Page 10 of 21
IM17.6-9 | Headache Diagnostic Testing and Lumbar Puncture — SDL Guide (Part 2)
Lumbar Puncture Technique: Step-by-Step Procedure
The following procedure describes LP on an adult patient in the clinical setting. Each step is linked to its rationale, and the common errors at each step are identified. Mastery of this sequence is required for the IM17.8 OSCE demonstration on a mannequin.
Step 1 — Preparation and consent: Obtain verbal or written informed consent. Explain the procedure (needle in the back to sample fluid around the spinal cord), its purpose, and the risks (post-LP headache most common; rare: haematoma, infection, failure). Confirm no contraindications. Ensure IV access, analgesia available if needed, and resuscitation equipment accessible.
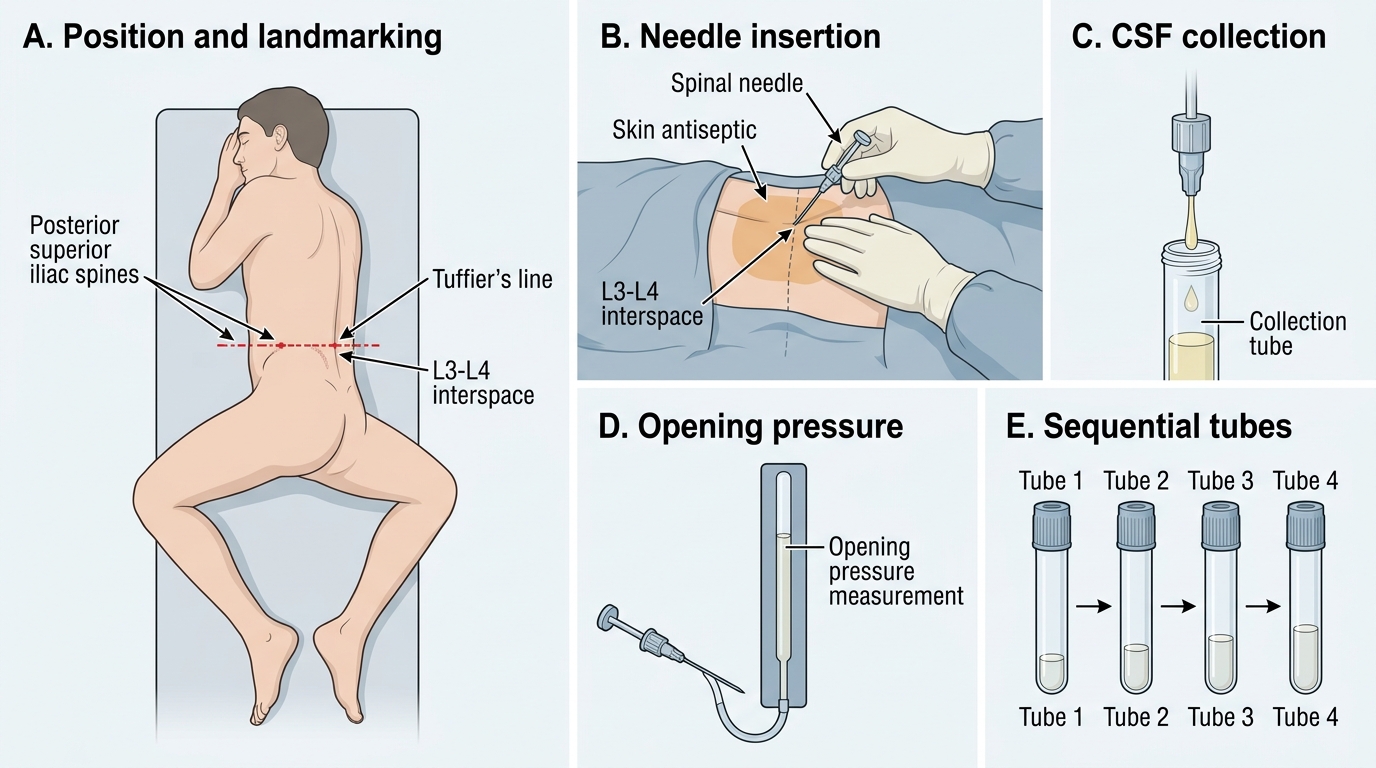
Step 2 — Positioning: Place the patient in the lateral decubitus (foetal) position at the edge of the bed — hips and knees maximally flexed toward the chest, spine parallel to the bed, neck flexed. An assistant supports the position from the front. The back should be at 90° to the bed surface (not rotated). For obese patients or when midline is difficult to palpate, the sitting position (leaning forward over a pillow) aids landmark identification but does not allow accurate pressure measurement.
