Page 5 of 19
IM16.{4-5,7} | Diarrheal Disorder Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit, document, and present a complete and structured history in a patient with diarrhoea including the seven domains: onset/duration, stool characterisation, associated symptoms, dietary history, travel and epidemiological history, sexual history, and medication/systemic history
- Perform and document a systematic physical examination in a patient with diarrhoea including assessment of dehydration severity (WHO Plan A/B/C signs), abdominal examination, perianal examination, and targeted extraintestinal examination
- Generate a prioritised differential diagnosis from clinical data using a structured framework based on duration, mechanism, risk factors, and must-not-miss diagnoses
INSTRUCTIONS
This module develops the clinical skill of structured assessment in diarrhoeal disorders — history taking, physical examination, and differential generation. These are not passive reading skills. For maximum benefit, after each content section, close the module and practise the elicitation domains on a simulated or real patient encounter before returning to review. The self-assessment scenarios at the end require you to apply reasoning rather than recall.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 43 — Diarrhoea and Constipation (textbook)
- API Textbook of Medicine, 10th ed., Ch. 7 — Gastroenterology (textbook)
- Davidson's Principles & Practice of Medicine, 24th ed., Ch. 24 — Alimentary Tract (textbook)
- WHO Pocket Book of Hospital Care for Children — Diarrhoea Assessment and Treatment (guideline)
- British Society of Gastroenterology Guidelines on Acute Diarrhoea, 2020 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients arrive at your outpatient clinic on the same afternoon. The first is a 22-year-old college student who had four watery stools yesterday after a canteen lunch; he looks entirely well and is checking his phone. The second is a 55-year-old woman who has had loose stools with occasional blood and mucus for the past 14 months, accompanied by weight loss of 12 kg and persistent lower abdominal cramping. She looks pale and cachectic, and her daughter mentions she has been avoiding food for fear it will worsen her symptoms. Both patients say they have 'diarrhoea.' Your job begins not with a stool culture or a colonoscopy, but with a focused, structured clinical evaluation — history and physical examination — that will do two things: determine whether the first patient needs any investigation at all, and generate a differential diagnosis narrow enough to guide the first investigation for the second. The art of clinical evaluation in diarrhoeal disorders is knowing exactly which questions to ask, in which order, and what physical signs to actively look for. This module builds that skill.
WHY THIS MATTERS
In a country where laboratory infrastructure varies dramatically from a tertiary referral hospital to a primary health centre in a remote taluk, the clinical evaluation — history and physical examination — must do more diagnostic work than it would in a resource-rich setting. For IM16.4 and IM16.5, you are expected to perform, document, and present a complete and appropriate assessment of a patient with diarrhoea including travel history, sexual history, dietary history, and abdominal examination. For IM16.7, you are expected to generate and prioritise a differential diagnosis from the clinical data. These are Skills with Hands (SH) and Knowledge with Application (KH) competencies — meaning the examination can ask you to role-play the history with a simulated patient, demonstrate an abdominal examination, or work through a clinical vignette and explain your diagnostic reasoning. Both scenarios require not just memory of what to ask, but internalised skill in structuring the encounter.
RECALL
Before proceeding, activate your knowledge of the four diarrhoeal mechanisms (from the Diarrheal Disorder Foundations SDL): secretory (large-volume watery, persists with fasting, no blood, low osmotic gap — prototype cholera), osmotic (ceases with fasting, bloating, high osmotic gap), inflammatory/invasive (blood/mucus, fever, tenesmus, faecal leucocytes — prototype dysentery from Shigella or amoebiasis), and malabsorptive (fatty floating stools, weight loss, nutritional deficiencies — prototype coeliac, giardia). Also recall the duration classification: acute <2 weeks, persistent 2–4 weeks, chronic >4 weeks. Every question you ask in the history is designed to map the patient's symptoms onto one of these mechanisms and one of these duration categories — this mapping is what generates the differential diagnosis. The physical examination then adds sign-level data (hydration status, abdominal tenderness, hepatomegaly, anal findings) that either supports the working diagnosis or raises a competing hypothesis.
