Page 11 of 21
IM17.6-9 | Headache Diagnostic Testing and Lumbar Puncture — SDL Guide (Part 3)
Traumatic Tap vs True SAH: Interpretation Rules
One of the most practically important CSF interpretation challenges is distinguishing a traumatic tap — blood introduced into the sample during needle insertion by puncturing an epidural or subdural vessel — from a true subarachnoid haemorrhage. This distinction has immediate life-or-death consequences: misclassifying SAH as a traumatic tap delays potentially life-saving neurosurgical intervention, while misclassifying a traumatic tap as SAH exposes the patient to unnecessary angiography and its associated risks. Every clinician who performs LP must master this interpretation.
Two parameters distinguish the two conditions with high reliability:
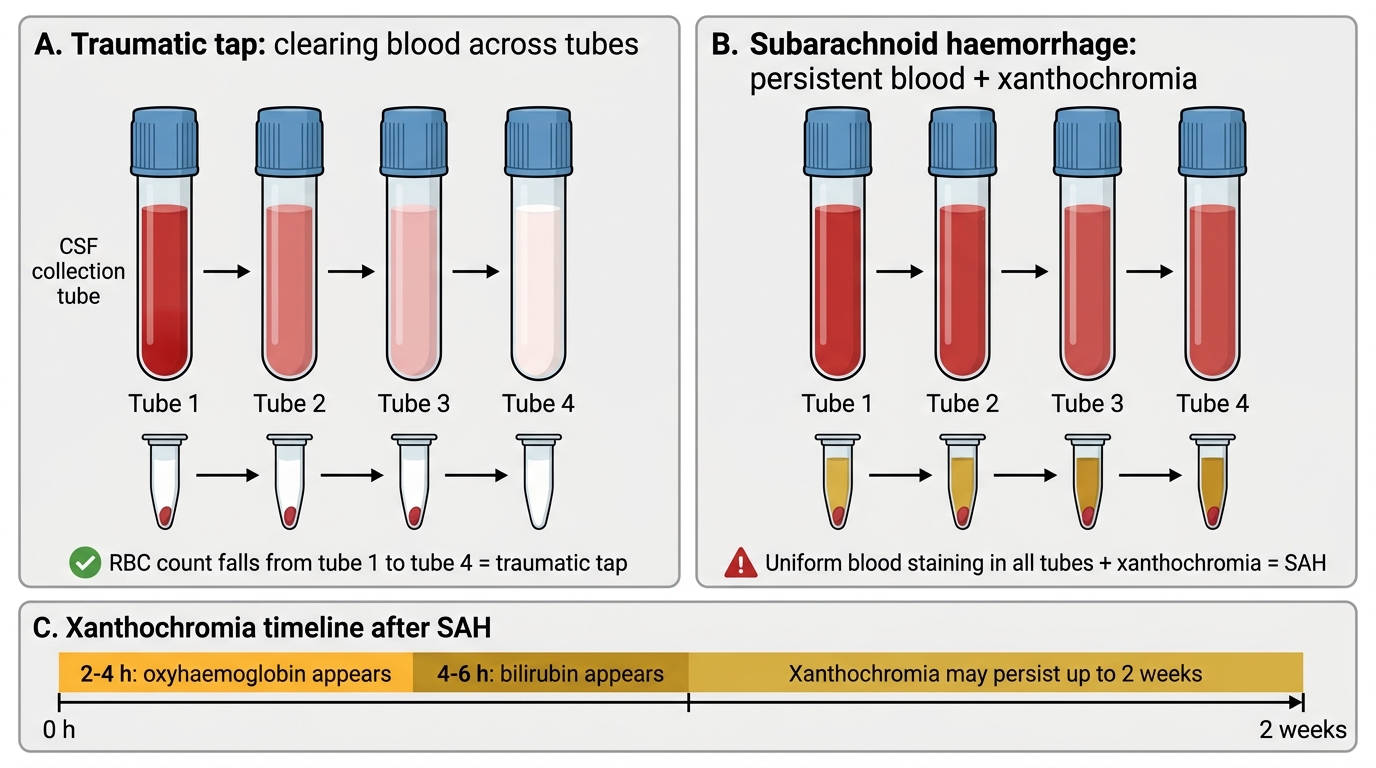
1. Blood clearance across collection tubes: In a traumatic tap, blood is introduced at the moment of needle entry and is not uniformly distributed throughout the CSF. It is therefore most concentrated in the first tube (collected first, closest to the bleeding point) and progressively decreases in subsequent tubes — tube 4 should show significantly fewer RBCs than tube 1. The conventional threshold is a ≥25% reduction in RBC count from tube 1 to tube 4 as evidence for traumatic tap. In true SAH, blood has been present in the CSF for hours before the LP and has distributed uniformly. Tube 4 therefore has the same RBC count as tube 1. Uniform RBC count across all 4 tubes = SAH until proven otherwise; progressive clearing = consistent with traumatic tap.
