Page 15 of 21
IM13.{5,13,17-19} | Cancer Pain and End of Life Care — SDL Guide (Part 2)
End-of-Life Care — Common Issues and Principles of Management
End-of-life care (EOLC) encompasses the medical, nursing, psychological, social, and spiritual care provided to patients in the final weeks to days of life, as well as bereavement support for families. The goal is not to accelerate or delay death but to ensure that the patient's dying process is as comfortable, dignified, and congruent with their values as possible. NMC competency IM13.5 requires knowledge of the common issues encountered at the end of life and the principles of their management.
Provided image
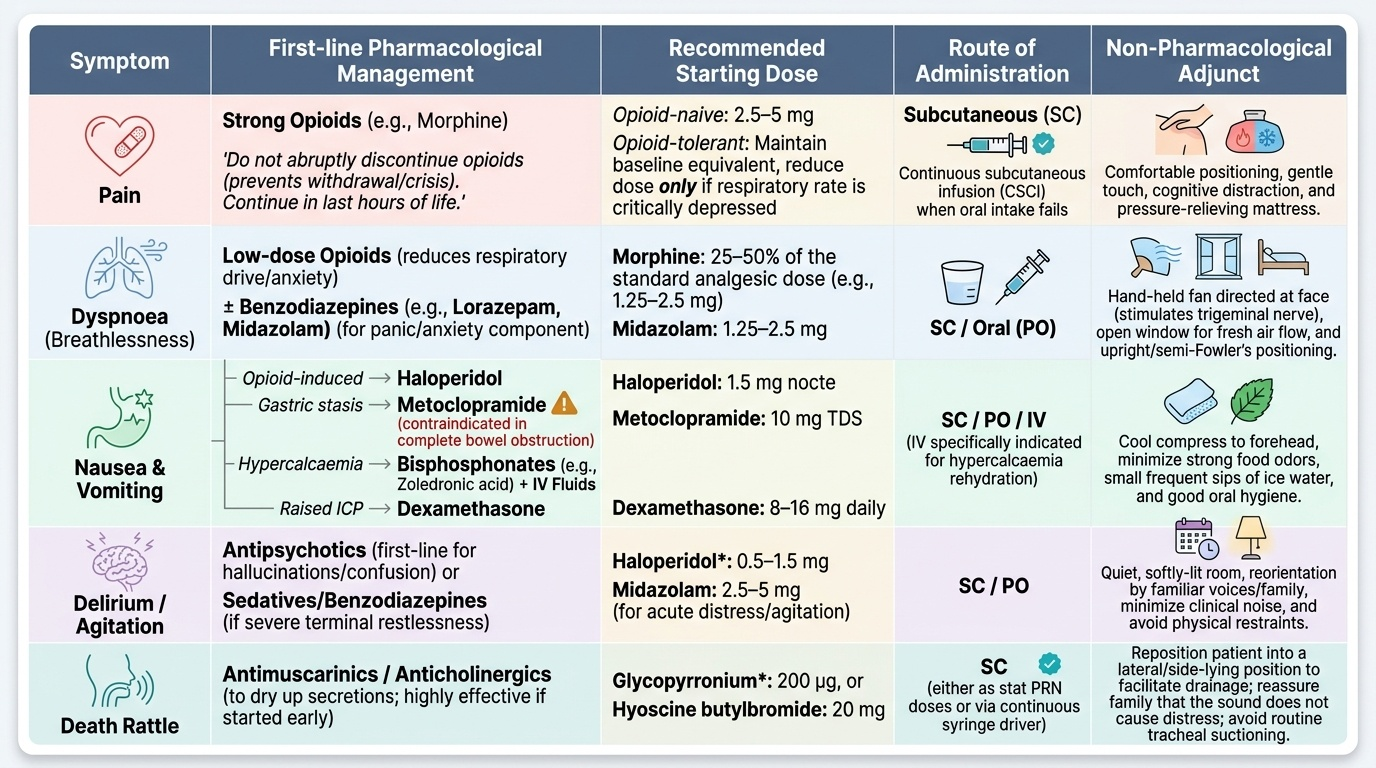
Common clinical problems in the last days of life and their management principles:
Pain: Opioid requirements often decrease in the terminal phase as oral intake fails; subcutaneous infusion of morphine via a syringe driver is a practical alternative when the oral route is no longer feasible. Never abruptly discontinue opioids in a patient who has been on them — this precipitates withdrawal and pain crisis. Continue opioids in the last hours of life; dose reductions are only made if respiratory rate is critically depressed.
