Page 6 of 19
IM16.{4-5,7} | Diarrheal Disorder Clinical Evaluation — SDL Guide (Part 2)
Interpretation: Generating and Prioritising the Differential Diagnosis
The differential diagnosis generation process in diarrhoeal disorders is not a list-memorisation exercise — it is a pattern-matching process that takes the clinical data (mechanism signals from history + physical examination findings) and maps them to the most probable diagnostic categories. The skill being assessed in IM16.7 is the ability to not just generate the differential but to prioritise it: to identify the most likely diagnosis first, followed by the next-most-likely, and to flag the most dangerous possibilities even if less probable ('must-not-miss' diagnoses). A clinically sound differential has three tiers: most probable, alternative diagnoses (higher prior probability of some other common condition), and must-not-miss (conditions that would be harmful to delay treatment of).
Framework for differential generation in diarrhoea: answer these questions in sequence
Q1: Is this acute (<2 wk), persistent (2–4 wk), or chronic (>4 wk)?
- Acute → infectious differential dominates (viral, bacterial, parasitic)
- Persistent → parasitic more probable (Giardia, Cryptosporidium, Cyclospora); post-infectious IBS; early inflammatory
- Chronic → non-infectious differential essential (IBD, coeliac, IBS, secretory tumour, parasitic, malabsorption)
Q2: Is this secretory/watery or inflammatory/bloody?
- Watery without blood → secretory or osmotic
- Acute + watery + epidemic context → cholera, ETEC, norovirus
- Acute + watery + travel → traveller's diarrhoea (ETEC), Cryptosporidium
- Watery + ceases with fasting → osmotic (lactase deficiency, laxative abuse)
- Chronic + watery + nocturnal → secretory neoplasm (VIPoma, carcinoid, microscopic colitis)
- Bloody with mucus → inflammatory/invasive
- Acute + bloody + fever → Shigella (most virulent, dysentery), EIEC, Campylobacter, Salmonella
- Acute + bloody + no fever → STEC/E. coli O157:H7 (haemolytic uraemic syndrome risk — order CBC and renal function urgently), E. histolytica amoebiasis
- Chronic + bloody + weight loss → IBD (Crohn's or UC), colorectal carcinoma (age >40), TB colitis (India)
Q3: Are there clues to a specific systemic diagnosis?
- Young patient + perianal fistula + right iliac fossa pain → Crohn's disease
- Patient >40 + rectal bleeding + weight loss + family history of CRC → colorectal cancer until proven otherwise (must-not-miss)
- Diarrhoea + heart failure + liver disease + flushing + wheeze → carcinoid syndrome
- Severe diarrhoea + mucosal burns + hypotension after antibiotic course → C. difficile colitis (pseudomembranous colitis)
- Immunocompromised + watery diarrhoea + no pathogen on routine stool culture → Cryptosporidium, Microsporidia, CMV
Q4: Apply the 'must-not-miss' filter regardless of prior probability:
- Amoebic liver abscess (fever + right hypochondrial tenderness + travel/endemic area history) — missed = spontaneous rupture, mortality
- Enteric fever with diarrhoea — missed = intestinal perforation at 3rd week, endocarditis
- Bloody diarrhoea without fever in a child → STEC/HUS risk — check creatinine, platelet count, blood film for microangiopathy
- Severe UC with dilatation → toxic megacolon (colon diameter >6 cm on plain X-ray) — surgical emergency
- Dehydration with altered sensorium → hypovolaemic shock — treat first, diagnose second
The prioritised differential should be documented as a structured list in the clinical notes, with the most likely diagnosis first, followed by the alternative diagnoses in decreasing probability, and the must-not-miss items explicitly flagged even if lower priority. This documentation demonstrates the reasoning, not just the outcome.
