Page 2 of 21
IM17.{1,3} | Headache Foundations — SDL Guide (Part 2)
Migraine: ICHD-3 Diagnostic Criteria and Classification
Migraine is the most important primary headache disorder in clinical practice, both because of its high prevalence (affecting approximately 14–15% of the global population, with a female-to-male ratio of 3:1) and because its management requires precision in distinguishing classical from non-classical forms, abortive from preventive therapy, and episodic from chronic disease. Mastery of the ICHD-3 diagnostic criteria for migraine is therefore non-negotiable at the final-year level. The criteria are operationalised — meaning each element is defined with enough precision to be applied systematically to a clinical encounter, not left open to subjective interpretation. They also serve as the gold standard against which any new headache presentation must be tested before a treatment decision is made. Understanding both the individual criteria and the reasoning behind them will sharpen your diagnostic thinking and prevent two common errors: over-diagnosing migraine in patients whose headache lacks the full phenotype, and under-treating migraine in patients who present atypically.
Migraine without aura (formerly 'common migraine') is the most prevalent form and accounts for approximately 75–80% of all migraine cases. The ICHD-3 diagnostic criteria require:
1. At least 5 attacks fulfilling criteria B–D
2. Headache attacks lasting 4–72 hours (untreated or unsuccessfully treated)
3. Headache has at least 2 of the following 4 characteristics: (a) unilateral location, (b) pulsating quality, (c) moderate or severe pain intensity, (d) aggravation by or causing avoidance of routine physical activity
4. During headache, at least 1 of the following: (a) nausea and/or vomiting, (b) photophobia AND phonophobia
5. Not better accounted for by another ICHD-3 diagnosis
The mnemonic POUND is useful in clinical practice: Pulsating quality, duration One to three days (4–72 hours), Unilateral, Nausea/vomiting, Disabling. Each of the 5 POUND criteria present increases diagnostic certainty; ≥4/5 has a positive LR of approximately 24 for migraine diagnosis.
Migraine with aura (formerly 'classical migraine') accounts for approximately 20–25% of migraine cases. The additional ICHD-3 criterion requires at least 2 attacks with at least one of the following fully reversible aura symptoms: visual, sensory, speech/language, motor, brainstem, or retinal. The aura must develop gradually over ≥5 minutes, with each symptom lasting 5–60 minutes, followed by headache onset within 60 minutes (though sometimes aura occurs without headache). The visual aura is most common (seen in >90% of aura episodes), typically manifesting as a scintillating scotoma — a flickering arc of zigzag lines (fortification spectra) surrounding a blind spot, which expands and moves across the visual field over 20–30 minutes. Sensory aura (ipsilateral tingling that migrates from fingers to arm to face — the 'marching' distribution) and speech/language aura are less common.