Taking the History: Clinical Indication and Approach
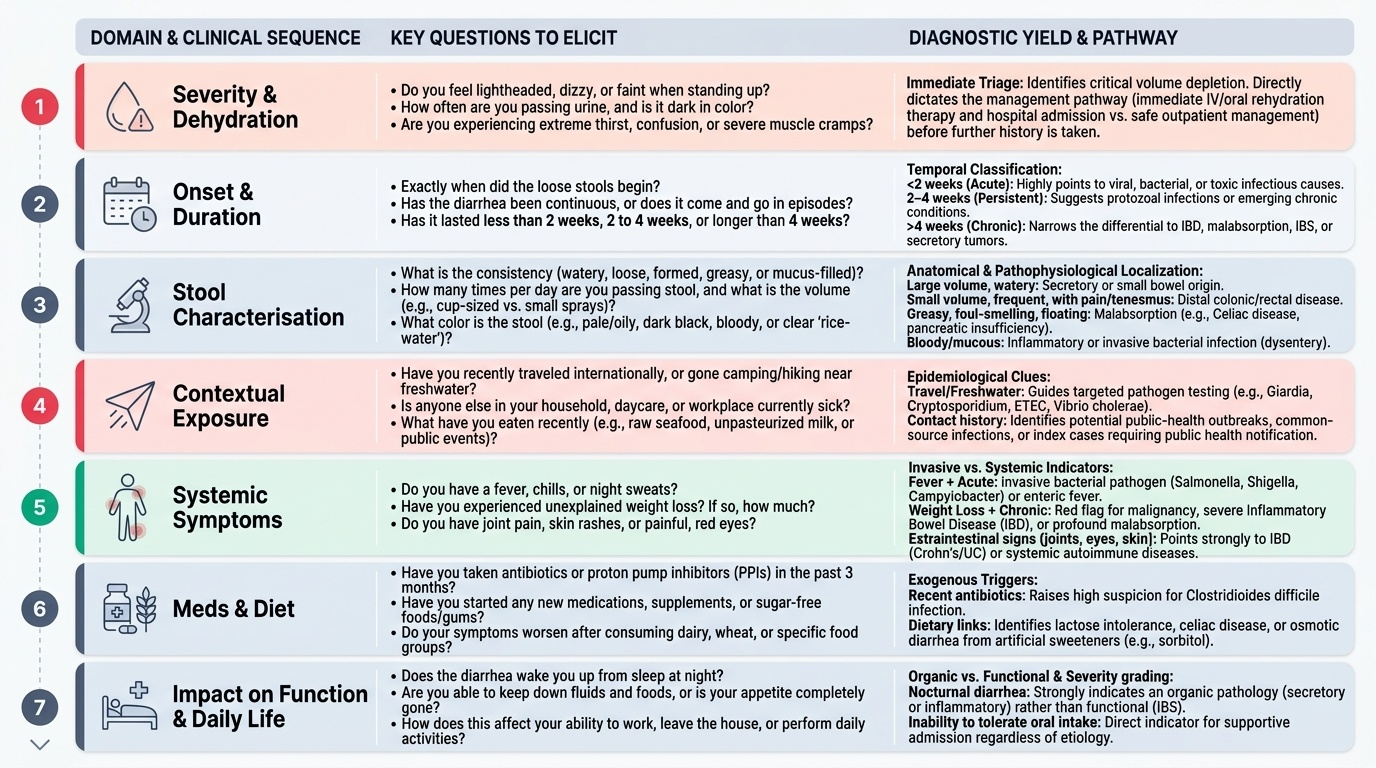
The clinical evaluation of a patient with diarrhoea begins with understanding what you are trying to achieve with the history: you are not collecting facts in a vacuum, but building a clinical narrative that tests each of the four mechanisms against the patient's actual experience. A well-taken history in a diarrhoeal presentation has seven structured domains, each yielding specific diagnostic signal. The order in which you elicit these domains is itself a clinical skill — start with the most time-sensitive assessment (severity and dehydration), then move to characterisation, then contextual risk factors, then systemic symptoms. This order ensures that a critically dehydrated patient is not kept sitting through an elaborate dietary history before hydration is initiated.