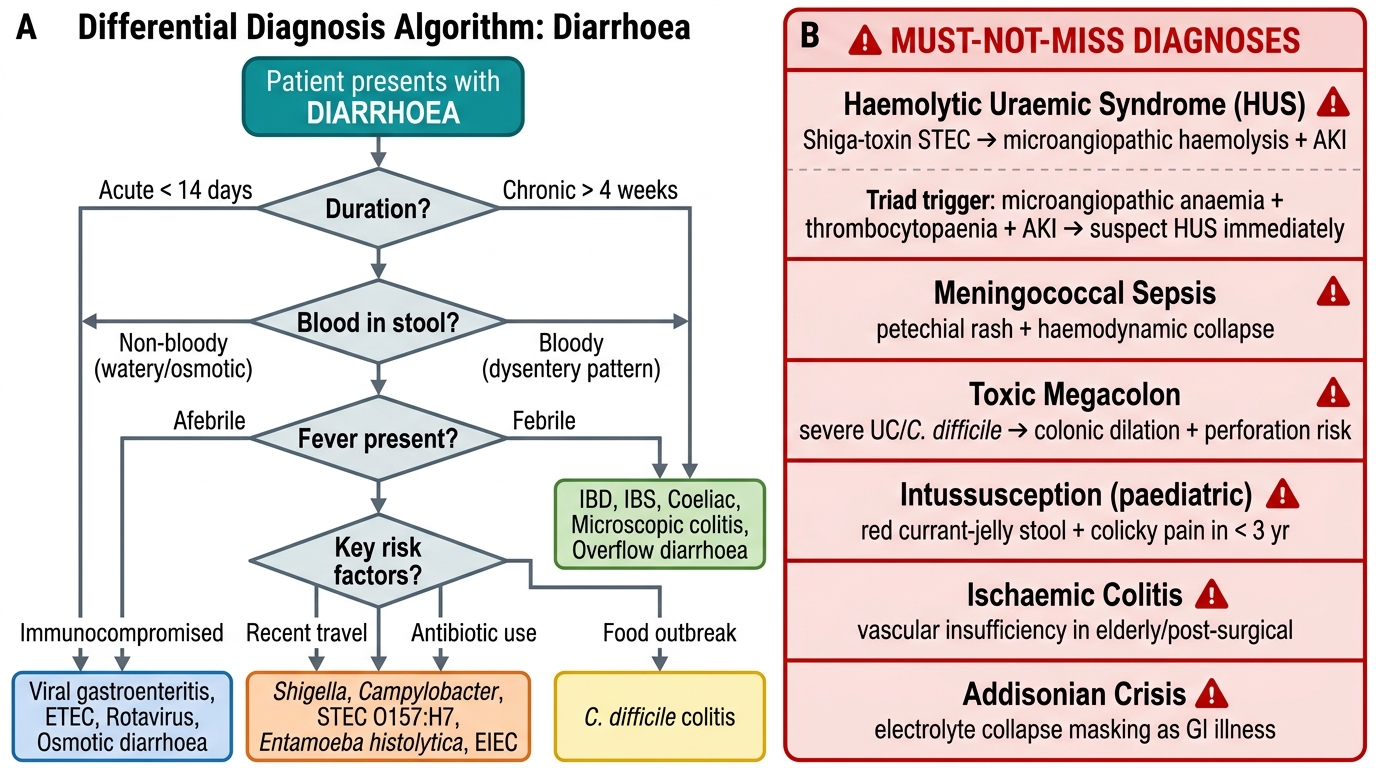
Decision Algorithm for Differential Diagnosis in Diarrhoea with Must-Not-Miss Red Flags
SELF-CHECK
A 9-year-old girl presents with three days of watery, non-bloody diarrhoea, abdominal cramps, and low-grade fever. She then develops oliguria, pallor, and petechiae. Her blood results show: Hb 7.2 g/dL, platelets 45×10⁹/L, creatinine 280 μmol/L, blood film shows fragmented red blood cells. What is the MOST LIKELY diagnosis, and what is the key causative mechanism?
A. Cholera; severe isotonic dehydration causing pre-renal AKI
B. Haemolytic Uraemic Syndrome (HUS); Shiga-toxin from STEC producing microangiopathic haemolysis
C. Severe UC with toxic megacolon; perforation causing bacteraemia
D. Amoebic dysentery with hepatic abscess; haemolytic anaemia from amoebic toxins
Reveal Answer
Answer: B. Haemolytic Uraemic Syndrome (HUS); Shiga-toxin from STEC producing microangiopathic haemolysis
The triad of microangiopathic haemolytic anaemia (fragmented RBCs on blood film), thrombocytopaenia, and acute kidney injury following a diarrhoeal illness is the classic presentation of Haemolytic Uraemic Syndrome (HUS). In children, the most common cause is Shiga-toxin-producing E. coli (STEC), particularly serotype O157:H7 — the diarrhoea is initially watery and non-bloody, then becomes bloody as colitis develops, followed by the systemic microangiopathy. Cholera causes pre-renal AKI from volume depletion but does not produce microangiopathic haemolysis or thrombocytopaenia. HUS is a must-not-miss diagnosis requiring early recognition and avoidance of antibiotics and antimotility agents (which increase Shiga toxin release).