Step 3 — Landmark identification: Locate Tuffier's line (posterior iliac crest–to–crest). Identify the L4 spinous process at this level. Mark the L3–L4 interspace (one level above) or L4–L5 interspace (at Tuffier's line). Palpate the interspinous space with the thumb — the midline depression between adjacent spinous processes is the target.
Step 4 — Asepsis: Surgical hand wash and sterile gloves. Full sterile draping of the lumbar region. Clean the skin with antiseptic (chlorhexidine preferred to povidone-iodine — lower infection risk, faster action) using concentric circular wipes outward from the intended puncture site. Allow the antiseptic to dry before needle insertion (avoids introducing antiseptic into CSF).
Step 5 — Local anaesthesia: Raise a subcutaneous bleb of 1% lidocaine (without adrenaline) at the puncture site with a 25G needle. Infiltrate deeper tissues along the intended needle tract. Allow 2–3 minutes for full effect. The local anaesthetic bleb serves both to anaesthetise the skin and to confirm the midline (midline injection is easier to introduce perpendicularly).
Step 6 — Needle insertion: Use a 22G (or 25G) Quincke-tip spinal needle, introduced in the midline with the bevel oriented parallel to the longitudinal dural fibres (bevel facing cephalad in lateral decubitus — this means the bevel faces upward when the patient is on their side). Direct the needle slightly cephalad (angled toward the umbilicus at approximately 15° from vertical to accommodate the caudal tilt of the spinous processes). Advance slowly and steadily, feeling for the following tissue layers: skin → subcutaneous fat → supraspinous ligament (fibrous resistance) → interspinous ligament (increased resistance) → ligamentum flavum (markedly increased resistance — the thickest barrier) → brief release as the epidural space is entered → dura (subtle 'pop' or change in resistance) → subarachnoid space.
Step 7 — CSF flow confirmation: Remove the stylet and observe for CSF dripping from the needle hub. CSF is clear, water-like, and drips at approximately 1 drop per second at normal pressure. If no CSF flows: (a) rotate the needle 90° (bevel may be occluded by a nerve root); (b) reintroduce the stylet and advance 1–2 mm; (c) if still no CSF after 3 attempts in the same interspace, attempt the next interspace (L4–L5 or L2–L3).
Step 8 — Pressure measurement: Connect the manometer before collecting CSF. Ensure the patient's legs are partially extended (fully flexed legs elevate intra-abdominal pressure and falsely raise the reading). Read the opening pressure when the CSF column stabilises (normal: 10–20 cmH₂O). Observe for respiratory oscillation (confirms correct placement in subarachnoid space).
Step 9 — CSF collection: Collect sequentially into 4 numbered sterile specimen tubes (1–2 mL each, or as required for ordered tests). Standard allocation: tube 1 = cell count + differential; tube 2 = protein + glucose (with simultaneous serum glucose); tube 3 = microbiology (Gram stain, culture and sensitivity, AFB smear, India ink, fungal culture); tube 4 = additional tests (cryptococcal antigen, cytology for malignant cells, viral PCR, oligoclonal bands, GeneXpert MTB/RIF). Tube 4 is also used to assess clearing (traumatic tap: significantly fewer RBCs in tube 4 versus tube 1; SAH: uniform counts and xanthochromic supernatant in all tubes).
Step 10 — Needle removal: Reinsert the stylet fully before withdrawing the needle (reduces CSF leak through the needle track and decreases post-LP headache risk). Apply firm pressure to the puncture site. The patient lies flat for 1–2 hours post-procedure; ensure adequate hydration.
Post-LP headache: Occurs in 10–30% of LPs. Orthostatic character — worse on sitting/standing, relieved by lying flat — due to ongoing CSF leak. Treatment: bed rest, oral fluids (2–3 L/day), oral caffeine 300 mg. Refractory (>72 hours): epidural blood patch (10–20 mL autologous blood injected into the epidural space at the LP site by an anaesthetist — seals the dural defect; >90% effective).
