Page 14 of 21
IM13.{5,13,17-19} | Cancer Pain and End of Life Care — SDL Guide
Learning Objectives
- Describe the common issues encountered in patients at the end of life and the principles of end-of-life care management
- Describe and assess pain and suffering objectively in a patient with cancer using validated tools
- Describe the indications, use, side effects, and safe prescribing of narcotics in cancer pain management
- Describe and discuss the ethical and medico-legal issues involved in end-of-life care in the Indian context
- Describe the therapies used in alleviating suffering in patients at the end of life
INSTRUCTIONS
Palliative care is a human right, not a last resort. This module addresses cancer pain assessment and management, the principles of end-of-life care, the ethical and legal dimensions of dying in India, and the full spectrum of therapies that alleviate suffering. Mastery of these skills transforms the physician from someone who treats disease to someone who cares for persons.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 12 — Palliative and End-of-Life Care (textbook)
- API Textbook of Medicine, 10th ed., Palliative Care and Pain Management (textbook)
- WHO Guidelines on the Pharmacological Treatment of Persistent Pain in Adults with Medical Illnesses, 2021 (guideline)
- IAPC (Indian Association of Palliative Care) National Standards for Palliative Care in India (guideline)
- Government of India Narcotic Drugs and Psychotropic Substances (NDPS) Amendment Act 2014 — Rule 14B (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Suresh is a 64-year-old retired school teacher with advanced lung cancer. He has not slept in three nights because of severe thoracic back pain from a T7 vertebral metastasis. His pain score is 9 out of 10. He is also breathless at rest, nauseated from his last chemotherapy cycle, and his family is sleeping in shifts to monitor him. He is not on any opioid analgesic — his family had refused morphine because 'people die when they get morphine'. His oncologist, overwhelmed with outpatient volume, has not addressed his pain for two visits. Right now, in this moment, Suresh is suffering — not from his cancer, but from undertreated pain that is entirely manageable with existing medications, existing guidelines, and existing law. This module ensures that you are never the reason a patient like Suresh continues to suffer.
WHY THIS MATTERS
Cancer pain is undertreated across India at an epidemic scale. The WHO estimated that India requires 284 metric tonnes of medical-grade oral morphine equivalent annually; actual consumption is less than 2 metric tonnes — less than 1% of need. NMC competencies IM13.5, IM13.13, IM13.17, IM13.18, and IM13.19 address the full spectrum of palliative and end-of-life care from symptom assessment to narcotic prescribing to ethics. These competencies are not peripheral to internal medicine — they represent some of the most frequently encountered and most profoundly impactful skills in final-year practice, particularly in Indian public health settings where palliative care infrastructure remains thin and the general physician must step into this role.
RECALL
Activate your prior knowledge. From pharmacology, recall the opioid receptor subtypes (mu, kappa, delta) and the concept of full agonists (morphine, oxycodone), partial agonists (buprenorphine), and mixed agonist-antagonists (nalbuphine). Recall the mechanism of NSAIDs (COX-1 and COX-2 inhibition, prostaglandin reduction) and their limitations (GI bleeding, renal impairment, cardiovascular risk). From your ethics module, recall the principles of autonomy, beneficence, non-maleficence, and justice — all four apply to end-of-life decisions. From law, recall that the Supreme Court of India in its landmark judgment in Common Cause v. Union of India (2018) recognised the right to die with dignity as part of the fundamental right to life under Article 21, and endorsed advance directives (living wills) as legally valid — a critical point for end-of-life discussions in India.
Clinical Indications for Palliative Care — When and Why
Palliative care is the specialised branch of medicine focused on the prevention and relief of suffering — physical, psychological, social, and spiritual — in patients with life-limiting illness and their families. The World Health Organization's 2002 definition explicitly states that palliative care neither hastens nor postpones death; it affirms life and regards dying as a normal process. Palliative care is not a specialty only for the dying — it is applicable from the time of diagnosis of a life-limiting illness, delivered in parallel with curative or disease-modifying treatment.