Applied Practice: Documenting and Presenting the Clinical Evaluation
The clinical skill (IM16.4, IM16.5) requires not only that you take a thorough history and perform a systematic physical examination, but that you document and present your findings in a way that communicates the diagnostic reasoning — not just a list of positive and negative findings. Medical documentation in diarrhoeal disorders must be structured to support triage, treatment initiation, and differential diagnosis — because the written record may be the basis for another clinician's decision if you are not available. In an OSCE, the presentation of your findings to an examiner follows the same principles of structured communication.
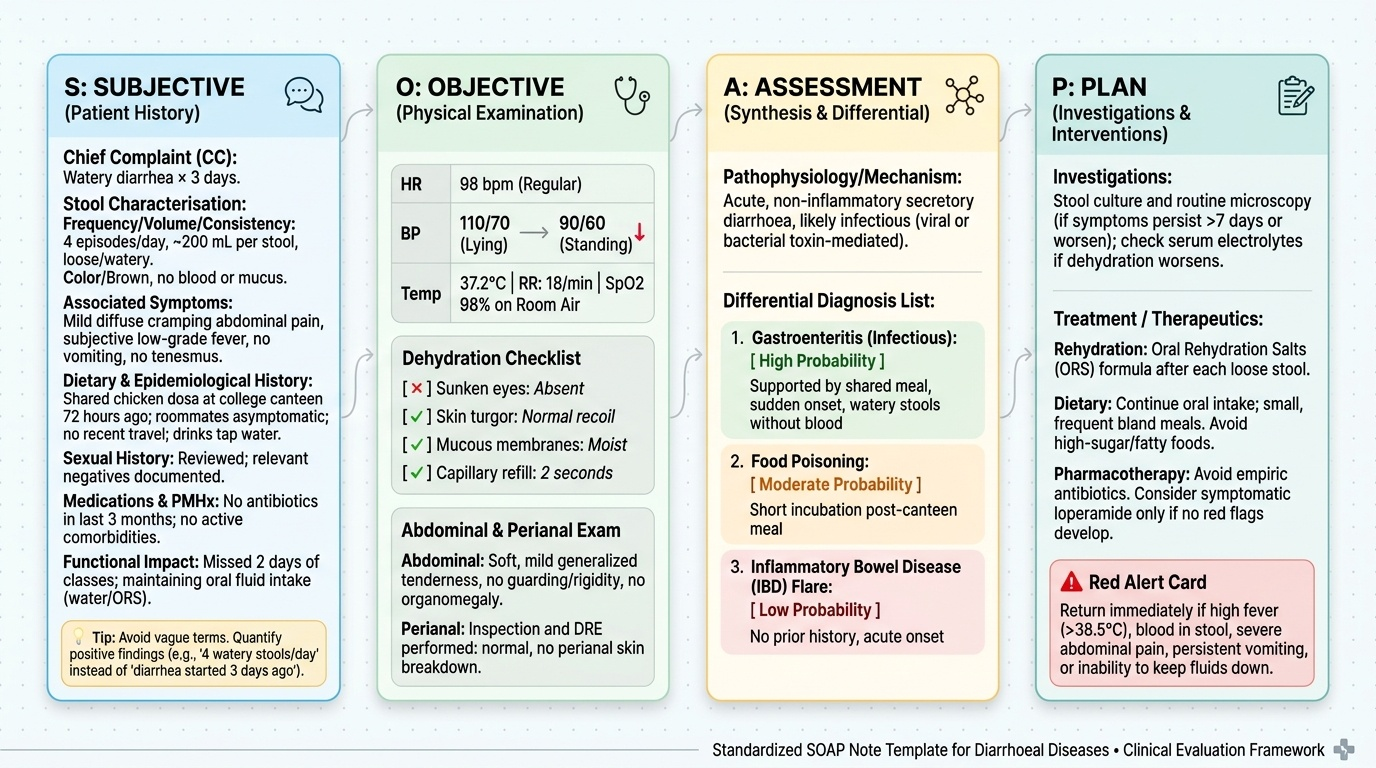
Provided image
Documenting the history: Write in a problem-oriented format. Begin with the chief complaint and its duration. Then systematically document: stool characterisation (frequency, volume, consistency, blood/mucus, colour), associated symptoms (fever temperature if measured, pain character and site, vomiting, tenesmus), dietary history (last 72 hours, any shared meals, specific foods), epidemiological context (travel, contacts with similar illness, source of drinking water), sexual history (document that it was taken and relevant negatives or positives), medication history (antibiotics within last 3 months, current medications including OTC), and past medical history with co-morbidities. Functional impact: how many days unable to work/study, fluid intake maintained or not. Each positive finding should be quantified where possible ("4 watery stools per day, approximately 200 mL per stool, onset 3 days ago after sharing dosa at college canteen") rather than vague ("diarrhoea started 3 days ago").