Lumbar Puncture Procedure: Step-by-Step Sequence
CSF Analysis: Normal Values and Interpretation Framework
Interpreting a CSF analysis report requires applying the reported values against normal reference ranges and recognising the characteristic patterns produced by specific pathological processes. CSF analysis encompasses several parameters — appearance, opening pressure, cell count and differential, protein, glucose, and microbiological stains — each contributing a distinct piece of the diagnostic picture. The skill lies in reading all parameters together rather than in isolation, because no single abnormality is pathognomonic in isolation; it is the complete pattern that is diagnostic. The combination of cell count, differential, protein, glucose, appearance, and microbiological stains forms a diagnostic signature that distinguishes bacterial meningitis from viral meningitis from tuberculous meningitis from SAH with considerable confidence when all values are interpreted simultaneously. This integrated pattern-recognition skill is exactly what IM17.9 tests at the SH level — and it requires memorising both the normal reference values AND the four abnormal archetypes.
The normal CSF reference values that must be memorised:
- Appearance: crystal clear (water-clear), colourless
- Opening pressure: 10–20 cmH₂O (lateral decubitus)
- White cell count (WBC): 0–5 cells/mm³, all lymphocytes; NO neutrophils in normal CSF
- Red cell count (RBC): 0 cells/mm³ (any RBC is abnormal unless attributable to traumatic tap)
- Protein: 15–45 mg/dL
- Glucose: 50–80 mg/dL; CSF:serum glucose ratio >0.6 (paired serum glucose drawn at LP time)
- Gram stain, India ink, AFB smear, culture: all negative/sterile
The CSF:serum glucose ratio is a critical derived value because it corrects for the patient's blood glucose. A CSF glucose of 40 mg/dL may be normal in a hypoglycaemic patient (serum 60 mg/dL, ratio 0.67) but profoundly abnormal in a normoglycaemic patient (serum 100 mg/dL, ratio 0.40). This is why a paired serum glucose must always be drawn at the time of LP.
The four key CSF interpretation archetypes:
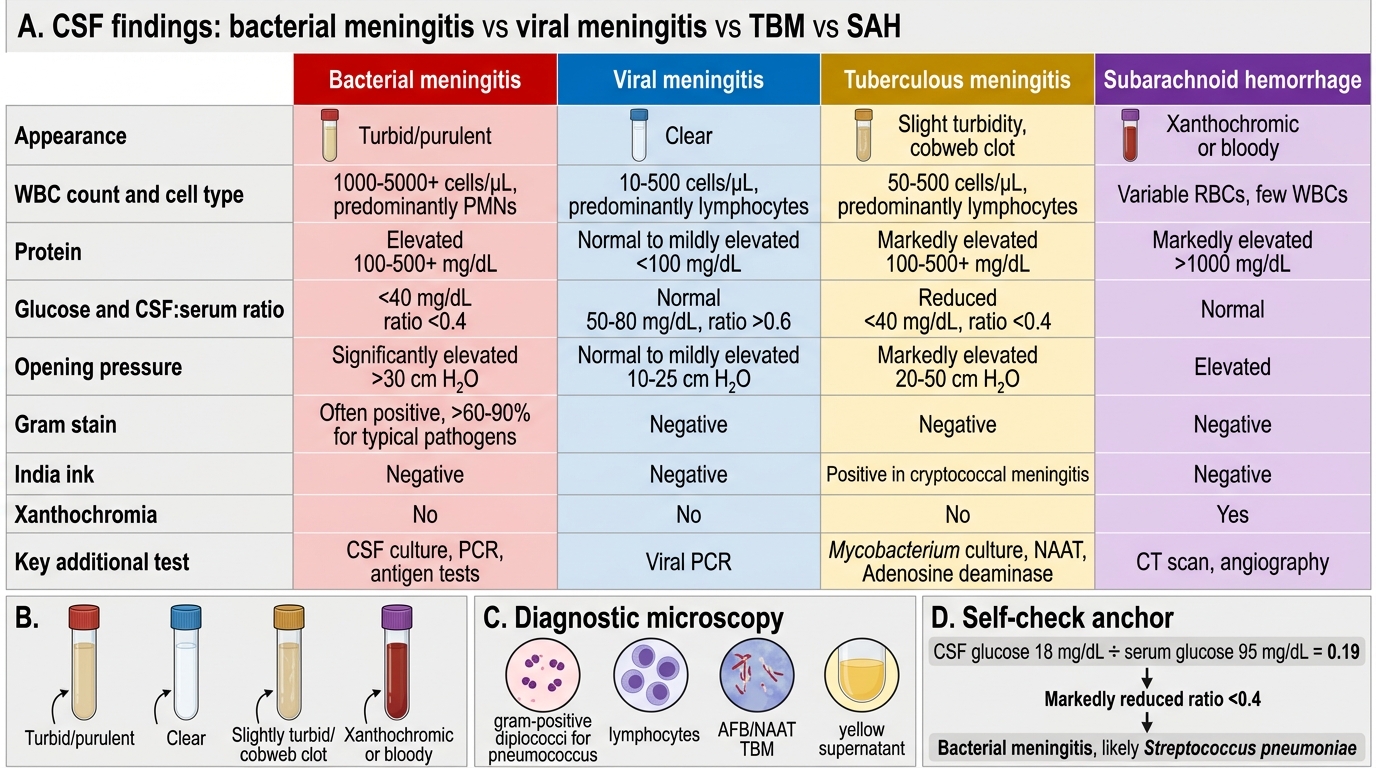
Bacterial meningitis: Appearance turbid/purulent/cloudy. WBC markedly elevated: typically 500–10,000+ cells/mm³, predominantly neutrophils (>80%). Protein markedly elevated: >100 mg/dL (often 200–500 mg/dL). Glucose markedly low: CSF:serum ratio <0.4, absolute glucose often <40 mg/dL. Opening pressure elevated. Gram stain positive in 60–80% (before antibiotics).