Menstrual migraine deserves specific mention in the Indian context: attacks occurring exclusively or predominantly in the perimenstrual window (day −2 to +3 of menstruation) due to the fall in oestradiol. This subtype is typically without aura, often more severe, and may require specific hormonal or preventive management strategies.
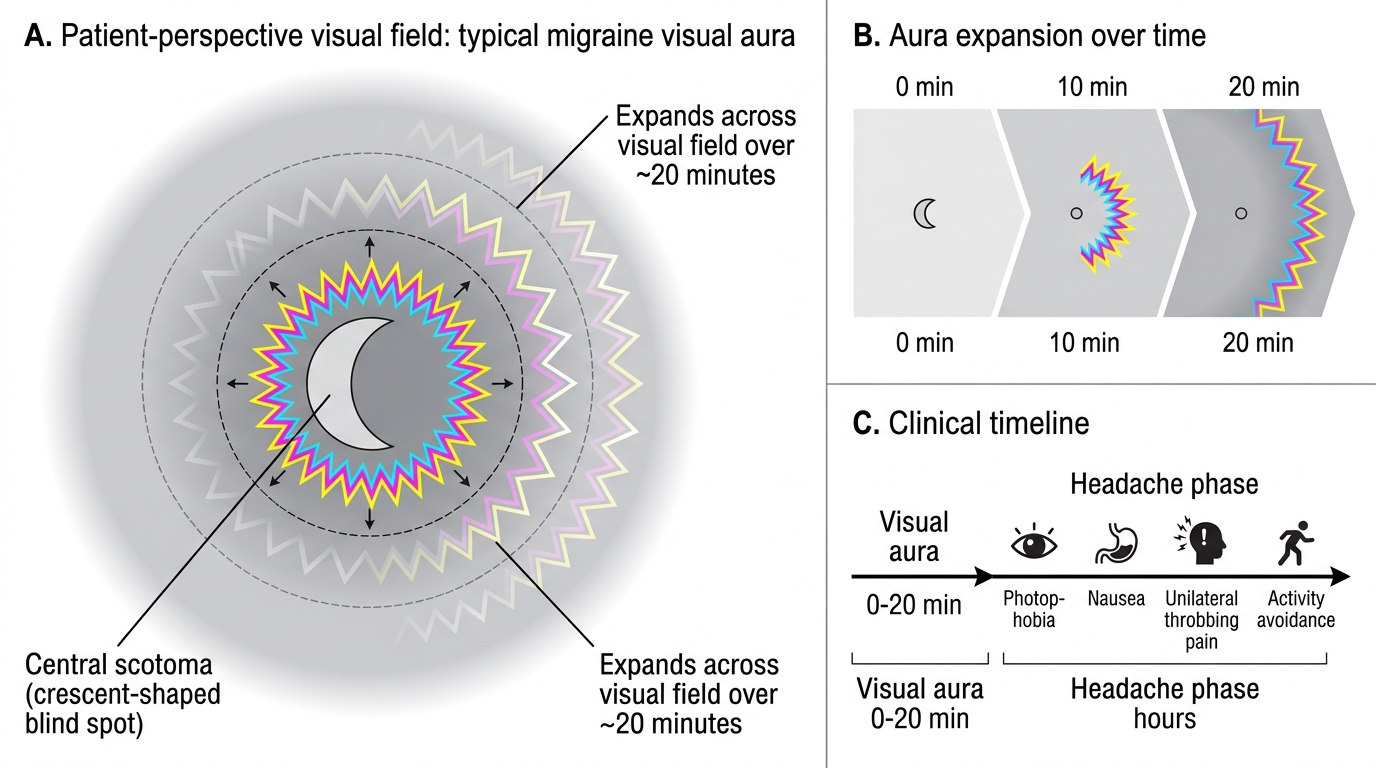
Typical Visual Aura of Migraine
SELF-CHECK
A 30-year-old woman presents with a 5-year history of recurrent headaches occurring 3–4 times per month. Each attack lasts 10–14 hours, is located on the right side, described as throbbing, moderate-to-severe in intensity, and accompanied by nausea and photophobia. She avoids her usual activities during attacks. She has no preceding neurological symptoms. How many of the ICHD-3 criteria for migraine without aura does she fulfil?
A. She fulfils only 2 of the required 4 headache characteristics
B. She fulfils criteria but requires brain imaging before diagnosis
C. She fulfils all required criteria for migraine without aura
D. Her attack duration is outside the ICHD-3 range and excludes migraine
Reveal Answer
Answer: C. She fulfils all required criteria for migraine without aura
She has ≥5 attacks (monthly recurrence ×5 years), duration 10–14 hours (within the 4–72-hour window), unilateral location + pulsating quality + severe intensity + avoidance of activity (3 of 4 headache characteristics — only 2 needed), nausea and photophobia (meets the associated features criterion), and no better explanation. All ICHD-3 criteria for migraine without aura are fulfilled. Brain imaging is NOT required to diagnose migraine — it is a clinical diagnosis. Her attack duration of 10–14 hours is well within the 4–72-hour range.
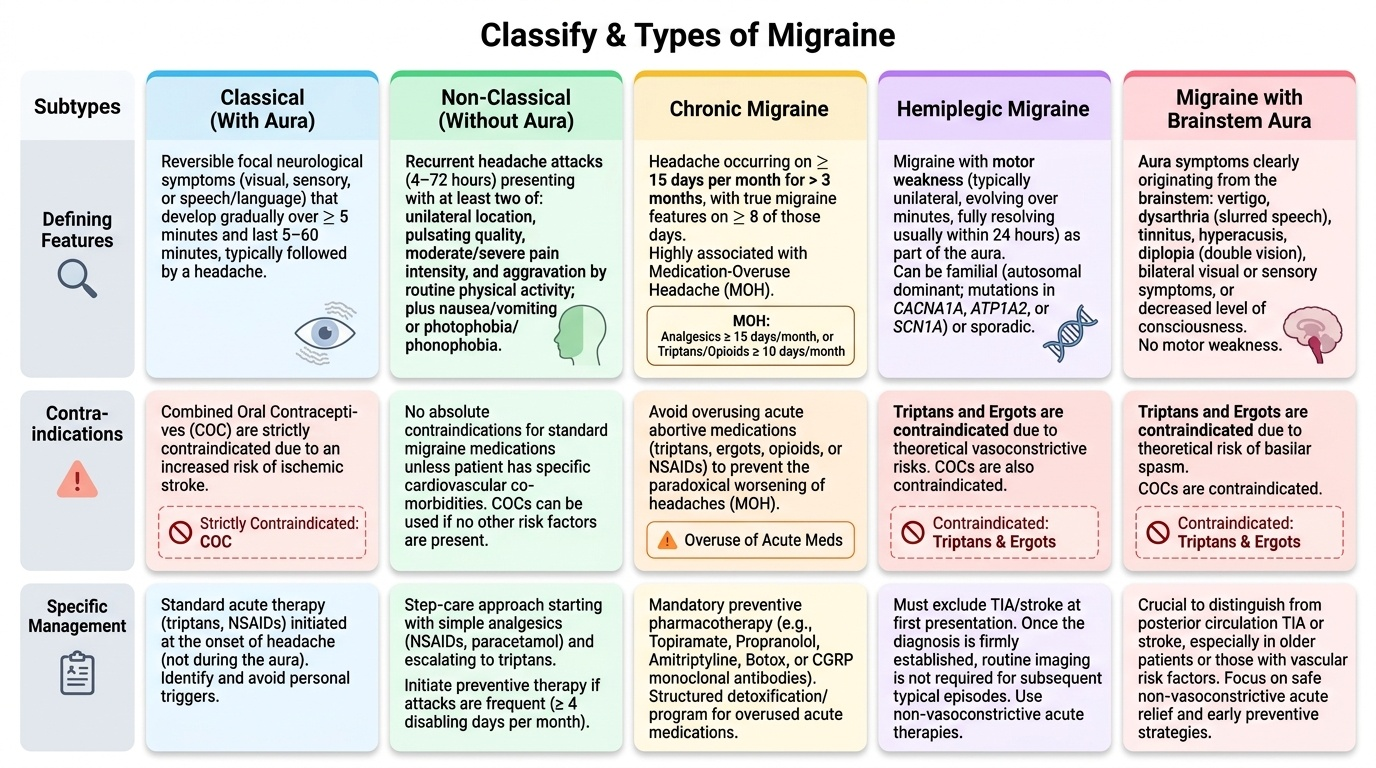
Migraine Subtypes: Classical vs Non-Classical Forms
The classification of migraine into subtypes beyond the core 'with aura' and 'without aura' categories has important clinical implications for prognosis, specific treatment choices, and contraindications. Several subtypes warrant detailed understanding at the final-year level because they present with features that may alarm the clinician or patient, and because misclassifying them as secondary headaches leads to unnecessary investigation, whereas overlooking them may delay appropriate care.
Provided image
Chronic migraine is defined by ICHD-3 as headache occurring on ≥15 days per month for more than 3 months, with migraine features on ≥8 of those days. This is a key clinical threshold because chronic migraine drives significant disability and requires preventive pharmacotherapy. A major cause of transformation from episodic to chronic migraine is medication-overuse headache (MOH) — the paradoxical worsening of headache due to overuse of acute analgesics (defined as ≥15 days/month for non-opioid analgesics/paracetamol/NSAIDs, or ≥10 days/month for triptans, ergotamine, or opioids, for >3 months). Rajesh in the opening vignette likely has MOH from near-daily NSAID use. Distinguishing chronic migraine with MOH from other causes of daily headache is a critical diagnostic task.