Documenting the physical examination: Record vital signs as numbers with units — "HR 98/min, BP 110/70 mmHg (lying) → 90/60 mmHg (standing; orthostatic drop 20/10 mmHg), Temp 37.2°C, RR 18/min, SpO2 98%." Dehydration signs: document each sign and whether present or absent (sunken eyes: absent; skin turgor: normal recoil; mucous membranes: moist; capillary refill: <2 sec). Abdominal examination: describe inspection findings explicitly (not "abdomen soft" alone), tenderness site and character, organ enlargement with dimensions, presence or absence of guarding. Perianal findings: describe explicitly or state "perianal inspection and DRE performed — normal."
Presenting in the OSCE or ward round: Use the structured presentation: (1) Patient demographics, (2) Chief complaint and duration, (3) History of presenting illness — mechanism-focused narrative ("This is a presentation most consistent with secretory diarrhoea given large volume, watery stools without blood, absence of fever, and onset 6 hours after a shared meal"), (4) Relevant positive and negative history, (5) Physical examination summary — severity first ("No features of dehydration; haemodynamically stable"), then localising signs, then systemic findings, (6) Working diagnosis and differential: lead with most likely, flag must-not-miss, (7) Proposed investigations and management plan.
Self-Assessment: Clinical Evaluation Scenarios
Apply the history, examination, and differential generation skills from this module to the following scenarios. For each, identify which questions in the history were the pivotal diagnostic drivers and what physical examination findings you would specifically seek.
Scenario A: A 67-year-old retired teacher presents with 10 weeks of loose stools, two to three per day, no blood, mild lower abdominal discomfort relieved by defaecation, and no weight loss. He has no fever and his physical examination is entirely normal. He takes no medications and has not travelled. His younger sister was diagnosed with irritable bowel syndrome. What is the highest-priority diagnosis to exclude before attributing this to IBS, and what key history question separates IBS from colorectal cancer?
Analysis: Chronic diarrhoea in a 67-year-old without blood but with lower abdominal discomfort — IBS vs colorectal cancer. The must-not-miss here is colorectal carcinoma — age >60, altered bowel habit. The key history question: is there any rectal bleeding, even minimal/intermittent ("sometimes a trace of blood or dark stool")? Weight loss? Nocturnal symptoms? (IBS does not wake the patient from sleep; organic disease often does.) Anaemia symptoms? Family history of colorectal cancer? IBS criteria (Rome IV) require: recurrent abdominal pain ≥1 day/week for ≥3 months, associated with defaecation, change in frequency, or change in stool form — but IBS is a diagnosis of exclusion in a 67-year-old, requiring colonoscopy to rule out malignancy.
Scenario B: A 35-year-old HIV-positive woman (CD4 count 85 cells/μL, not on ART due to adherence issues) presents with 4 weeks of watery, non-bloody diarrhoea, 8 stools per day, and weight loss of 5 kg. She has no fever. Routine stool microscopy shows no parasites. Stool culture: no growth at 48 hours. What three pathogens should be specifically investigated that the routine stool examination misses, and why?