The clinical indications for initiating specialist palliative care input in a cancer patient are: (1) any Stage IV (metastatic) solid cancer, regardless of treatment status — the palliative care team should be involved from the point of metastatic diagnosis, not after treatment fails; (2) uncontrolled symptoms — pain, dyspnoea, nausea, fatigue, psychological distress — that are not adequately managed by the oncology team; (3) declining performance status (ECOG PS 3–4) — the patient is approaching functional dependence and will require active symptom management and care planning; (4) complex social and psychosocial needs — caregiver burden, family conflict about treatment decisions, financial catastrophe, anticipatory grief; (5) explicit patient request for supportive care priorities, or a conversation about goals of care and the patient's wishes about life-sustaining treatment; (6) any patient with a prognosis estimated at ≤12 months from a haematological or solid malignancy.
Early integration of palliative care — the model endorsed by ASCO (2012 guidelines), ESMO (2023), IAPC, and the WHO — has been shown in multiple randomised trials (Temel et al. NEJM 2010; Zimmermann et al. Lancet Oncol 2014) to improve quality of life, reduce depression and anxiety, reduce emergency department visits, reduce receipt of futile end-of-life chemotherapy, AND extend overall survival. The mechanism is not mysterious: when suffering is better controlled, patients maintain better nutritional status, better sleep, better immune function, and make better-informed decisions about discontinuing futile treatments that accelerate decline.
Prognostic indicators that signal approaching end of life (relevant to hospice referral and goals-of-care discussions): PPS (Palliative Performance Scale) ≤40%; unable to take oral medications; ≥10% weight loss in the past 6 months; severe hypoalbuminaemia (<25 g/L); dyspnoea at rest; rapid functional decline over weeks. These are clinical signs of the terminal phase — the period during which death is expected within days to weeks and the focus of care shifts entirely to comfort.
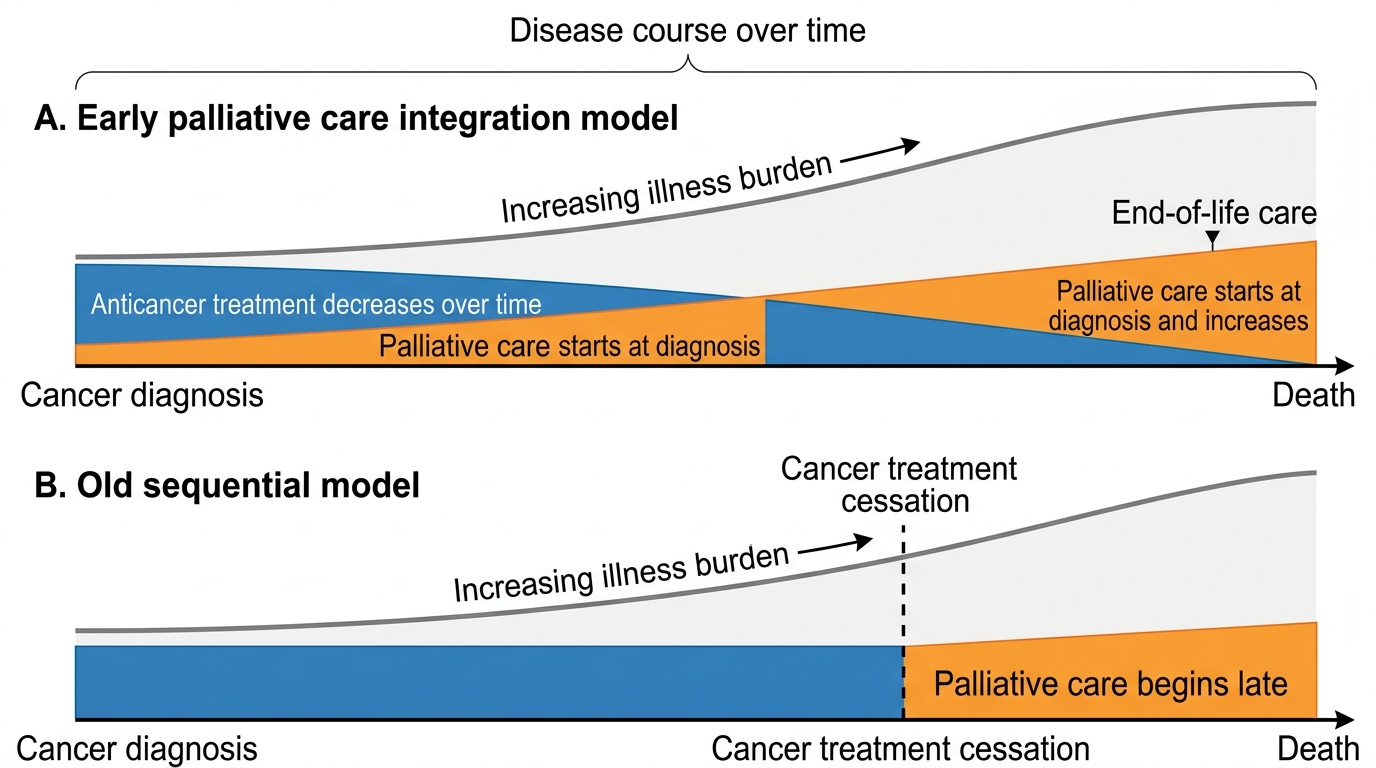
Early Integrated Palliative Care in Cancer
Cancer Pain Assessment — Objective and Validated Tools
