a rare but life-threatening side effect — occurring in approximately 0.1–0.5% of patients, typically within the first 3 months of treatment. Every patient starting carbimazole or propylthiouracil (PTU) must be counselled to stop the drug and present immediately if they develop a sore throat, fever, or mouth ulcers. A CBC must be checked urgently in this scenario — agranulocytosis on carbimazole is a medical emergency requiring drug cessation and supportive care (granulocyte colony-stimulating factor (G-CSF) in severe cases). Leucocytosis in a thyrotoxic patient suggests either infection (a precipitant of thyroid storm) or thyroid storm itself, where sympathetic activation may cause demargination of neutrophils.
Other laboratory investigations:
- Serum calcium: Hypercalcaemia may occur in thyrotoxicosis (increased bone resorption; T3 activates osteoclasts directly). Also check calcium if considering MEN2 in medullary thyroid carcinoma (associated hyperparathyroidism).
- Liver function tests: Mildly elevated alkaline phosphatase and ALT are common in thyrotoxicosis due to increased bone ALP (thyroid-driven osteoclast activity) and liver involvement. Frank hepatitis-pattern LFT elevation may be caused by PTU (rare but serious hepatotoxicity — PTU is generally avoided except in the first trimester of pregnancy for this reason; carbimazole preferred thereafter).
- Serum glucose: Thyrotoxicosis causes hyperglycaemia through increased gluconeogenesis and reduced insulin sensitivity; hypothyroidism may aggravate hypoglycaemia in patients with diabetes. Check fasting glucose in new-onset thyroid disease.
- Lipid profile: Hypothyroidism is a secondary cause of dyslipidaemia — elevated LDL and total cholesterol from reduced LDL receptor expression. These abnormalities may partially or fully reverse with levothyroxine treatment.
- Serum TSH-receptor antibodies (TRAb): Measured in hyperthyroid patients to distinguish Graves (TRAb positive) from TMNG/toxic adenoma (TRAb negative); also in pregnancy (predicts neonatal thyrotoxicosis if high).
- Urinary iodine concentration (UIC): Population-level indicator of iodine status (not routinely used clinically but required for NIDDCP monitoring); median UIC <100 µg/L = iodine deficiency.
Thyroid Function Test Interpretation
Interpreting thyroid function tests (TFTs) correctly requires integrating the TSH result with FT4 and FT3 in the context of the clinical presentation. The reference ranges used below are approximate; actual laboratory reference ranges vary slightly between methods and platforms — always interpret against your institution's reference interval. The key patterns to master are overt hypothyroidism, subclinical hypothyroidism, overt hyperthyroidism, subclinical hyperthyroidism, T3 toxicosis, secondary hypothyroidism, and sick euthyroid syndrome. Each pattern has specific clinical implications that must be linked to management decisions.
Pattern 1 — Primary overt hypothyroidism: TSH elevated (>4.0, often substantially above 10 mIU/L in overt disease) + FT4 below normal range. Clinical features of hypothyroidism present. Aetiology: Hashimoto thyroiditis (anti-TPO positive), iodine deficiency, post-radioiodine, post-thyroidectomy, drug-induced (amiodarone, lithium). Action: start levothyroxine replacement; titrate dose to normalise TSH within 4–6 weeks of a dose change.
Pattern 2 — Subclinical hypothyroidism: TSH elevated (typically 4.0–10 mIU/L) + FT4 within normal range. Patient may be asymptomatic or have non-specific symptoms. Clinical significance: risk of progression to overt hypothyroidism (~5% per year if anti-TPO positive, ~2% per year if antibody negative); associated with adverse cardiovascular outcomes if TSH >10 mIU/L; increased risk of pregnancy complications. Treatment threshold: TSH >10 mIU/L (treat with levothyroxine); TSH 4–10 mIU/L (treat if symptomatic, if anti-TPO positive, if pregnant or planning pregnancy, or if cardiovascular risk factors present).
Pattern 3 — Primary overt hyperthyroidism: TSH suppressed (<0.1, often undetectable) + FT4 and/or FT3 elevated. Clinical features of thyrotoxicosis present. Distinguish by antibodies and RAIU (see foundations module): TRAb positive = Graves; TRAb negative + nodular goitre = TMNG/toxic adenoma; low RAIU = thyroiditis.