Dyspnoea (breathlessness) is one of the most distressing symptoms in the terminal phase; it is common in lung cancer, pleural effusion, cardiac failure, and cachexia-related respiratory muscle weakness. Low-dose opioids are the most effective pharmacological treatment for dyspnoea — morphine reduces the respiratory drive and anxiety associated with breathlessness without causing clinically significant respiratory depression when appropriately dosed; starting with 25–50% of the analgesic morphine dose for dyspnoea is the recommendation. Benzodiazepines (lorazepam, midazolam) reduce the anxiety component. Non-pharmacological: a hand-held fan directed at the face activates nasal cool thermoreceptors and reduces the subjective perception of breathlessness; open windows; upright positioning.
Nausea and vomiting: often multifactorial in advanced cancer (constipation, opioids, hypercalcaemia, bowel obstruction, uraemia, hepatic failure, raised ICP from brain metastases). Identify the mechanism before choosing an antiemetic: (1) opioid-induced — haloperidol 1.5 mg nocte; (2) gastric stasis/functional bowel obstruction — metoclopramide (but NOT if complete mechanical obstruction); (3) hypercalcaemia — IV fluids and bisphosphonate (zoledronic acid); (4) raised ICP — dexamethasone 8–16 mg/day; (5) complete bowel obstruction — combination of octreotide (reduces secretions), cyclizine or hyoscine (reduces colic), and dexamethasone (reduces peritumoural oedema).
Delirium (terminal agitation, terminal restlessness) occurs in up to 80% of patients in the last 24–48 hours of life. It is characterised by fluctuating consciousness, disorientation, agitation, and sometimes hallucinations. In many cases terminal delirium is irreversible. Management: haloperidol 0.5–2 mg SC or IM (first-line), midazolam 2.5–5 mg SC for severe agitation or myoclonus; palliative sedation (see below) for refractory, distressing delirium. Avoid physical restraint; reassure family that agitation does not mean the patient is in uncontrolled pain (though pain must be excluded and managed).
Cachexia-anorexia syndrome in advanced cancer: characterised by involuntary weight loss, muscle wasting, fatigue, and anorexia driven by cytokine-mediated metabolic dysregulation (tumour necrosis factor-alpha, IL-6, IL-1). Nutritional supplementation does NOT reverse cancer cachexia — the metabolic pathway is not nutritional deficiency but cytokine-driven catabolism. Megestrol acetate (appetite stimulant, progestogenic), corticosteroids (dexamethasone 4–8 mg/day — short-term appetite stimulant, often used for the last weeks of life), and olanzapine (emerging evidence for cachexia) are pharmacological options for appetite stimulation. Families should be counselled that inability to eat is a consequence of advanced cancer, not its cause, and that forcing oral intake may cause distress rather than benefit.
Mouth care is a fundamental nursing and medical responsibility in the terminal phase: dry, cracked, and coated oral mucosa causes significant distress; regular mouth swabs moistened with water, oral gel, and lip balm provide comfort. Oral candidiasis (common with steroid use and immunosuppression) causes pain and should be treated with nystatin suspension or fluconazole.
Spiritual and existential suffering: patients near the end of life often face existential distress — loss of meaning, fear of the unknown, concerns about burdening family, unfinished business, religious and spiritual questions. The physician's role is to listen, acknowledge, and facilitate — not to provide answers. Chaplaincy input, psychological support, and fostering the completion of important relationships are as important as any pharmacological intervention. Dignity therapy (the Chochinov model — a narrative approach that helps patients articulate their legacy and what matters most to them) is an evidence-based psychological intervention for existential distress.
Ethical and Medico-Legal Issues in End-of-Life Care in India
End-of-life care in India exists at the intersection of medicine, law, ethics, culture, and religion. NMC competency IM13.18 requires understanding of the ethical and medico-legal issues specific to this context. The Supreme Court's 2018 judgment in Common Cause v. Union of India has resolved several longstanding legal ambiguities, but practical implementation challenges remain.
