Page 8 of 17
IM12.8-10 | Thyroid Diagnostic Testing — SDL Guide (Part 2)
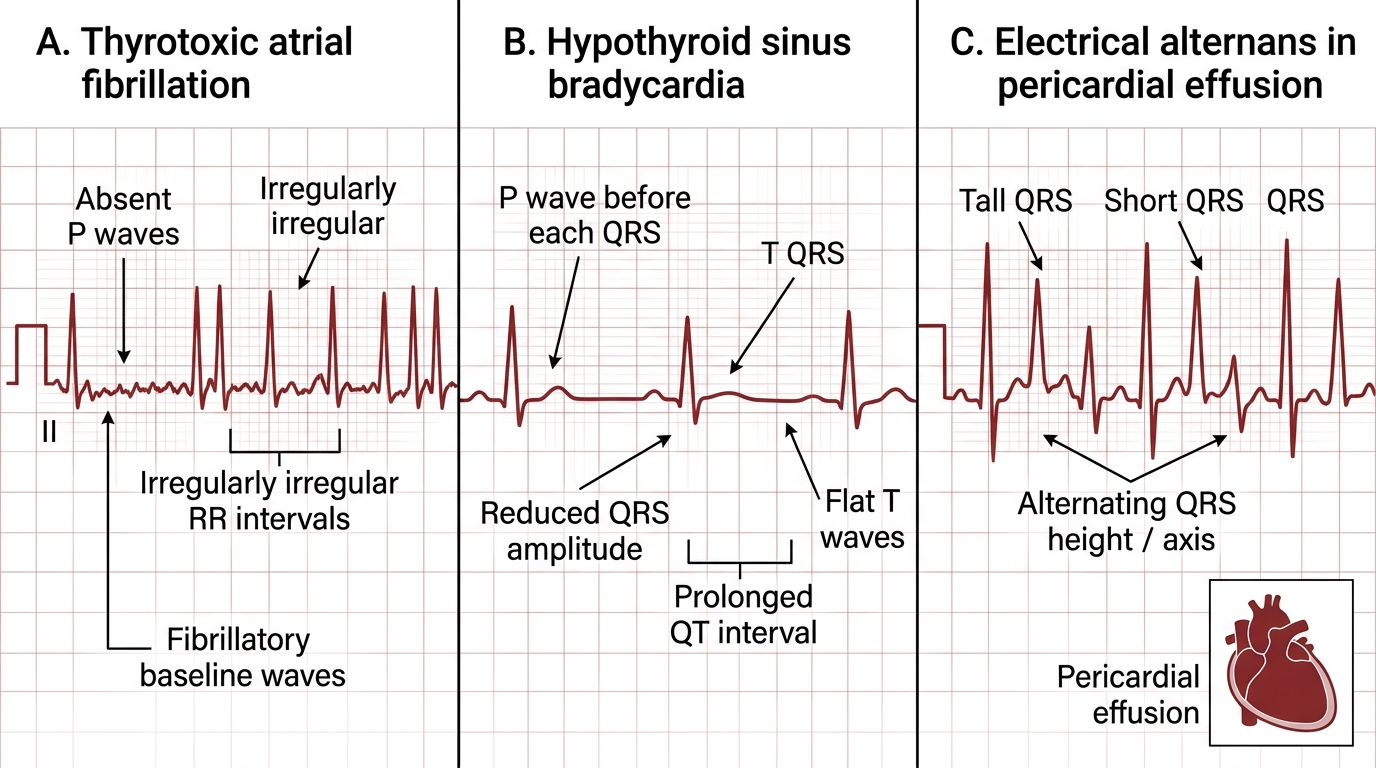
ECG Interpretation in Thyroid Disease
The electrocardiogram (ECG) is an essential investigation in both hyperthyroidism and severe hypothyroidism, providing objective evidence of cardiac complications and directly influencing management decisions. The NMC IM12.9 competency requires you to identify three specific ECG patterns in the thyroid context: atrial fibrillation, pericardial effusion, and bradycardia. Each pattern corresponds to a specific thyroid condition and carries specific management implications. Before interpreting any ECG, apply the systematic reading approach: rate → rhythm → axis → P waves → PR interval → QRS complex → ST segment → T waves → QT interval.