Viral meningitis (aseptic meningitis): Appearance clear or slightly turbid. WBC moderately elevated: 10–500 cells/mm³, predominantly lymphocytes (note: early viral meningitis may transiently show neutrophils in the first 24–48 hours, then shifts to lymphocytes). Protein mildly elevated: 50–200 mg/dL. Glucose normal: CSF:serum ratio ≥0.6. Gram stain and culture: negative. The normal CSF glucose is the key distinguishing feature from bacterial meningitis.
Tuberculous meningitis (TBM): Appearance clear or opalescent; may form a fibrin 'cobweb clot' on standing. WBC moderately elevated: 50–500 cells/mm³, predominantly lymphocytes. Protein moderately to markedly elevated: 100–500 mg/dL (often the highest protein of all meningitides). Glucose low: CSF:serum ratio <0.5, sometimes very low (<20 mg/dL in advanced disease). AFB smear: positive in only 10–40% — low sensitivity, multiple samples required. GeneXpert MTB/RIF on CSF: sensitivity ~50–80%, results in 2 hours. Opening pressure: elevated.
Subarachnoid haemorrhage (SAH): Appearance uniformly blood-stained in all 4 tubes (distinguishes from traumatic tap where blood clears from tube 1 to tube 4). After centrifugation, supernatant shows xanthochromia (yellow-orange) — detectable by spectrophotometry from ≥12 hours post-bleed, persisting up to 2 weeks. RBC count very high, uniform across all tubes. WBC mildly elevated (reactive). Protein elevated proportionally to blood. Glucose: normal (no infection).
CSF Findings in Meningitis and SAH
SELF-CHECK
A CSF report shows: appearance turbid; WBC 1,200 cells/mm³ with 90% neutrophils; protein 320 mg/dL; glucose 18 mg/dL (simultaneous serum glucose 95 mg/dL); Gram stain: gram-positive diplococci. What is the diagnosis and CSF:serum glucose ratio?
A. Viral meningitis; CSF:serum ratio 0.19 — normal range
B. Bacterial meningitis (likely pneumococcal); CSF:serum ratio 0.19 — markedly reduced
C. Tuberculous meningitis; CSF:serum ratio 0.19 — typical of TBM lymphocytic pattern
D. Normal LP with traumatic tap artefact — CSF:serum ratio not interpretable
Reveal Answer
Answer: B. Bacterial meningitis (likely pneumococcal); CSF:serum ratio 0.19 — markedly reduced
CSF glucose 18 mg/dL ÷ serum glucose 95 mg/dL = CSF:serum ratio 0.19 (markedly reduced; normal ≥0.6; bacterial meningitis threshold <0.4). The turbid appearance, markedly elevated neutrophilic pleocytosis (1,200 cells, 90% neutrophils), very high protein (320 mg/dL), very low glucose ratio (0.19), and gram-positive diplococci on Gram stain together are diagnostic of bacterial meningitis — gram-positive diplococci = Streptococcus pneumoniae (pneumococcal meningitis). Viral meningitis has normal glucose and lymphocytic pleocytosis. TBM has lymphocytes and a subacute course. A traumatic tap produces uniform blood-staining but normal WBC, protein, and glucose.