2. Xanthochromia of the spun supernatant: This is the definitive test. After centrifugation of the CSF sample, the supernatant is examined for yellow or orange-brown discolouration. Xanthochromia arises from the in-vivo degradation of haemoglobin: oxyhaemoglobin (pink-red, detectable from 2–4 hours post-bleed), and bilirubin (yellow, from 4–6 hours, persisting up to 2 weeks). In a traumatic tap, the blood has just entered the tube — there has been no time for in-vivo haemolysis; the spun supernatant is therefore crystal clear (though very high RBC counts in a traumatic tap can produce some in-vitro haemolysis, causing minimal pink discolouration that must be distinguished from xanthochromia on spectrophotometry). The NICE guidelines specify that spectrophotometry of the supernatant is significantly more sensitive than visual inspection and is the recommended method — it measures absorbance at specific wavelengths corresponding to oxyhaemoglobin (415 nm) and bilirubin (450–460 nm).
Timing is critical: LP must be performed ≥12 hours after headache onset to allow sufficient bilirubin to accumulate for detection. LP at <2–4 hours post-onset may give a false-negative result for xanthochromia even in genuine SAH, because bilirubin has not yet formed. The window for reliable xanthochromia detection is 12 hours to approximately 2 weeks post-bleed.
Practical summary: Uniform blood + xanthochromic spun supernatant + LP done ≥12 hours after onset = SAH confirmed. Progressive clearing of blood from tube 1 to tube 4 + clear spun supernatant = traumatic tap, SAH excluded (provided LP was done ≥12 hours after onset and spectrophotometry was used).
Traumatic Tap vs SAH: CSF Tube Pattern and Xanthochromia
Self-Assessment: CSF Interpretation Exercises
The IM17.9 competency requires you to interpret a CSF analysis report and match the pattern to the correct clinical diagnosis. The following self-assessment cases test this skill directly. For each case, read the data and generate: (1) the most likely diagnosis, (2) the key discriminating finding, and (3) one additional test to confirm.