Provided image
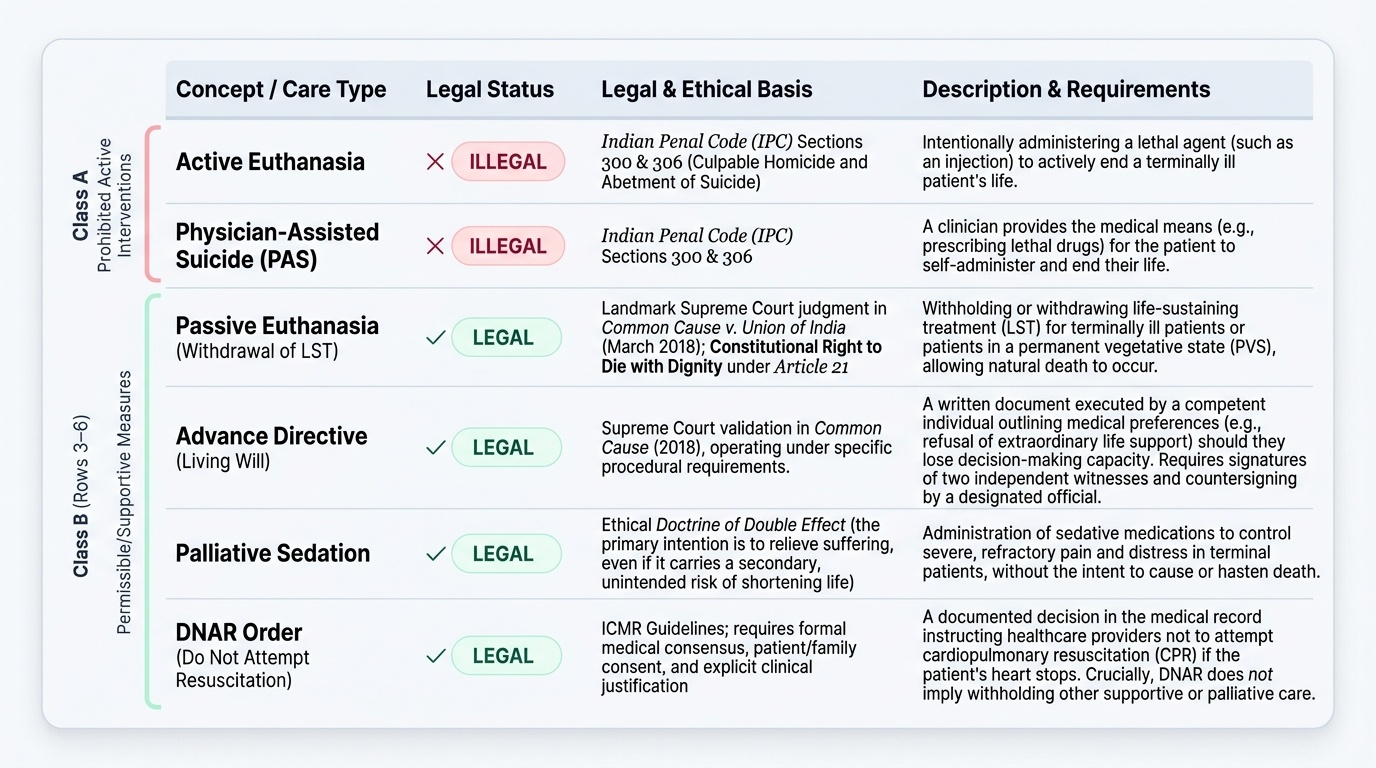
The right to die with dignity: The Supreme Court's 5-judge Constitutional Bench in Common Cause (March 2018) held unanimously that the right to live with dignity, guaranteed under Article 21 of the Constitution, necessarily includes the right to die with dignity. The Court recognised passive euthanasia (withdrawal or withholding of life-sustaining treatment for patients who are terminally ill or in a permanent vegetative state) as lawful and enforceable through the constitutional framework. Active euthanasia (intentionally administering a lethal agent to end life) and physician-assisted suicide remain illegal in India under Sections 300 and 306 IPC.