Provided image
The indication for a thorough history is broader than it might seem. In acute diarrhoea, most episodes are self-limiting and infectious, and the history's primary role is to identify the minority that need antibiotics (dysentery, cholera, enteric fever), that are part of a public-health outbreak (common source, index case), or that have features suggesting a more sinister non-infectious cause. In persistent and chronic diarrhoea, the history is the primary tool for separating the many possible aetiologies — IBD, malabsorption, IBS, secretory tumour, parasitic infection — that require radically different investigation and treatment. The history must also elicit the impact of diarrhoea on daily function, fluid intake, and appetite — because this directly informs the management plan (hospital admission vs outpatient management, dietary advice, nutritional support).
The seven domains of the diarrhoea history, and the diagnostic signal each yields:
- Onset and duration: First, is this acute (<2 wk), persistent (2–4 wk), or chronic (>4 wk)? Duration immediately narrows the differential — an acute 2-day watery illness is almost always infectious; a 6-month history of loose stools with weight loss requires chronic-aetiology thinking.
- Stool characterisation: (a) Frequency — how many stools per day? (b) Volume — large (cup to litre per episode) suggests secretory/small bowel origin; small, frequent, pain-accompanied suggests large bowel/distal colonic disease. (c) Consistency — watery/loose vs formed with blood. (d) Colour — rice-water (cholera), yellow-green (rotavirus, ETEC), pale/fatty (malabsorption), bright red blood (lower GI, dysentery), dark/tarry (upper GI, melaena), mucus-rich (IBD, amoebiasis). (e) Blood and/or mucus — present = dysentery/invasive/inflammatory. (f) Odour — foul-smelling fatty stools = steatorrhoea.
- Associated symptoms: Fever (invasive bacterial, inflammatory); nausea/vomiting (gastroenteritis, food poisoning — particularly with rapid onset within hours of eating); abdominal pain — character, site, radiation, relation to defaecation (IBS: pain relieved by defaecation; IBD: often persists; small bowel colic is peri-umbilical; colonic pain is lower abdominal); tenesmus (rectal urgency — suggests rectal/distal colonic inflammation); rectal bleeding; bloating and flatulence (malabsorption, SIBO, osmotic).
- Dietary history: What did the patient eat in the 6–72 hours before onset? Common implicated foods: raw or undercooked poultry (Campylobacter, Salmonella), shellfish (Vibrio, norovirus), raw eggs (Salmonella), reheated rice (Bacillus cereus — rapid-onset vomiting within 1–6 hours), dairy products (Listeria, Yersinia), unwashed vegetables, street food. History of consuming food at a large gathering or shared meal (point-source outbreak). Lactose intake in a patient with known lactase deficiency. Sorbitol/sugar-free products (osmotic diarrhoea). Change in diet including new fruits, fibre, or laxatives.
Governing Principles: Epidemiological, Travel, Sexual, and Systemic History
The second half of the diarrhoeal history extends beyond stool characterisation into epidemiological, occupational, travel, sexual, and systemic domains that are frequently underemphasised in bedside teaching but carry high diagnostic weight in specific clinical scenarios. Missing these questions in an OSCE or in clinical practice represents an incomplete history that leaves important aetiologies unexamined and may lead to delayed diagnosis of conditions that require specific treatment. These domains are particularly important because they often hold the diagnostic key when initial stool examination returns negative or inconclusive results. In a country as epidemiologically diverse as India — where cholera and typhoid persist in certain districts, where HIV prevalence remains elevated in specific populations, and where patterns of sexual behaviour and occupational exposure carry distinct pathogen risks — the contextual history is never a formality. It is a structured clinical search for the specific exposure that will narrow your differential from 20 possibilities to 3.
Travel history is essential in patients with diarrhoea because the pathogen spectrum changes dramatically with geography. In India, the key travel contexts are:
- Pilgrimages and mass gatherings (Kumbh Mela, Amarnath Yatra, Char Dham): crowded conditions, shared water sources, potential cholera/enteric fever outbreaks
- Rural-urban migration or travel: exposure to water-borne pathogens in areas with inadequate sanitation — cholera, amoebiasis, giardia, enteric fever
- Tribal and forested areas: helminthic infestations, tropical sprue
- International travel to sub-Saharan Africa, Southeast Asia, or South America: Campylobacter, Cryptosporidium, cyclosporiasis, cholera; traveller's diarrhoea (predominantly ETEC)
Ask specifically: where, how long, food and water sources consumed, healthcare access during travel.