Pain is the most common and most feared symptom in cancer. Approximately 30–50% of patients with early-stage cancer and 70–90% of patients with advanced cancer experience moderate to severe pain. Yet pain is also the most undertreated cancer symptom — particularly in India, where a combination of regulatory barriers, opiophobia among physicians and patients, poor palliative care infrastructure, and historical cultural attitudes to pain as inevitable suffering has created what the NHRC (National Human Rights Commission) described in 2012 as a 'national crisis of unrelieved cancer pain.'
Effective pain management begins with systematic, objective assessment using validated tools. Assessment must cover seven dimensions — the 'OPQRST' mnemonic adapted for cancer pain: Onset and chronology (when did pain start? has it changed?); Provocating and relieving factors (movement-related = bone/neuropathic; position-related = visceral/capsular stretch); Quality and character (burning/shooting = neuropathic; dull/aching = somatic visceral; sharp/stabbing = musculoskeletal/peritoneal); Radiation and referral (shoulder-tip pain = diaphragmatic irritation from liver or subphrenic pathology; back pain radiating to legs = cord compression); Severity (numeric or validated scale); Temporal pattern (constant vs. intermittent; breakthrough frequency).
Pain intensity scales: the Numerical Rating Scale (NRS) is the most widely used — patient rates pain intensity from 0 (no pain) to 10 (worst imaginable pain); validated across multiple languages including Hindi, Tamil, and Bengali; mild pain 1–3, moderate 4–6, severe 7–10. For patients unable to self-report (delirium, severe cognitive impairment, language barrier), behavioural pain scales are used: the Abbey Pain Scale or the PAINAD (Pain Assessment in Advanced Dementia) scale — these observe facial expression, vocalisation, body language, and consolability to estimate pain intensity. The Brief Pain Inventory (BPI) assesses both pain intensity (0–10 for worst, least, average, and current pain) and pain interference with function (interference with walking, work, mood, sleep, relationships — rated 0–10); it is the WHO-recommended comprehensive tool for cancer pain assessment in research and clinical settings and is validated in Hindi.