Atrial fibrillation (AF) in thyrotoxicosis:
AF is the most serious cardiac complication of hyperthyroidism, occurring in 10–15% of thyrotoxic patients, with the incidence rising sharply in older patients and those with subclinical hyperthyroidism. Excess T3/T4 has direct electrophysiological effects on atrial tissue: it shortens the atrial refractory period, increases ectopic foci, and sensitises the heart to catecholamines — all promoting AF. Additionally, high-output cardiac failure from tachycardia and increased stroke volume may further destabilise atrial rhythm.
ECG features of atrial fibrillation:
- Absent P waves: The chaotic atrial depolarisation of AF produces no organised P wave — instead, there is a fine or coarse irregular baseline (fibrillatory waves) best seen in leads V1 and II.
- Irregularly irregular R-R intervals: The hallmark of AF — ventricular response is irregular because AV node conduction of atrial impulses is random. This is the most important ECG criterion.
- Normal (narrow) QRS morphology: Unless there is aberrant conduction or pre-existing bundle branch block.
- Ventricular rate: Variable (typically 100–180 bpm in untreated thyrotoxic AF, depending on AV nodal tone).
The clinical significance of AF in thyrotoxicosis: (1) it may precipitate acute cardiac decompensation; (2) it carries thromboembolic risk and requires anticoagulation assessment (CHA₂DS₂-VASc score); (3) up to 50–60% of thyrotoxic AF reverts spontaneously to sinus rhythm when euthyroidism is restored — therefore, cardioversion is generally deferred until the thyrotoxicosis is treated. Rate control (beta-blockers — propranolol or atenolol — preferred) should be initiated immediately.
Sinus tachycardia in thyrotoxicosis: More common than AF. ECG shows regular rhythm with identifiable P waves before each QRS, rate typically 100–140 bpm. Responds well to beta-blockade.
Bradycardia in hypothyroidism:
Sinus bradycardia (rate <60 bpm) is a common ECG finding in hypothyroidism, reflecting the reduced sympathetic tone and decreased cardiac sensitivity to catecholamines. The ECG shows: regular rhythm, normal P waves, normal QRS, prolonged QTc interval (due to slowed repolarisation). Additional ECG features in hypothyroidism include: low-voltage complexes (reduced amplitude of QRS, P waves, and T waves throughout all leads) — caused by pericardial effusion dampening the electrical signal or by myxoedematous changes in the myocardium; flat or inverted T waves in multiple leads; and prolonged PR interval (first-degree heart block, from AV nodal slowing).
Pericardial effusion in hypothyroidism:
Pericardial effusion occurs in ~30% of patients with severe, long-standing hypothyroidism, resulting from mucopolysaccharide deposition in the pericardium and increased vascular permeability (the same mechanism as peripheral oedema and myxoedema). The fluid accumulates slowly, so cardiac tamponade is rare despite sometimes large effusions.
ECG features of pericardial effusion:
- Low-voltage complexes: QRS amplitude <5 mm in all limb leads and <10 mm in all precordial leads — the most consistent finding.
- Electrical alternans: The QRS complex alternates in axis with each beat (the heart swings within the effusion, altering its orientation) — a specific though insensitive sign; when present, it strongly suggests a haemodynamically significant effusion (cardiac tamponade).
- Sinus tachycardia: In large effusions with tamponade, compensatory tachycardia develops (in hypothyroidism with tamponade, this may be masked by bradycardia from the underlying disease).
- Diffuse ST elevation (saddle-shaped) + PR depression are features of pericarditis (inflammation), not effusion alone — may coexist but are not required for the diagnosis of effusion.
Echocardiography is the definitive investigation for pericardial effusion and is far more sensitive than ECG. However, ECG low voltage in a hypothyroid patient should prompt echocardiography.
ECG Patterns in Thyroid Dysfunction
SELF-CHECK
A 74-year-old woman is admitted with palpitations and breathlessness. Her ECG shows an irregularly irregular rhythm with absent P waves and a ventricular rate of 128 bpm. Serum TSH is undetectable; FT4 is 32 pmol/L. She takes no anticoagulants. Her CHA₂DS₂-VASc score is 3 (age, sex, hypertension). What is the MOST appropriate immediate management strategy?