Sexual history is a sensitive but clinically necessary component of the diarrhoeal history in the following contexts:
- Men who have sex with men (MSM): increased risk of Shigella, gonorrhoeal proctitis, LGV (lymphogranuloma venereum — Chlamydia trachomatis serovars L1–L3 causing severe proctitis in MSM), amoebiasis (sexual transmission possible)
- HIV risk factors: HIV-positive individuals have a specific diarrhoeal differential — Cryptosporidium (which is self-limiting in immunocompetent patients but causes life-threatening chronic diarrhoea in HIV when CD4 <200 cells/μL), Microsporidia, CMV colitis, MAC (Mycobacterium avium complex), and Isospora belli. Always document HIV status and CD4 count if known. In India, where HIV prevalence is higher in certain populations (sex workers, truck drivers, MSM), and where antiretroviral therapy (NACO/ART programme) may have complicated adherence issues, this history is particularly important.
- Rectal intercourse: risk of proctitis from gonorrhoea, herpes simplex, Chlamydia — presenting with rectal pain, bleeding, mucus discharge
Occupational and social history:
- Healthcare worker: C. difficile exposure from patient contact
- Childcare/nursery worker or parent of young children: rotavirus, norovirus exposure
- Food handler: Salmonella, Staph aureus food poisoning
- Farmer or animal handler: Cryptosporidium (from calves), Brucellosis (presenting with diarrhoea), Yersinia
- Immunocompromised household member or patient: opportunistic pathogens
Antibiotic and medication history: Recent broad-spectrum antibiotics (especially clindamycin, fluoroquinolones, cephalosporins) → Clostridioides difficile (C. diff): watery to bloody diarrhoea, characteristic foul odour, fever, lower abdominal pain, often in hospital or post-hospital setting. Metformin: watery diarrhoea, dose-related, particularly at initiation. NSAIDs: can cause collagenous or lymphocytic colitis. Laxative abuse: osmotic diarrhoea. Proton pump inhibitors (rare). Always take a complete medication history including traditional/herbal remedies — certain Ayurvedic preparations contain laxative compounds (senna, cascara).
Systemic review and past medical history: Thyroid disease (hyperthyroidism causes diarrhoea — high-output, watery); diabetes mellitus (autonomic neuropathy causes diabetic enteropathy — alternating constipation and diarrhoea, particularly nocturnal); inflammatory arthritis, uveitis, skin lesions (extra-intestinal manifestations of IBD); previous abdominal surgery (post-gastrectomy dumping syndrome, short bowel syndrome, bile-acid diarrhoea after ileal resection); family history of coeliac disease, colorectal cancer, or IBD.