Pattern 4 — Subclinical hyperthyroidism: TSH suppressed (<0.1 or 0.1–0.4 mIU/L) + FT4 and FT3 within normal range. Often asymptomatic. Clinical significance: increased risk of atrial fibrillation (3-fold higher in patients with TSH <0.1); bone loss (particularly in postmenopausal women). Management: TSH 0.1–0.4 mIU/L — monitor (may be transient); TSH <0.1 mIU/L — treat if >65 years, cardiac disease, osteoporosis, or postmenopausal; caused by levothyroxine over-replacement or autonomous nodule.
Pattern 5 — T3 thyrotoxicosis: TSH suppressed + FT4 normal + FT3 elevated. The toxic gland preferentially secretes T3. FT3 measurement is essential to confirm hyperthyroidism in this pattern — without it, the normal FT4 could be misinterpreted as subclinical hyperthyroidism. Most commonly seen in toxic adenoma or early Graves disease.
Pattern 6 — Secondary hypothyroidism (central): TSH low or normal + FT4 low. The pituitary fails to secrete adequate TSH despite low T4 — absence of the expected TSH rise. Always associated with other evidence of hypopituitarism (low cortisol, low FSH/LH, or imaging finding of pituitary mass/empty sella). Critical to identify because: (a) treatment requires addressing the underlying pituitary pathology; (b) corticosteroid replacement MUST precede thyroid hormone replacement to prevent precipitating adrenal crisis.
Pattern 7 — Sick euthyroid syndrome (non-thyroidal illness): In acutely ill patients, cytokines (IL-1, IL-6, TNF-alpha) suppress the HPT axis — TSH may be low or normal, FT3 is typically low (reduced peripheral conversion), and FT4 may be low or normal. This pattern mimics primary hyperthyroidism (suppressed TSH) or secondary hypothyroidism. Key distinguishing features: the patient is acutely systemically ill; FT3 is disproportionately low relative to FT4; TSH often returns to normal rapidly as the patient recovers. Management: do NOT start thyroid hormone in sick euthyroid syndrome — it does not improve outcomes and may worsen them; recheck TFTs after recovery.
| TFT Pattern | TSH | FT4 | FT3 | Interpretation |
|---|---|---|---|---|
| Primary overt hypothyroidism | High (>10) | Low | Low | Treat with levothyroxine |
| Subclinical hypothyroidism | High (4–10) | Normal | Normal | Treat if TSH >10, or if risk factors |