A. Emergency DC cardioversion to restore sinus rhythm before treating thyrotoxicosis
B. Start antithyroid drugs, initiate rate control with a beta-blocker, and commence anticoagulation; defer cardioversion until euthyroidism is achieved
C. Radioiodine ablation as the fastest definitive treatment for thyrotoxic AF
D. Start digoxin alone for rate control — beta-blockers are contraindicated in thyrotoxic AF
Reveal Answer
Answer: B. Start antithyroid drugs, initiate rate control with a beta-blocker, and commence anticoagulation; defer cardioversion until euthyroidism is achieved
Thyrotoxic AF is managed by treating the underlying thyrotoxicosis (antithyroid drugs), rate control (beta-blockers preferred — propranolol or atenolol; digoxin is less effective due to heightened adrenergic tone and is a second-line agent, not first-line), and anticoagulation based on CHA₂DS₂-VASc score. A score of ≥2 in women (or ≥1 in men) indicates anticoagulation — this patient scores 3, warranting anticoagulation with a DOAC or warfarin. Cardioversion is NOT appropriate immediately: up to 50–60% of thyrotoxic AF spontaneously reverts to sinus rhythm once euthyroidism is restored, and cardioverting before treating the thyrotoxicosis carries high recurrence risk. Radioiodine ablation is a definitive treatment but takes weeks to months to achieve euthyroidism — not appropriate as the immediate step.
Applied Diagnostic Practice: Integrated Cases
This section applies the diagnostic testing framework from this module to integrated clinical cases, mirroring the decision-making you will perform in clinical postings and examinations. For each case, work through the investigation sequence: what tests do you order, in what order, and what does each result tell you? Focus on the reasoning process — which TFT pattern, which ECG finding, which additional test result — and articulate how each finding modifies your differential and management plan. This is the IM12.8–IM12.10 skills integration stage: moving from individual test interpretation to coordinated clinical reasoning in a real patient encounter.
A brief review of the critical decision points in thyroid diagnostic testing before the cases: (1) TSH is the entry point for all thyroid workups; (2) FT4 and FT3 are confirmed when TSH is abnormal; (3) the distinction between overt and subclinical disease (FT4 normal vs abnormal) has direct management implications; (4) ECG should be obtained in every patient with symptomatic thyrotoxicosis to exclude AF and assess rate; (5) CBC must be checked before starting antithyroid drugs (baseline) and urgently if agranulocytosis is suspected during treatment. These five decision rules prevent the most common diagnostic and management errors.
Case A: A 44-year-old woman presents with a 4-month history of increasing fatigue, weight gain, and cold intolerance. TSH 18.4 mIU/L; FT4 6.1 pmol/L; Anti-TPO antibodies 480 IU/mL (elevated; reference <35). CBC: Hb 10.2 g/dL, MCV 98 fL, WBC normal, platelets normal. Interpret the results and outline next investigations.