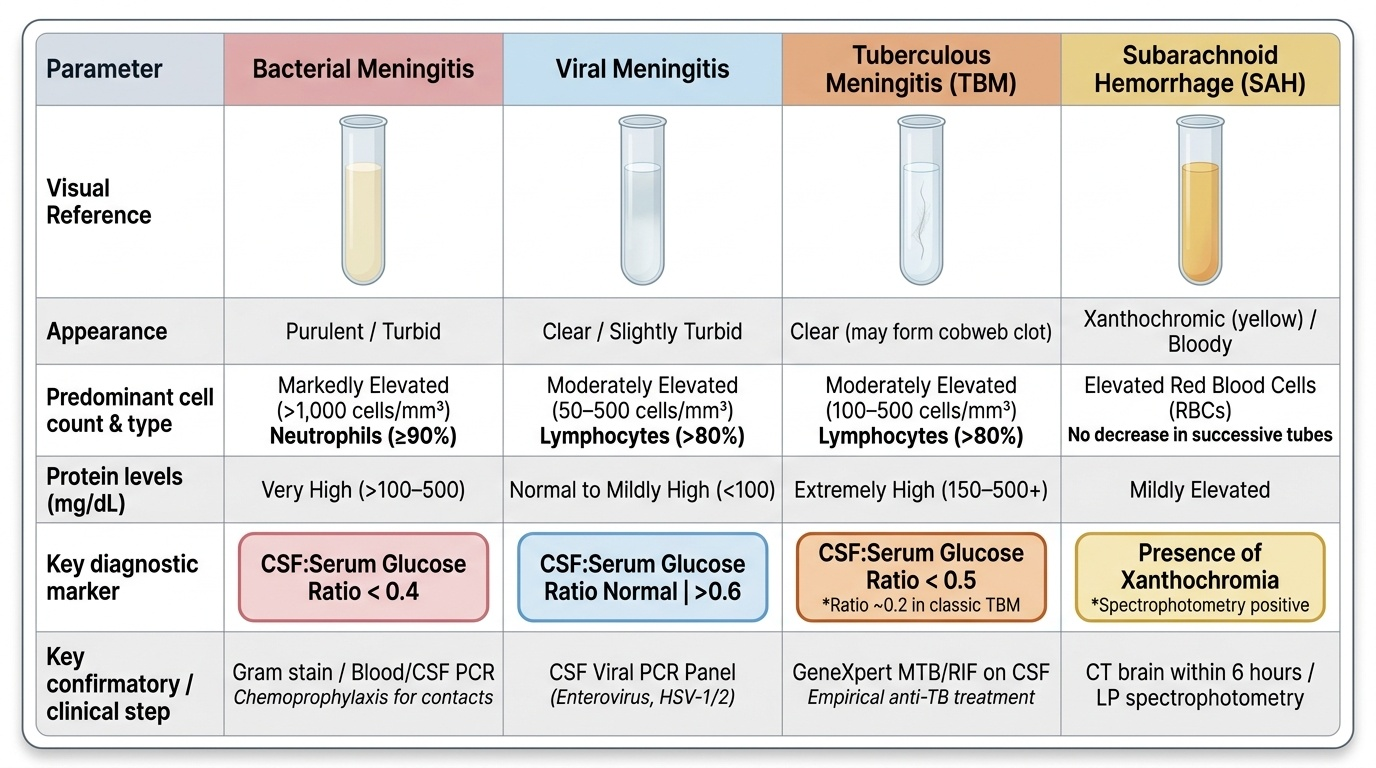
Provided image
Case 1: A 19-year-old has fever, headache, and neck stiffness over 6 hours. LP: appearance purulent; WBC 8,500 cells/mm³ (92% neutrophils); protein 480 mg/dL; glucose 12 mg/dL (serum 90 mg/dL); Gram stain: gram-negative diplococci.
Answer: Bacterial meningitis — meningococcal (Neisseria meningitidis). CSF:serum glucose ratio 0.13. Key discriminating finding: neutrophilic pleocytosis + very low glucose + gram-negative diplococci. Additional test: meningococcal PCR on blood or CSF (most sensitive, result within hours), notifiable disease — contact tracing and chemoprophylaxis (rifampicin or single-dose ciprofloxacin) for close contacts.
Case 2: A 28-year-old returns from Goa with headache and fever 4 days. LP: appearance slightly turbid; WBC 280 cells/mm³ (85% lymphocytes); protein 95 mg/dL; glucose 58 mg/dL (serum 82 mg/dL, ratio 0.71); Gram stain negative; India ink negative.
Answer: Viral (aseptic) meningitis. Key discriminating finding: lymphocytic pleocytosis with normal glucose ratio (0.71). Common causes in young adults: enterovirus, HSV-2, arboviral (dengue). Additional test: CSF viral PCR panel (enterovirus, HSV-1/2); dengue serology.
Case 3: A 42-year-old diabetic has headache, fever, and neck stiffness for 12 days with bilateral CN VI palsy. LP: clear CSF; WBC 320 cells/mm³ (88% lymphocytes); protein 340 mg/dL; glucose 22 mg/dL (serum 110 mg/dL, ratio 0.20); AFB smear negative; Gram stain negative; India ink negative.