Analysis: Severe immunosuppression (CD4 <200) + chronic watery diarrhoea not detected on routine examination = opportunistic organisms. Specifically: (1) Cryptosporidium parvum — requires modified Ziehl-Neelsen (acid-fast) staining of stool, not seen on standard wet preparation; (2) Microsporidia — requires modified trichrome stain or electron microscopy; (3) Cytomegalovirus (CMV) colitis — requires colonoscopy with biopsy showing CMV inclusion bodies ("owl eye" cells). Standard bacterial culture at 48 hours misses all three. The treatment for Cryptosporidium in this case is ART initiation to restore CD4 count — nitazoxanide has limited efficacy in severe immunosuppression.
Scenario C: A 22-year-old woman has had intermittent right lower quadrant pain for 9 months, two to four loose stools per day (occasionally with blood), and 6 kg weight loss. She also mentions two perianal fistulae discovered 1 year ago (attributed to "haemorrhoids" at the time). On examination, she is thin, has right iliac fossa tenderness, and you find two indurated nodules on her anterior shins. What diagnosis do these findings collectively support, what are the perianal fistulae and shin lesions respectively, and what must be excluded before starting immunosuppressive therapy in India?
Analysis: Terminal ileitis pattern (right iliac fossa) + perianal fistulae (now recognised as Crohn's-associated) + erythema nodosum (painful indurated nodules on anterior shins = classic extra-intestinal manifestation of IBD, most common with Crohn's) + weight loss + young woman = Crohn's disease. Before starting immunosuppression (azathioprine, anti-TNF), always exclude intestinal tuberculosis — the clinical, endoscopic, and radiological overlap is high in India (ileocaecal involvement, granulomas on biopsy, strictures). Perform: Mantoux test, IGRA (QuantiFERON), chest X-ray, colonoscopy with deep biopsies (caseating vs non-caseating granulomas on histology). If equivocal, consider an empirical 2-month anti-TB trial before committing to immunosuppression.
SELF-CHECK
A 72-year-old man presents with a 5-month history of alternating constipation and diarrhoea, bright red rectal bleeding on three occasions (each attributed to 'haemorrhoids' by the patient), 7 kg weight loss, and progressively worsening lower abdominal discomfort. His father died of colorectal cancer. On examination, there is left iliac fossa tenderness and digital rectal examination reveals a hard, irregular mass felt at 8 cm from the anal margin. What is the single MOST IMPORTANT next investigation?
A. Stool culture for bacterial pathogens
B. Colonoscopy with biopsy
C. Serum CEA level
D. Abdominal X-ray for obstruction
Reveal Answer
Answer: B. Colonoscopy with biopsy
This presentation is colorectal carcinoma until proven otherwise: age >70, change in bowel habit, rectal bleeding, significant weight loss, family history of CRC, and — most importantly — a palpable rectal mass on DRE. The single most important next investigation is colonoscopy with biopsy, which provides both diagnosis (histological confirmation of malignancy) and extent (synchronous lesions). Serum CEA (carcinoembryonic antigen) is a useful tumour marker for monitoring but is neither sensitive nor specific enough for diagnosis. Stool culture is irrelevant for an apparent malignancy. Abdominal X-ray for obstruction is relevant if obstruction is suspected, but the diagnostic priority is histological confirmation first. This case also illustrates the must-not-miss principle: attributing rectal bleeding to haemorrhoids without investigation in a patient >50 with change in bowel habit is a diagnostic error.
CLINICAL PEARL
The single most common diagnostic error in diarrhoeal disorders at the bedside is attributing chronic rectal bleeding in a patient over 50 to haemorrhoids without performing a proper examination and investigation. Haemorrhoids bleed — but so does colorectal cancer. The history alone cannot reliably distinguish the two, and digital rectal examination and proctoscopy (or colonoscopy in older patients) must be performed before diarrhoea with rectal bleeding is dismissed as haemorrhoidal. In India, where consultation for rectal symptoms may be delayed by embarrassment and where colonoscopy access is limited in some settings, this diagnostic delay contributes measurably to late-stage colorectal cancer presentation.
A second pearl for the history: ask specifically about nocturnal diarrhoea. IBS does not wake patients from sleep — if a patient reports waking at 3 AM to pass stool, the diagnosis is organic disease (IBD, microscopic colitis, secretory tumour, diabetic autonomic neuropathy) until proven otherwise. This single question separates a common benign functional disorder from conditions requiring investigation.