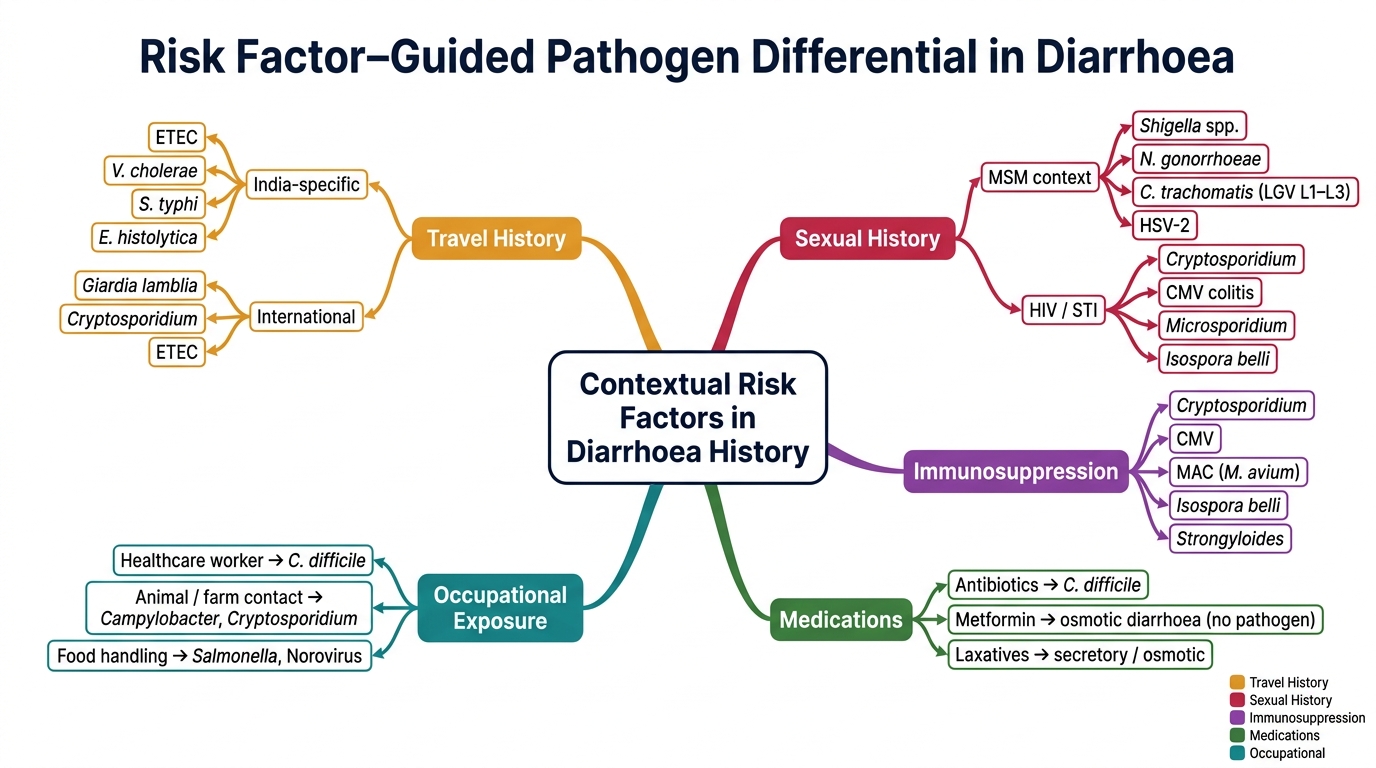
Risk Factor–Pathogen Mind Map in Diarrhoea History
SELF-CHECK
A 28-year-old man presents with severe bloody proctitis — rectal pain, mucoid bloody discharge, and tenesmus for 6 weeks. He is a healthcare worker and has not travelled recently. He discloses he has sex with men and has had three partners in the past year. HIV test is negative. Which pathogens should be specifically added to the differential diagnosis based on his sexual history?
A. Vibrio cholerae and Entamoeba histolytica
B. Shigella, Chlamydia trachomatis (LGV serovars), and Neisseria gonorrhoeae
C. Rotavirus and Cryptosporidium parvum
D. Clostridioides difficile and Campylobacter jejuni
Reveal Answer
Answer: B. Shigella, Chlamydia trachomatis (LGV serovars), and Neisseria gonorrhoeae
In a man who has sex with men (MSM) with proctitis, the differential must include sexually transmitted causes of proctitis: Shigella (MSM outbreaks documented globally and in India), Neisseria gonorrhoeae (gonococcal proctitis), Chlamydia trachomatis serovars L1-L3 (lymphogranuloma venereum, LGV — causing severe granulomatous proctitis in MSM; important to test for because it requires 3 weeks of doxycycline, not the standard 1-week regimen), and herpes simplex virus. Entamoeba histolytica can also be sexually transmitted among MSM. Cholera, rotavirus, and Cryptosporidium are not sexually transmitted. C. difficile is hospital-associated and not MSM-specific.
Physical Examination: Technique and Systematic Approach
Physical examination in a patient with diarrhoea serves three purposes: assess severity (dehydration, haemodynamic compromise), localise the disease (signs that suggest small bowel vs large bowel, inflammatory vs non-inflammatory), and identify systemic signs of the underlying aetiology (hepatomegaly suggesting amoebic liver abscess, lymphadenopathy suggesting enteric fever, perianal disease suggesting Crohn's, skin and joint manifestations suggesting IBD). A structured examination proceeds from general assessment to vital signs to a focused abdominal and perianal examination, with targeted extraintestinal examination guided by the differential diagnosis generated from the history. This sequence should be practised as a reproducible routine — in an OSCE, the examiner evaluates not just what you find but whether you perform each component systematically.