Answer: Tuberculous meningitis (TBM). Subacute course + lymphocytic pleocytosis + very high protein + very low glucose + CN VI palsy from basilar meningitis = classic TBM. Key discriminating finding: the subacute course, lymphocytic pleocytosis, and very low glucose (ratio 0.20) with negative Gram stain and India ink. Additional test: GeneXpert MTB/RIF on CSF (rapid, ~50–80% sensitivity). Treat empirically with NTEP regimen: 2HRZE + 10HR + dexamethasone.
Case 4: A 24-year-old known migraineur with thunderclap headache. CT normal at 4 hours. LP at 14 hours: tube 1 RBC 18,000/mm³; tube 4 RBC 16,500/mm³ (no clearing). Spun supernatant: yellow-brown. Spectrophotometry: oxyhaemoglobin + bilirubin peaks confirmed.
Answer: Subarachnoid haemorrhage. Uniform RBC count (tubes 1 and 4 almost identical, no clearing) + xanthochromia on spectrophotometry = SAH confirmed. Prior migraine history is irrelevant. Additional test: CT angiography to identify the aneurysm before neurosurgical or endovascular treatment.
Applied Practice: Integrating Imaging, LP, and CSF Results
The complete diagnostic workflow for a headache patient requiring investigation integrates imaging, LP, and CSF analysis into a coherent sequence. At the applied practice level, you must not only interpret individual pieces of data correctly but also know how to sequence the investigations and act immediately on the results in real time. The three opening vignette cases are resolved here to demonstrate integrated clinical reasoning.
Case resolution — Arjun's thunderclap patient: The LP is mandatory at ≥12 hours post-onset despite the normal CT, for the reasons detailed in this module. The LP at ≥12 hours shows xanthochromia on spectrophotometry — SAH confirmed. The team proceeds immediately to CT angiography, which identifies a 7 mm posterior communicating artery aneurysm. Neurosurgical referral for endovascular coiling. Outcome: aneurysm secured before re-bleed. The attending who nearly accepted 'normal CT = no SAH' has now understood the lesson that cannot be learned twice safely.
Case resolution — The HIV patient (CD4 85): After CT excluded SOL, LP showed: opening pressure 38 cmH₂O, minimal pleocytosis, India ink positive, CrAg titre 1:512. Cryptococcal meningitis confirmed. Management: liposomal amphotericin B 3–4 mg/kg/day + flucytosine 100 mg/kg/day for 2 weeks (induction) → fluconazole 400 mg/day for 8 weeks (consolidation) → fluconazole 200 mg/day maintenance until CD4 >100 cells/µL on ART. Serial daily LPs reduced pressure from 38 to 18 cmH₂O over 5 days. ART initiated 4–6 weeks after antifungal therapy to reduce immune reconstitution inflammatory syndrome (IRIS) risk.
Case resolution — Fever + meningism + rash: Blood cultures drawn, IV ceftriaxone 2 g started within 10 minutes of patient arrival. LP performed 45 minutes after antibiotics — CSF: purulent, WBC 9,400 cells/mm³ (92% neutrophils), protein 420 mg/dL, glucose 8 mg/dL (ratio 0.09). Gram stain: gram-negative diplococci = meningococcal meningitis. Dexamethasone 0.15 mg/kg IV q6h for 4 days started with first antibiotic dose (reduces mortality and neurological sequelae in bacterial meningitis — most evidence in pneumococcal meningitis, also used in meningococcal). Public health notification for contact tracing; rifampicin chemoprophylaxis for household contacts.
The three cases illustrate the cardinal principle: diagnostic testing in headache is never a standalone exercise — each result triggers an immediate management action, and the sequence of investigations matters as much as the results themselves.