Pain types in cancer and their clinical differentiation:
- Nociceptive somatic pain: from bone metastases, muscle invasion, or surgical wounds; well-localised, aching, worse on movement; responds well to NSAIDs, opioids, bisphosphonates (for bone pain)
- Nociceptive visceral pain: from stretching or distension of visceral organs (hepatic capsule stretch in liver metastases, peritoneal carcinomatosis, bowel obstruction); poorly localised, colicky or constant, often referred to distant sites; responds to opioids but less predictably than somatic pain
- Neuropathic pain: from invasion or compression of nerves (brachial plexopathy from apical lung tumour, lumbosacral plexopathy from pelvic tumour, cord compression, chemotherapy-induced peripheral neuropathy); burning, shooting, electric-shock-like, allodynia (pain from non-painful stimulus), hyperalgesia; requires adjuvant analgesics beyond standard opioids
- Mixed pain: most cancer pain syndromes have both nociceptive and neuropathic components — accurate characterisation guides drug selection
Breakthrough pain (BTP) is a transient, severe exacerbation of pain occurring on a background of controlled baseline pain. It may be predictable (incident pain — triggered by movement, coughing, dressing changes) or unpredictable (spontaneous BTP). Approximately 65–70% of cancer patients with chronic pain experience BTP; its management requires a short-acting opioid rescue dose (typically 10–15% of the total daily opioid dose) available as needed, in addition to the regular around-the-clock long-acting opioid.
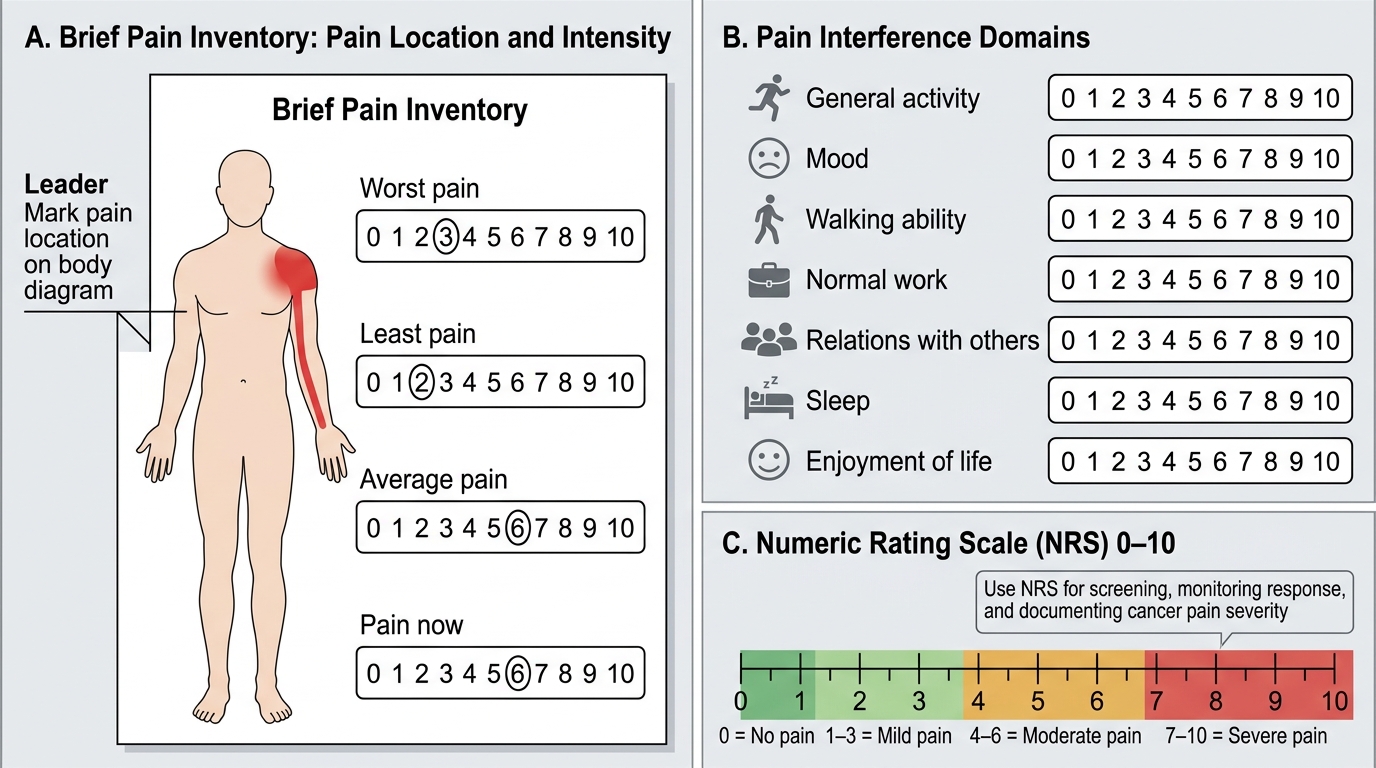
Brief Pain Inventory and Numeric Rating Scale for Cancer Pain Assessment
SELF-CHECK
A 58-year-old woman with metastatic breast cancer reports pain in the left shoulder that is described as constant, burning, and shooting down the inner forearm to the little finger. On examination, you find mild weakness of finger flexion and reduced sensation in the ulnar distribution. What type of cancer pain is this most likely to be, and what additional analgesic class beyond standard opioids is indicated?