Analysis: Overt primary hypothyroidism (TSH markedly elevated, FT4 low) due to Hashimoto thyroiditis (elevated anti-TPO antibodies, characteristic firm rubbery goitre pattern). CBC shows macrocytic anaemia (Hb 10.2, MCV 98) — in the context of Hashimoto thyroiditis, the most important differential for macrocytosis is pernicious anaemia (autoimmune atrophic gastritis with vitamin B12 deficiency) — this autoimmune association is well established. Next investigations: serum vitamin B12 and folate, serum iron/ferritin (to exclude concurrent iron deficiency from menorrhagia), intrinsic factor antibodies (if B12 low), anti-parietal cell antibodies. Begin levothyroxine after baseline investigations; recheck TSH in 6 weeks.
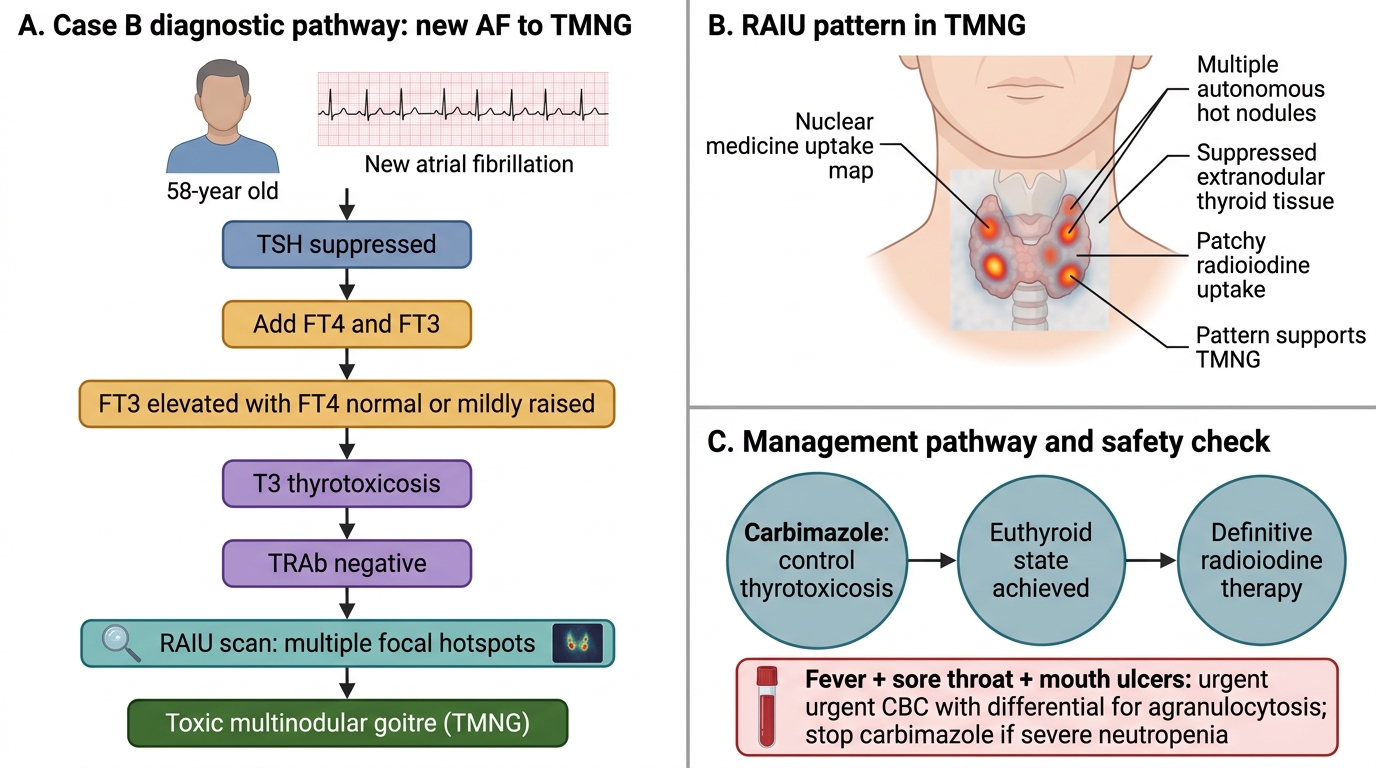
Case B: A 58-year-old man is referred from cardiology after new-onset atrial fibrillation is found during a routine ECG. He denies palpitations or heat intolerance. He has lost 3 kg over the past 2 months. Examination: irregularly irregular pulse 88 bpm (rate-controlled by the cardiologist with diltiazem). Thyroid: small bilateral nodules palpable. TFT results: TSH 0.02 mIU/L; FT4 19 pmol/L (upper normal); FT3 8.9 pmol/L (elevated). TRAb: negative. RAIU: multiple focal areas of increased uptake.
Analysis: T3 thyrotoxicosis in the context of toxic multinodular goitre (TMNG). TSH is suppressed and FT4 is at the upper limit of normal — without FT3, this could be misinterpreted as subclinical hyperthyroidism. The elevated FT3 confirms overt T3 thyrotoxicosis. TRAb negative excludes Graves disease. Multiple focal areas of increased uptake on RAIU confirms TMNG (not Graves, which would show diffuse uptake). Apathetic hyperthyroidism in an older male — no adrenergic symptoms. Management: rate control maintained; antithyroid drugs (carbimazole) to achieve euthyroidism; then definitive therapy — radioiodine ablation preferred for TMNG (surgery if very large goitre or retrosternal extension); CHA₂DS₂-VASc score for anticoagulation decision.
Case B: T3 Thyrotoxicosis Due to Toxic Multinodular Goitre
SELF-CHECK
A patient on carbimazole 30 mg daily for Graves disease presents to the Emergency Department 6 weeks after starting treatment with a 3-day history of high-grade fever (39.2°C), sore throat, and painful mouth ulcers. Which immediate investigation is the SINGLE MOST URGENT to order?
A. Thyroid function tests (TSH and FT4) to assess hyperthyroid control
B. Blood culture to identify the causative organism of presumed sepsis
C. Full blood count (CBC) with differential to assess for agranulocytosis
D. Throat swab for culture and sensitivity
Reveal Answer
Answer: C. Full blood count (CBC) with differential to assess for agranulocytosis
Agranulocytosis is a rare but life-threatening idiosyncratic reaction to thionamide drugs (carbimazole, PTU), occurring in 0.1–0.5% of patients, typically in the first 3 months of treatment. The presentation — high-grade fever, sore throat, and mouth ulcers — is the classic triad of agranulocytosis. The single most urgent test is a CBC with differential to check the absolute neutrophil count (ANC). If ANC <0.5 × 10⁹/L, carbimazole must be stopped IMMEDIATELY and the patient admitted for supportive care (G-CSF may be used in severe cases). Every patient starting carbimazole or PTU must be counselled to stop the drug and seek immediate medical assessment if they develop this symptom triad. TFTs and blood cultures are important but secondary — the priority is to confirm or exclude agranulocytosis, which requires immediate drug cessation before any sepsis workup.