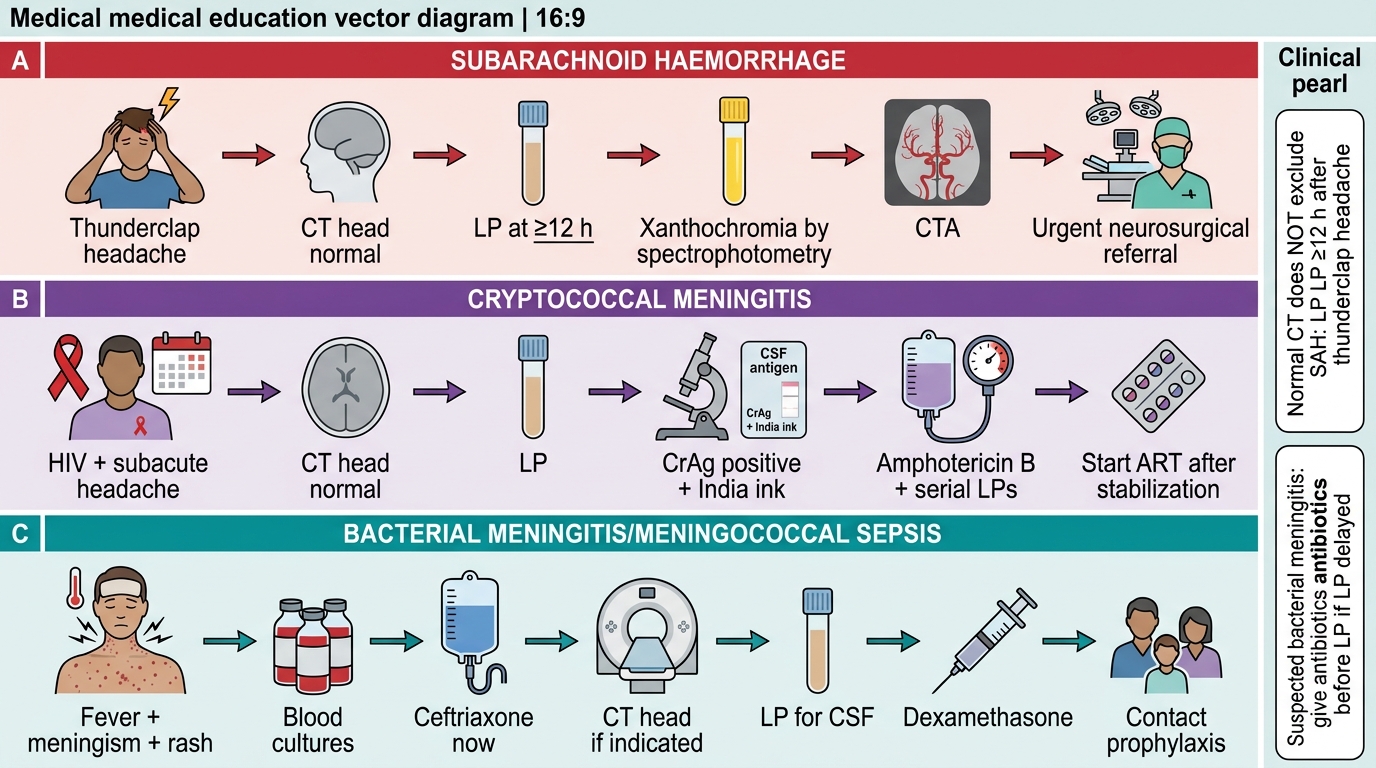
Three Critical Headache Pathways
CLINICAL PEARL
The most important clinical pearl in headache diagnostics: a normal CT head does NOT exclude subarachnoid haemorrhage. CT sensitivity for SAH peaks at ~98% within 6 hours; by 24 hours it falls to ~85%; by 1 week it is ~50%. Any thunderclap headache with a normal CT requires LP at ≥12 hours — with the supernatant examined by spectrophotometry, not visual inspection alone. The consequence of a missed SAH is re-bleed, which carries 40–50% mortality.
For LP: start antibiotics BEFORE LP if any delay in LP is anticipated in a patient with suspected bacterial meningitis — every hour without antibiotics worsens outcome. LP within 1 hour of starting antibiotics still gives diagnostic CSF information (cell count, protein, glucose remain abnormal; Gram stain sensitivity falls but is not zero). Never withhold antibiotics to preserve diagnostic CSF purity in a critically ill patient.