A. Visceral pain from liver metastasis — add a laxative and antacid
B. Somatic bone pain from clavicular metastasis — add a bisphosphonate
C. Neuropathic pain from brachial plexus infiltration — add a neuropathic adjuvant (gabapentin or amitriptyline)
D. Incident pain from shoulder joint effusion — add an NSAID
Reveal Answer
Answer: C. Neuropathic pain from brachial plexus infiltration — add a neuropathic adjuvant (gabapentin or amitriptyline)
Burning, shooting pain radiating in a dermatomal pattern (inner forearm to little finger = C8/T1 territory = lower brachial plexus) with associated motor weakness and sensory loss is the classic presentation of brachial plexopathy from tumour infiltration of the brachial plexus. This is neuropathic pain, which responds poorly to opioids alone and requires adjuvant analgesics: gabapentin or pregabalin (first-line for neuropathic pain in cancer — stabilise neuronal membranes by binding voltage-gated calcium channels), or amitriptyline (tricyclic antidepressant — sodium channel and NMDA receptor modulation, good evidence for neuropathic pain; also improves sleep). Dexamethasone is also useful short-term to reduce peritumoural oedema around the plexus.
Opioid Analgesics in Cancer Pain — Indications, Dosing, and Side Effects
Opioids are the cornerstone of moderate-to-severe cancer pain management. The WHO three-step analgesic ladder, first published in 1986 and updated in 2019, remains the operational framework for cancer pain pharmacotherapy worldwide. The ladder moves from non-opioid analgesics (Step 1) through weak opioids (Step 2: tramadol, codeine) to strong opioids (Step 3: morphine, oxycodone, hydromorphone, fentanyl) — with the principle that adjuvant analgesics (co-analgesics) are added at any step for specific pain types.
The five principles of opioid prescribing in cancer pain (WHO, 2021): (1) By mouth — oral administration is preferred for chronic use; avoid the parenteral route when the oral route is available and functional; (2) By the clock — opioids should be given regularly at fixed intervals (around the clock), not on a PRN (as needed) basis — anticipating and preventing pain is more effective and requires lower total doses than treating pain after it has escalated; (3) By the ladder — step-up through the analgesic ladder; do not skip steps prematurely, but do not remain on a lower step when pain is uncontrolled; (4) For the individual — the correct opioid dose is the dose that controls pain; there is NO standard maximum dose of morphine; titrate upward by 25–30% increments until pain is controlled, observing for side effects; (5) With attention to detail — always co-prescribe a laxative (opioid-induced constipation is universal and does NOT diminish with time — unlike nausea and sedation); anticipate, monitor, and manage side effects proactively.
Oral morphine (immediate-release and sustained-release preparations) is the WHO standard strong opioid and the first-choice Step 3 analgesic for cancer pain. Starting dose for an opioid-naive adult: morphine immediate-release 5–10 mg every 4 hours (5 mg in elderly, frail, or renal-impaired patients). Once the total 24-hour opioid requirement is established (sum of all immediate-release doses used in 24 hours), convert to an equivalent once-daily or twice-daily sustained-release morphine dose. The rescue dose for breakthrough pain is 10–15% of the total daily opioid dose, available every 1–2 hours as needed. Opioid dose titration: if more than 3 rescue doses are required in 24 hours, increase the baseline dose by 25–30%.