Advance directives (living wills): The Common Cause judgment validated the legal status of advance directives — written documents in which a person with decision-making capacity records their preferences about future medical treatment (specifically, the preference not to be subjected to extraordinary life-sustaining measures if they become incapacitous and terminal). The Court prescribed specific procedural requirements: the directive must be signed by the person in the presence of two independent witnesses and countersigned by the jurisdictional first-class magistrate or a gazetted officer. In practice, these procedural requirements are burdensome; simplified implementation frameworks are being developed under the National Health Policy 2017 provisions.
Cardiopulmonary resuscitation (CPR) — DNAR orders: 'Do Not Attempt Resuscitation' (DNAR) orders — or equivalently, 'Allow Natural Death' (AND) orders — must be discussed explicitly with the patient (and family if the patient lacks capacity or chooses to involve family) and documented clearly in the medical record with the clinical rationale, the patient's consent or the best-interest decision, and the treating physician's name and signature. A DNAR order does not mean withholding other care — it applies only to CPR in the event of cardiopulmonary arrest; all other treatments continue unless separately decided otherwise.
Opioid prescribing and the 'doctrine of double effect': The doctrine of double effect — drawn from Catholic bioethics but broadly accepted in secular medical ethics — holds that an action with two possible effects (one good, one potentially harmful) is ethically permissible if: the action itself is not intrinsically evil, the intended effect is the good one, the harmful effect is foreseen but not intended as a means to the good effect, and the good effect is proportionate to any harm. In palliative care, this doctrine justifies using opioids at doses sufficient to relieve pain even if they carry a theoretical risk of hastening death — because the intention is analgesia, not death, and the benefit (relief of suffering) is proportionate. In clinical practice, appropriately titrated opioids do NOT shorten life (several studies show the opposite — better pain control extends survival); the doctrine of double effect is invoked pre-emptively to resolve prescribers' fears, not to justify a documented risk.
Palliative sedation (previously called terminal sedation) refers to the deliberate reduction of consciousness in a patient with intractable, refractory suffering in the terminal phase. It is ethically distinct from euthanasia because: the intent is to relieve intolerable suffering, not to cause death; the lowest dose of sedative that relieves suffering is used; there is no intention to hasten death. Midazolam 2.5–10 mg SC or phenobarbitone are the most commonly used agents. Proportionate palliative sedation is endorsed by IAPC and consistent with the doctrine of double effect and Indian law.
Truth-telling and prognostic disclosure: Indian cultural norms frequently favour protection of the patient from a cancer diagnosis (the family is told first; the patient may not be told at all). While respecting cultural norms is important, the physician has a duty to determine the patient's own preferences about disclosure — 'Would you like me to explain your medical situation in full, or would you prefer that I discuss it with your family members and how much you would like me to share with you?' Many patients who are 'protected' from the diagnosis are in fact aware and are protecting the family in return. Non-disclosure denies patients the opportunity to complete advance directives, settle affairs, and make autonomous treatment decisions — ethically, the patient's autonomy should be the anchor even when cultural norms push toward protection.
SELF-CHECK
A 72-year-old man with end-stage pancreatic cancer is admitted with severe pain, delirium, and respiratory distress. He has no advance directive. He is unconscious and cannot communicate his wishes. His family states he had previously expressed a desire 'not to be kept alive on machines'. A DNAR order is discussed. Which statement BEST reflects the ethical and legal position in India regarding this DNAR decision?
A. A DNAR order requires active euthanasia and is illegal in India under all circumstances
B. A DNAR order can only be implemented if there is a written advance directive signed before a magistrate
C. A DNAR order for a terminally ill patient who expressed a wish not to be kept alive on machines can be documented based on best-interest principles and family report of prior expressed wishes — consistent with the Common Cause 2018 Supreme Court judgment
D. The family has no legal standing in DNAR decisions; only the treating physician decides
Reveal Answer
Answer: C. A DNAR order for a terminally ill patient who expressed a wish not to be kept alive on machines can be documented based on best-interest principles and family report of prior expressed wishes — consistent with the Common Cause 2018 Supreme Court judgment
The Common Cause v. Union of India (2018) Supreme Court judgment recognised that withholding or withdrawing life-sustaining treatment (including CPR) for terminally ill patients is lawful passive euthanasia, consistent with the constitutional right to die with dignity. In the absence of a formal advance directive, decisions are made on a best-interest basis, taking into account previously expressed wishes (which the family has relayed), the patient's current clinical condition, the prognosis, and the clinical team's assessment. DNAR orders are NOT active euthanasia — they permit natural death; they are ethically and legally distinct from active killing. The family's report of the patient's prior expressed wish is a legitimate input into the best-interest decision, though it does not replace clinical judgment.