CSF in TBM and Cryptococcal Meningitis: Special Patterns
Two specific meningitis patterns deserve expanded discussion because of their particular importance in the Indian clinical context and their distinctive CSF profiles that differ from the standard bacterial and viral archetypes. Both can be missed when the clinician expects the full-blown inflammatory picture of bacterial meningitis and overlooks the more subtle findings of TBM and cryptococcal meningitis.
Tuberculous meningitis (TBM) is the most feared CNS complication of tuberculosis and a leading cause of subacute meningitis in India. TBM results from the rupture of a cortical or subependymal TB focus (Rich focus) into the subarachnoid space, releasing mycobacteria and provoking a granulomatous inflammatory response predominantly involving the basilar meninges. Unlike bacterial meningitis which evolves over hours, TBM presents subacutely over days to weeks: headache, low-grade fever, meningism, and progressively altered consciousness. Cranial nerve palsies (CN II, III, IV, VI, VII) from basilar meningitis are characteristic; obstructive hydrocephalus and cerebral vasculitis causing infarcts are serious complications.
The CSF in TBM shows the lymphocytic meningitis with low glucose pattern. The characteristic 'cobweb clot' (a delicate fibrin pellicle that forms when TBM CSF is allowed to stand in a test tube) is a classic but increasingly rare observation. AFB smear has only 10–40% sensitivity — diagnosis relies on GeneXpert MTB/RIF (Xpert Ultra, sensitivity ~50–80% on CSF, result in ~2 hours) and mycobacterial culture (MGIT liquid medium or Löwenstein-Jensen solid medium, sensitivity 45–90%, takes 2–8 weeks). In clinical practice, TBM is frequently treated empirically with anti-TB therapy in patients with a compatible CSF profile and risk factors, even before microbiological confirmation — because untreated TBM has >50% mortality. The standard NTEP anti-TB regimen for TBM follows the same principle as pulmonary TB: 2HRZE + 10–12HR (intensive phase 2 months with isoniazid, rifampicin, pyrazinamide, ethambutol; continuation phase 10–12 months); adjunctive dexamethasone for 6–8 weeks to reduce meningeal inflammation and improve survival.
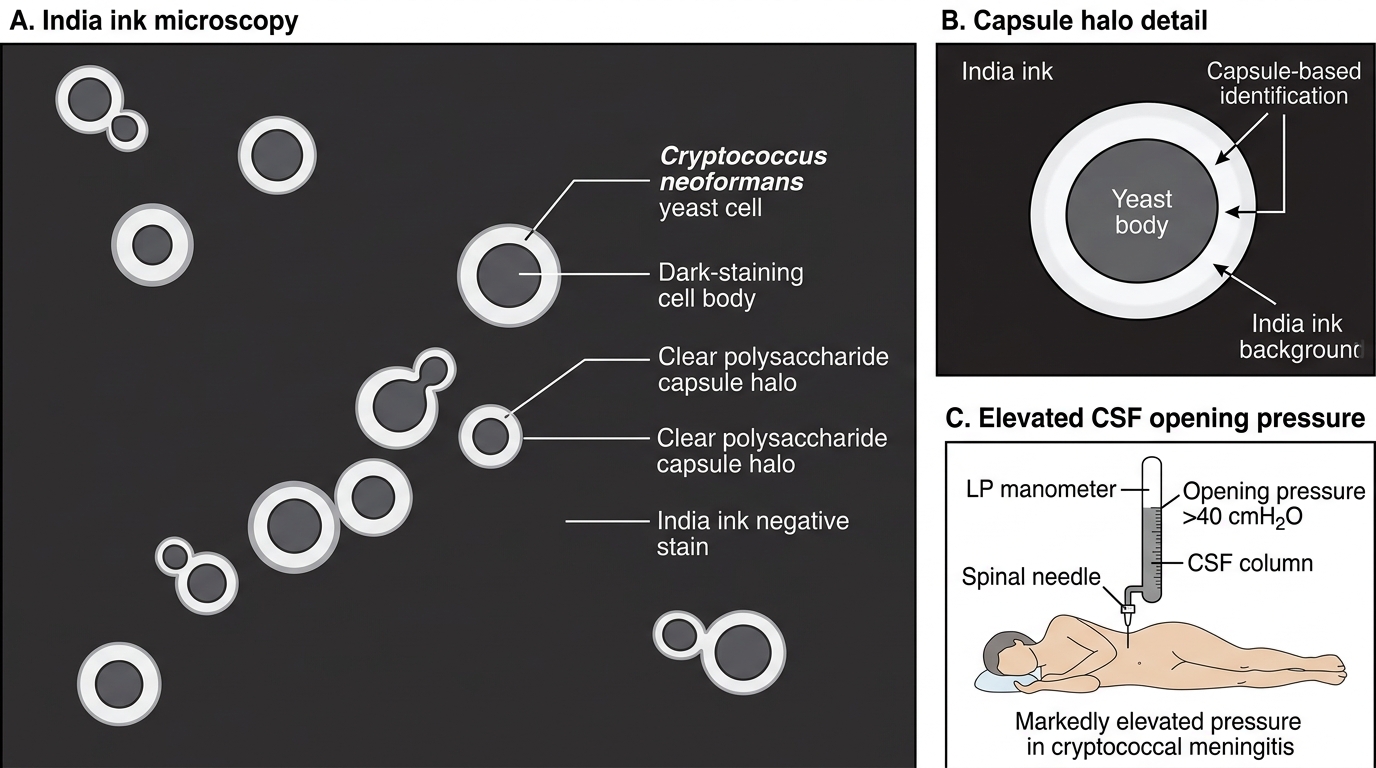