Opioid side effects and their management:
- Constipation: universal, does not diminish with time. Co-prescribe a stimulant laxative (senna 2 tablets nocte; lactulose 15 mL BD) from day 1. Methylnaltrexone (peripherally acting mu-opioid receptor antagonist) or naloxegol are used for refractory opioid-induced constipation without reversing central analgesia.
- Nausea and vomiting: common in the first 1–2 weeks, then often tolerates. Start metoclopramide 10 mg TDS or haloperidol 1.5 mg nocte as anti-emetic cover for the first 2 weeks; antiemetics can usually be withdrawn thereafter.
- Sedation: common at initiation and after dose increases, typically resolves within 48–72 hours. If persistent: consider opioid rotation or psychostimulant (methylphenidate) in selected patients.
- Respiratory depression: the most feared but actually the least common clinically significant complication in appropriately titrated patients. Pain is a physiological antagonist to opioid-induced respiratory depression — patients titrated on opioids for pain almost never develop clinically significant respiratory depression at therapeutic doses. Risk is highest in opioid-naive patients given excessive doses, in patients with renal failure (accumulation of morphine-6-glucuronide), and in rapid dose escalation. Reversal with naloxone (0.4 mg IV, diluted and titrated in 0.04 mg increments to avoid acute withdrawal and pain precipitation).
- Opioid-induced hyperalgesia (OIH): paradoxical increase in pain sensitivity at high opioid doses — important to recognise and distinguish from undertreated pain; managed by opioid rotation.
Opioid rotation — switching from one opioid to another using equianalgesic dose tables — is indicated when: intolerable side effects limit dose escalation; opioid-induced hyperalgesia; poor pain control despite escalation (possible partial cross-tolerance). Key equianalgesic conversions:
| Opioid | Equianalgesic dose (oral) | Conversion from oral morphine |
|---|---|---|
| Morphine | 30 mg/24h | Reference |
| Oxycodone | 20 mg/24h | × 0.67 (oxycodone 30–50% more potent) |
| Hydromorphone | 7.5 mg/24h | × 0.25 |
| Transdermal fentanyl | 12 mcg/h patch per 24h | Oral morphine 30–44 mg → 12 mcg/h patch |
| Tramadol (oral) | 300 mg/24h | Weak opioid; max 400 mg/day |
When rotating, reduce the calculated equianalgesic dose of the new opioid by 25–30% (incomplete cross-tolerance) and observe for pain re-emergence or over-sedation.
NDPS Act 2014 amendment and Rule 14B in India: The Narcotic Drugs and Psychotropic Substances (NDPS) Act Amendment of 2014, combined with the Essential Medicines List (2015) and the Rules for access to oral morphine under Rule 14B, simplified opioid prescribing for palliative care. Rule 14B allows registered medical practitioners to prescribe oral morphine for patients with cancer, HIV, or other specified conditions using a single-carbon-paper prescription; it removed the complex two-form requirement that had made prescribing impractical in most states. However, implementation remains inconsistent — many district hospitals still cannot dispense oral morphine due to licensing delays or pharmacy shortages. As a clinician, you have a responsibility to know your state's specific regulations and to advocate for opioid access for your patients.