General examination and vital signs (always performed first — non-negotiable):
- Consciousness and orientation: altered sensorium in severe dehydration (Plan C) or sepsis
- Nutritional status: wasting, muscle atrophy, sunken eyes, skin fold tenting — chronic disease vs acute dehydration
- Pallor: anaemia suggests chronic blood loss (IBD), malabsorption (iron/B12 deficiency), or haemolytic anaemia (HUS from STEC/E. coli O157:H7)
- Jaundice: amoebic liver abscess (rare), hepatitis A presenting with diarrhoea (early), cholestasis
- Temperature: fever indicates invasive bacterial diarrhoea, IBD flare, or enteric fever (may be bradycardia-relative to fever height in enteric — Faget's sign)
- Pulse rate and character: tachycardia = dehydration or sepsis; weak/thready = severe dehydration/shock
- Blood pressure (both lying and standing): orthostatic hypotension (drop ≥20 mmHg systolic or ≥10 mmHg diastolic on standing) = significant dehydration (Plan B–C)
- Respiratory rate: tachypnoea in metabolic acidosis (Kussmaul respiration in severe dehydration)
Dehydration assessment (WHO physical signs — integrate with history of fluid loss):
- Eyes: sunken orbits — moderate-severe dehydration
- Mucous membranes: dry mouth/tongue — dehydration
- Skin turgor: pinch the skin of the lateral abdomen or forearm → timing of recoil: immediate = normal; 1–2 seconds = some dehydration; >2 seconds = severe dehydration. Note: less reliable in elderly and obese patients
- Capillary refill: press fingernail for 5 seconds; normal = refill <2 seconds
- Fontanelle: in infants — sunken = dehydration; bulging = raised ICP (meningitis differential)
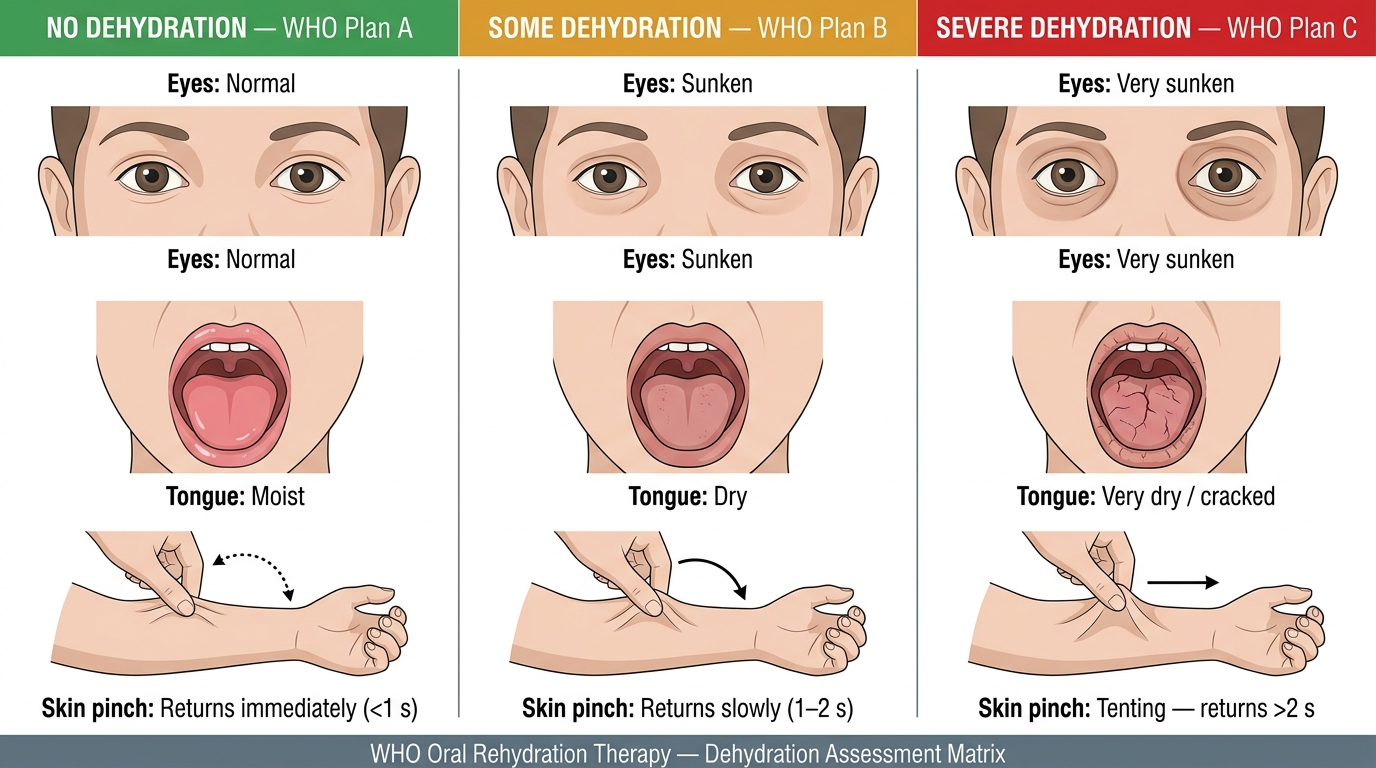
Dehydration Signs and WHO Rehydration Plan Classification (Plans A, B, C)
Abdominal examination — systematic sequence:
1. Inspection: distension (gaseous = malabsorption/SIBO; faecal = obstruction; ascites with chronic disease), visible peristalsis, surgical scars (prior abdominal surgery = short bowel risk), hernias, visible pulsations
2. Auscultation: bowel sounds — hyperactive ('gurgling') in acute enteritis; absent in ileus, severe electrolyte imbalance (hypokalaemia from diarrhoea-induced potassium loss)