Self-Assessment: Integrating Palliative Care Competencies
This self-assessment section integrates the clinical, pharmacological, and ethical content of this module. Work through each question before reviewing the analysis.
Q1: Opioid rotation scenario
A patient is on oral morphine 120 mg/24h with good pain control but is experiencing severe, dose-limiting nausea and vomiting that has not responded to antiemetics. His renal function is normal. He needs opioid rotation to oxycodone. Calculate the starting dose of oral oxycodone.
Calculation: Oral morphine 120 mg/24h → oral oxycodone conversion using equianalgesic ratio (oxycodone is approximately 1.5× more potent): 120 ÷ 1.5 = 80 mg/24h oxycodone equianalgesic. Reduce by 25–30% for incomplete cross-tolerance: 80 × 0.75 = 60 mg/24h oxycodone. Starting dose: oxycodone 30 mg BD (modified-release) with a rescue dose of 5–7.5 mg immediate-release oxycodone PRN for breakthrough pain (10% of daily dose).
Q2: Anticipatory prescribing
A 68-year-old woman with end-stage ovarian cancer is in the terminal phase at home under a palliative home care team. Her swallowing is deteriorating. As her treating physician, what medications should be prescribed anticipatorily ('just in case' medications) to ensure comfort during the last hours to days of life?
Analysis: Anticipatory prescribing for the terminal phase should always include medications for the five most likely distressing symptoms: (1) Pain: morphine 2.5–5 mg SC PRN 4-hourly; (2) Agitation/delirium: midazolam 2.5–5 mg SC PRN or haloperidol 1–2.5 mg SC PRN; (3) Dyspnoea: morphine 2.5 mg SC PRN (25–50% of analgesic dose) — consider lorazepam sublingual if patient is still able to take sublingual medications; (4) Nausea: haloperidol 1.5 mg SC PRN or cyclizine 50 mg SC PRN; (5) Respiratory secretions (death rattle): glycopyrronium 0.2 mg SC PRN (anticholinergic, reduces secretions; does NOT reduce consciousness unlike scopolamine which is CNS-active). These six prescriptions are written in advance so that the home carer or community nurse can administer them promptly without needing to contact a prescriber at 3 am.
Q3: Ethical reasoning
A family of a 55-year-old man with terminal lung cancer insists that his physician not tell him his prognosis 'because he will lose hope and give up'. The patient has previously asked you privately: 'Doctor, am I going to be able to make it to my daughter's marriage in 4 months? I need to know the truth.' How do you handle this conflict?
Analysis: The patient has explicitly invoked his right to information — he has asked for the truth. His autonomy takes precedence over the family's protective impulse. The ethical approach: speak with the patient privately, acknowledge that this is a difficult question, and provide honest but compassionate prognostic information — 'Based on your test results, I am concerned that 4 months may be a very optimistic timeline; many patients in your situation would be managing one to three months. I cannot be certain, but I think we need to plan for this possibility so that you can focus your energy on what matters most to you, including your daughter's wedding.' Simultaneously, acknowledge the family's care and involve them appropriately. Document the conversation. The 'protection' offered by non-disclosure is often the physician's and family's protection from a difficult conversation, not the patient's protection from suffering.