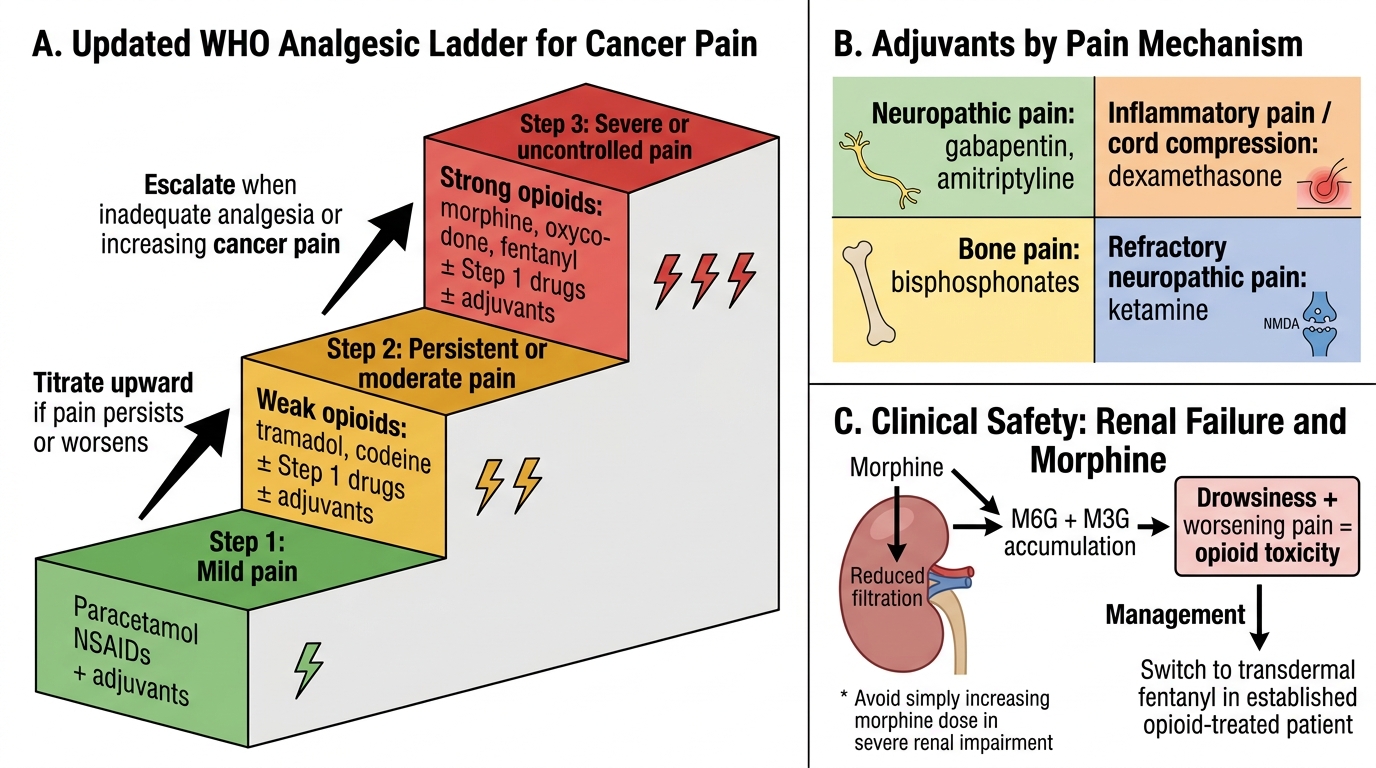
Updated WHO Analgesic Ladder for Cancer Pain
SELF-CHECK
A 70-year-old man with terminal cancer has been stabilised on oral morphine 60 mg/24h. His renal function is now deteriorating (creatinine rising, eGFR 18 mL/min/1.73m²). He is becoming more drowsy and his pain is worsening — suggesting opioid toxicity rather than inadequate analgesia. What is the most appropriate management?
A. Increase the morphine dose to overcome the apparent tolerance
B. Switch to transdermal fentanyl, which is not renally cleared and avoids morphine-6-glucuronide accumulation
C. Discontinue all opioids and use only NSAIDs
D. Add naloxone to the current morphine regimen to reverse toxicity and maintain analgesia
Reveal Answer
Answer: B. Switch to transdermal fentanyl, which is not renally cleared and avoids morphine-6-glucuronide accumulation
Morphine is metabolised to morphine-6-glucuronide (M6G, the active analgesic and respiratory-depressant metabolite) and morphine-3-glucuronide (M3G, which causes neuroexcitatory effects). Both accumulate in renal failure, causing opioid toxicity even at previously tolerated doses. Transdermal fentanyl is the preferred opioid in significant renal impairment (eGFR <30 mL/min/1.73m²) because fentanyl is primarily hepatically metabolised and its inactive metabolites are not renally cleared. Hydromorphone is an alternative. Increasing morphine would worsen toxicity. NSAIDs are contraindicated in renal failure. Naloxone will reverse analgesia and precipitate acute withdrawal and severe pain — it is reserved for life-threatening respiratory depression, not routine management of drowsiness.