3. Palpation: (a) superficial then deep; (b) guarding/rigidity = peritonism (perforation risk in severe colitis — emergency); (c) tenderness — right iliac fossa = Crohn's terminal ileitis OR Yersinia ileitis OR appendicitis OR enteric fever; left iliac fossa = UC, sigmoid diverticulitis, EIEC/Shigella; diffuse = severe colitis, peritonitis; (d) hepatomegaly — amoebic liver abscess is tender (distinguish from non-tender hepatic enlargement); splenomegaly — enteric fever, kala-azar
4. Percussion: dullness shifting (ascites from hypoalbuminaemia in protein malabsorption or protein-losing enteropathy), tympanic distension
5. Special signs: palpable loop of bowel (Crohn's stricture palpable in right iliac fossa); succussion splash (delayed gastric emptying, rare)
Perianal inspection (essential in any patient with chronic diarrhoea or bloody stool):
Inspect the perianal skin: skin tags, fissures, fistula openings (external openings of fistulous tracts), external haemorrhoids, perianal abscess. Perianal fistulae and skin tags in a young patient with diarrhoea strongly suggest Crohn's disease — they may appear years before the bowel symptoms are attributed to IBD. Perform digital rectal examination (DRE): assess anal tone (reduced in neurological disease), tenderness, rectal mass (carcinoma, polyp), rectal mucosa (cobblestone feel in proctitis), and obtain stool on the examining glove (colour, blood, mucus).
Targeted extraintestinal examination by differential:
- IBD suspicion: examine joints (arthritis — peripheral, non-deforming), eyes (uveitis, episcleritis — slit lamp if suspicious), skin (erythema nodosum = tender, red, indurated nodules over anterior shin; pyoderma gangrenosum = painful undermined ulcers)
- Enteric fever (typhoid): rose spots (faint salmon-pink macules on trunk, 2–4 mm, found in 10–20%), relative bradycardia, splenomegaly, coated tongue
- Malabsorption/vitamin deficiency: examine mucous membranes (angular stomatitis, glossitis — B-vitamin deficiency), hair (brittle, sparse — protein deficiency), nails (koilonychia — iron deficiency), skin (hyperpigmentation in pellagra, Addisonian changes), neurology (peripheral neuropathy B12/E, SACD for B12)
- Amoebic liver abscess: right hypochondrial tenderness, hepatomegaly, intercostal tenderness (point tenderness between ribs over the liver), absence of jaundice (characteristic — liver function is usually preserved)