Cancer Pain Management by Pain Type
CLINICAL PEARL
Three high-yield clinical pearls for palliative and end-of-life care:
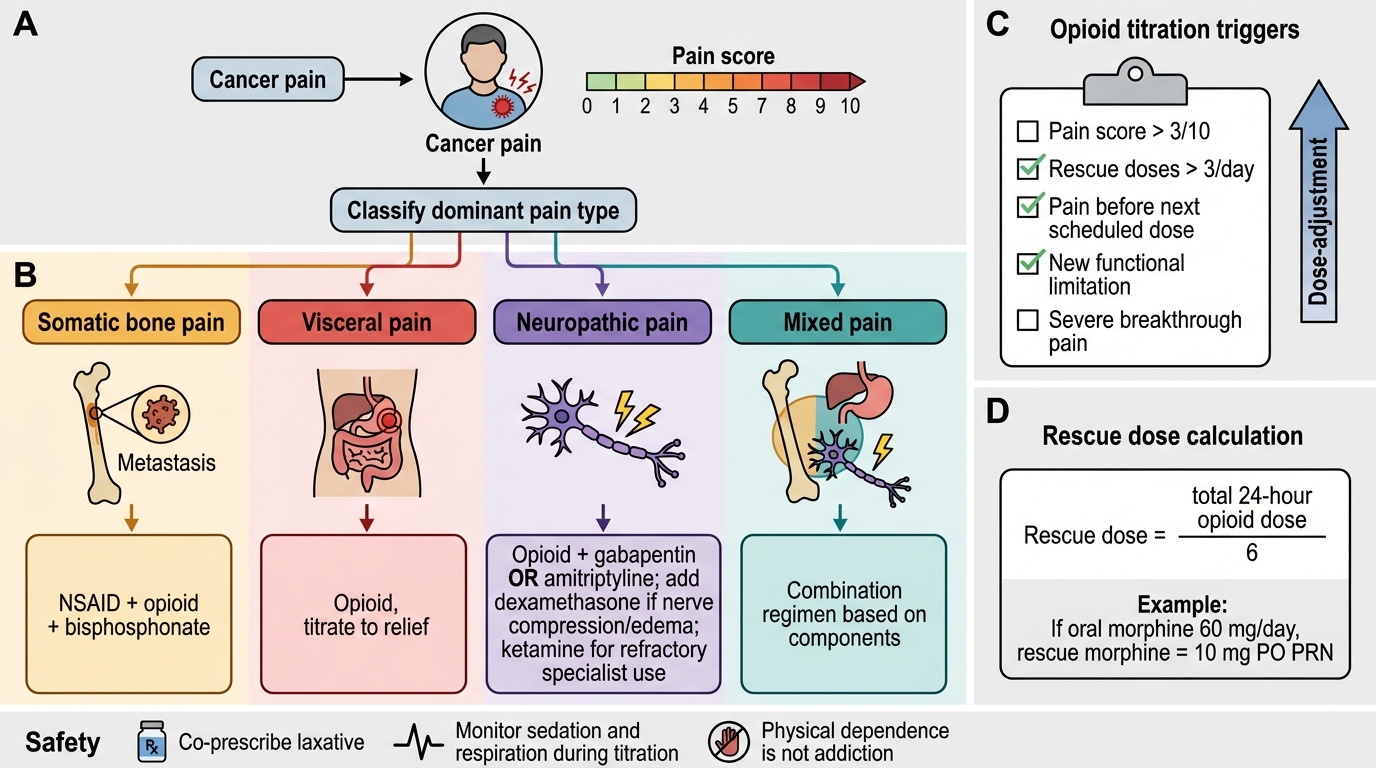
First, opiophobia kills. The single most common reason for undertreated cancer pain in India is physician opiophobia — the unfounded fear that prescribing morphine will kill the patient or create addiction. Evidence is clear: (1) appropriately titrated opioids in cancer patients do NOT cause respiratory depression at therapeutic doses; (2) addiction (psychological dependence with drug-seeking behaviour) is extremely rare in cancer patients using opioids for genuine pain; (3) physical dependence (physiological adaptation requiring gradual dose reduction when stopping) is expected and normal — it is NOT addiction. Prescribe morphine when it is indicated. The legal framework under Rule 14B of the NDPS Act supports you.
Second, laxatives must be co-prescribed with every opioid. Opioid-induced constipation is universal, does not improve with time (unlike nausea and sedation), and causes severe suffering including faecal impaction, overflow diarrhoea, and bowel obstruction. Starting senna or lactulose at opioid initiation is mandatory, not optional — and the dose increases proportionally with the opioid dose.
Third, death rattle does NOT indicate respiratory distress in the patient — it is caused by pooled secretions in the hypopharynx vibrating with respiration in a semi-conscious patient who has lost the ability to cough or swallow. It is distressing to relatives (who interpret it as suffering) but not typically distressing to the patient. Management is primarily repositioning (lateral or semi-prone to drain secretions by gravity) and glycopyrronium SC to reduce secretion production. Family education about its meaning is as important as the pharmacological intervention.