Self-Assessment: Diagnostic Test Interpretation
You have now covered the full diagnostic testing framework for thyroid disease — investigation sequencing, TFT interpretation across all seven major patterns, CBC findings and their clinical relevance, and ECG interpretation in thyrotoxicosis and hypothyroidism. This self-assessment section tests whether you can apply these competencies to unseen clinical scenarios, as required at the SH/KH level for IM12.8, IM12.9, and IM12.10. Work through each question independently before reading the analysis. Pay particular attention to the reasoning chain — the sequence of test results that leads to each diagnostic conclusion — rather than pattern-matching to a list of diseases.
As a final anchor, the three ECG patterns you must recognise in the thyroid context are: (1) Atrial fibrillation — absent P waves, irregularly irregular RR intervals, ventricular rate often 100–180 bpm; seen in thyrotoxicosis; (2) Bradycardia with low-voltage complexes — sinus rate <60 bpm, reduced QRS amplitude in all leads, flat/inverted T waves; seen in hypothyroidism; (3) Electrical alternans — alternating QRS axis beat-to-beat; specific for haemodynamically significant pericardial effusion (may accompany severe hypothyroidism).
Q1: A pregnant woman at 8 weeks gestation has TSH 0.15 mIU/L, FT4 16 pmol/L (normal), FT3 5.2 pmol/L (normal). She has no symptoms of thyrotoxicosis and no goitre. Anti-TPO antibodies negative; TRAb negative. How do you interpret this result?
Analysis: This is a normal physiological finding in early pregnancy. HCG cross-reacts with the TSH receptor due to structural homology (both are glycoproteins with an alpha subunit in common); high HCG levels in the first trimester weakly stimulate thyroid cells, causing mild suppression of TSH. Normal TSH range in the first trimester is lower than in the non-pregnant adult — approximately 0.1–2.5 mIU/L. A TSH of 0.15 with normal FT4/FT3 and no antibodies in the first trimester is a normal gestational finding, not Graves disease or pathological thyrotoxicosis. No treatment is indicated. Gestational thyrotoxicosis (hyperemesis gravidarum-associated) is self-limiting; true Graves disease in pregnancy (TRAb positive) requires careful antithyroid drug treatment (PTU preferred in first trimester due to carbimazole embryopathy risk).
Q2: A 55-year-old woman with long-standing hypothyroidism on levothyroxine 100 µg daily presents for a routine review. Her TSH is 0.08 mIU/L (suppressed), FT4 18 pmol/L (normal). She feels well. She has osteoporosis. What is your assessment and management?
Analysis: This patient has over-replacement with levothyroxine — subclinical hyperthyroidism (TSH <0.1 with normal FT4). In a 55-year-old postmenopausal woman with osteoporosis, chronic TSH suppression accelerates bone loss and increases fracture risk. The levothyroxine dose should be reduced to bring TSH into the low-normal range (0.5–1.5 mIU/L is a reasonable target for most hypothyroid patients on replacement). Recheck TSH 6–8 weeks after dose adjustment. This is a common and clinically important error — routine monitoring of TSH in patients on levothyroxine is not to ensure compliance alone, but to prevent iatrogenic subclinical hyperthyroidism.
CLINICAL PEARL
The two most dangerous errors in thyroid diagnostic testing are: (1) missing T3 thyrotoxicosis by not measuring FT3 when TSH is suppressed and FT4 is normal — always check FT3 when TSH is suppressed to exclude T3 toxicosis; and (2) missing agranulocytosis on carbimazole by not acting immediately on the triad of fever, sore throat, and mouth ulcers — the CBC must be checked urgently and the drug stopped if ANC <0.5 × 10⁹/L. Both errors are preventable, both can be life-threatening, and both arise from failure to follow a systematic testing protocol. A third important clinical point: ECG should be obtained in every patient with symptomatic thyrotoxicosis — not only when palpitations are reported. Thyrotoxic AF in elderly patients can be clinically silent, and anticoagulation decisions depend on its detection.