Cryptococcal meningitis is the most common cause of meningitis in HIV-positive patients with CD4 <100 cells/µL. The clinical presentation is insidious — headache that progresses over weeks with minimal fever, and classic meningeal signs may be absent because the immune response is blunted in severe immunosuppression. The CSF in cryptococcal meningitis typically shows: clear or slightly turbid appearance; minimal pleocytosis (often only 5–50 cells/mm³ despite florid infection — the blunted immune response produces few cells); mildly elevated protein; mildly low glucose. The opening pressure is typically markedly elevated (often >30–40 cmH₂O) due to impaired CSF resorption by cryptococcal capsular polysaccharide. India ink staining demonstrates encapsulated yeast cells with large clear capsule halos — sensitivity ~70–80% in AIDS-related disease. Cryptococcal antigen (CrAg) detection by lateral flow assay or latex agglutination on CSF or serum has sensitivity >95% — it is the test of choice for rapid diagnosis. Serial therapeutic LPs to reduce ICP below 20 cmH₂O are a critical component of management to prevent vision loss from optic neuropathy and herniation from raised ICP; this is as important as antifungal therapy in the first 2 weeks.
Cryptococcal Meningitis: India Ink Capsule Halo and Raised Opening Pressure
SELF-CHECK
A 35-year-old HIV-positive man (CD4 72 cells/µL) presents with 3 weeks of progressive headache. CSF: opening pressure 38 cmH₂O; appearance clear; WBC 8 cells/mm³ (all lymphocytes); protein 65 mg/dL; glucose 42 mg/dL (serum glucose 88 mg/dL, ratio 0.48). India ink shows encapsulated yeast. What is the diagnosis and the test with the highest sensitivity for confirmation?
A. Viral meningitis; PCR for HSV or enterovirus is most sensitive
B. Tuberculous meningitis; GeneXpert MTB/RIF on CSF is most sensitive rapid test
C. Cryptococcal meningitis; cryptococcal antigen (CrAg) in CSF or serum has sensitivity >95%
D. Bacterial meningitis; repeat CSF Gram stain and culture is most sensitive
Reveal Answer
Answer: C. Cryptococcal meningitis; cryptococcal antigen (CrAg) in CSF or serum has sensitivity >95%
The clinical context (HIV, CD4 72), insidious 3-week course, markedly elevated opening pressure (38 cmH₂O), minimal CSF pleocytosis (8 cells — blunted immune response in severe immunosuppression), mildly low glucose ratio (0.48), and India ink showing encapsulated yeast all diagnose cryptococcal meningitis. Cryptococcal antigen (CrAg) by lateral flow assay or latex agglutination has sensitivity >95% in AIDS-related disease — far exceeding India ink (~70–80%) and culture. The markedly elevated opening pressure (38 cmH₂O) requires serial therapeutic LPs to reduce ICP to <20 cmH₂O. Treatment: liposomal amphotericin B + flucytosine (2-week induction) → fluconazole (consolidation + maintenance).