| Primary overt hyperthyroidism | Suppressed (<0.1) | High | High | Treat; RAIU/TRAb to find cause |
| Subclinical hyperthyroidism | Low/suppressed | Normal | Normal | Monitor or treat if risk factors |
| T3 thyrotoxicosis | Suppressed | Normal | High | Check FT3; treat as hyperthyroid |
| Secondary hypothyroidism | Low/normal | Low | Low | Pituitary imaging; cortisol first |
| Sick euthyroid | Low/normal | Low/normal | Low | Do NOT treat; recheck after recovery |
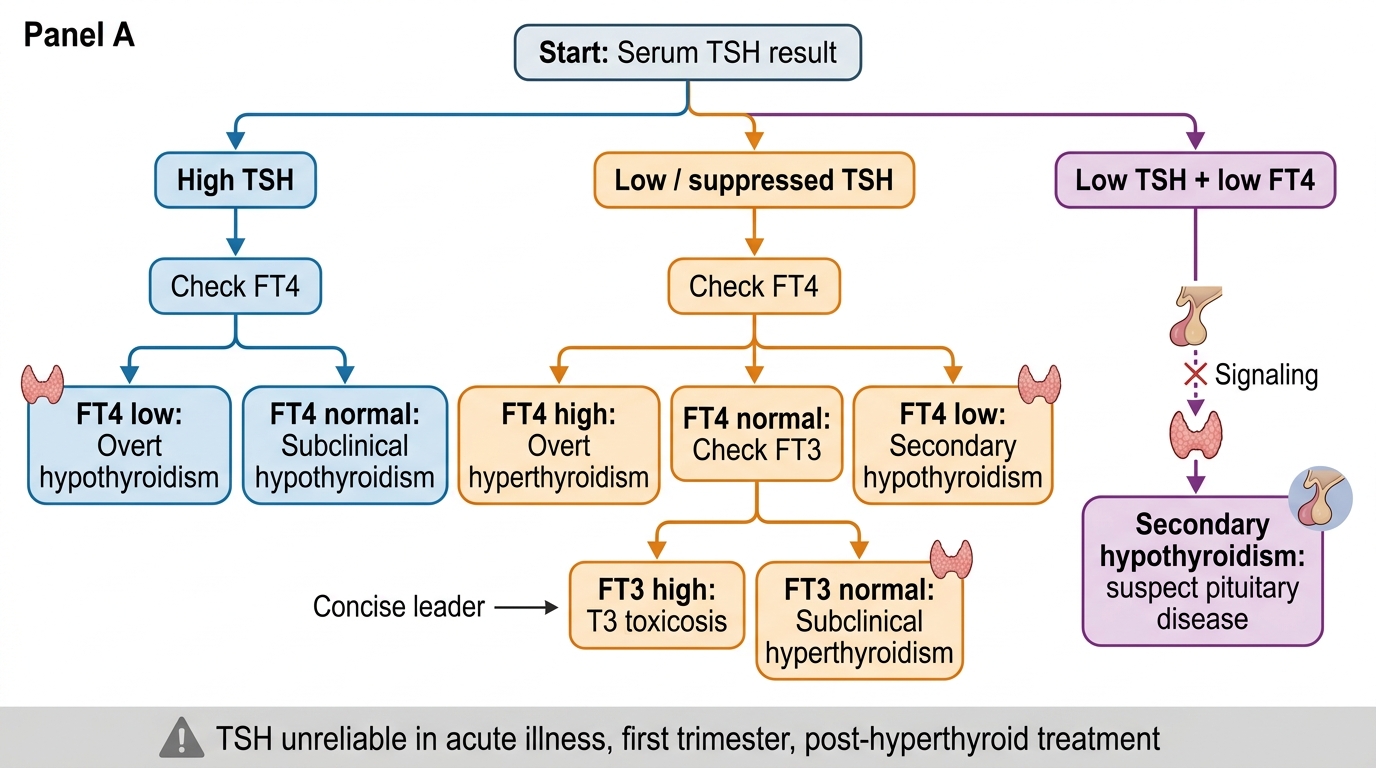
TFT Interpretation Algorithm
SELF-CHECK
A 68-year-old woman with osteoporosis has serum TSH 0.08 mIU/L (reference 0.4–4.0), FT4 15 pmol/L (normal), and FT3 4.2 pmol/L (normal). She is asymptomatic for thyrotoxicosis. She is not taking any thyroid medication. Which statement best describes the management approach?
A. No treatment required — TSH is only mildly suppressed and she is asymptomatic
B. Start antithyroid drug therapy immediately to normalise TSH
C. Subclinical hyperthyroidism with TSH <0.1 mIU/L in a postmenopausal woman with osteoporosis warrants treatment to prevent further bone loss; investigate the cause (RAIU/TRAb) and treat accordingly
D. This pattern is most consistent with sick euthyroid syndrome — do not treat, recheck in 6 weeks
Reveal Answer
Answer: C. Subclinical hyperthyroidism with TSH <0.1 mIU/L in a postmenopausal woman with osteoporosis warrants treatment to prevent further bone loss; investigate the cause (RAIU/TRAb) and treat accordingly
This is subclinical hyperthyroidism — TSH suppressed (<0.1 mIU/L) with normal FT4 and FT3. In a 68-year-old postmenopausal woman with existing osteoporosis, subclinical hyperthyroidism is an established risk factor for accelerated bone loss and fracture, as well as increased risk of atrial fibrillation. The threshold for treatment is TSH <0.1 mIU/L in patients over 65, those with cardiac disease (AF risk), and those with osteoporosis — all present here. The cause should be investigated first (autonomous nodule on RAIU? — if a single hot nodule, radioiodine ablation is appropriate). Option A is incorrect — the osteoporosis risk makes watchful waiting inappropriate here. Sick euthyroid syndrome (option D) is associated with acute systemic illness and shows disproportionately low FT3; this patient is otherwise well.