Migraine with brainstem aura (formerly basilar migraine) presents with aura symptoms originating in the brainstem — vertigo, diplopia, dysarthria, tinnitus, bilateral visual disturbances, bilateral sensory symptoms, or decreased level of consciousness. It must be distinguished from posterior circulation TIA and stroke, particularly in older patients or those with vascular risk factors. Triptans and ergots are contraindicated due to theoretical vasoconstrictive risk, though evidence is limited.
Hemiplegic migraine — either familial (autosomal dominant; mutations in CACNA1A, ATP1A2, or SCN1A) or sporadic — presents with motor weakness as part of the aura. The weakness is typically unilateral, evolves over minutes, and fully resolves, usually within 24 hours though occasionally persisting longer. This subtype requires exclusion of TIA/stroke at first presentation; once the diagnosis is established, further imaging is not required for typical episodes. Triptans and ergots are contraindicated.
Retinal migraine produces monocular visual disturbances (positive or negative — scintillations or scotoma) in one eye rather than the binocular visual field changes of typical visual aura, reflecting temporary ischaemia of the retinal artery. It must be differentiated from amaurosis fugax (transient monocular blindness due to carotid artery disease or cardioembolism).
Vestibular migraine is now recognised as a distinct diagnostic entity in ICHD-3 — vestibular symptoms (vertigo, positional dizziness) associated with current or prior migraine history. It is the most common cause of recurrent spontaneous vertigo in adults, often without concurrent headache, and requires awareness in an undifferentiated dizzy patient.
The clinically relevant comparison between migraine with aura ('classical') and migraine without aura ('common' or 'non-classical') is summarised as follows: aura is an additional diagnostic and risk-stratifying feature, not a severity marker. Combined oral contraceptive pills (COCs) are absolutely contraindicated in migraine with aura due to significantly increased stroke risk (approximately 8-fold increase versus non-migrainous women taking COCs) — this contraindication does NOT apply to migraine without aura. Women of reproductive age presenting with migraine must therefore have their aura status explicitly documented before prescribing contraception.
SELF-CHECK
A 24-year-old woman with a known 3-year history of migraine with visual aura requests combined oral contraceptive pills for family planning. The appropriate response is:
A. Prescribe low-dose oestrogen combined OCP as the aura is mild
B. Prescribe a progestogen-only pill instead, as COC is contraindicated in migraine with aura
C. Prescribe combined OCP for 3 months and then reassess
D. No contraceptive restriction applies to migraine — prescribe as requested
Reveal Answer
Answer: B. Prescribe a progestogen-only pill instead, as COC is contraindicated in migraine with aura
Migraine with aura is a World Health Organization Medical Eligibility Criteria Category 4 (absolute contraindication) for combined oestrogen-containing contraceptives. The risk of ischaemic stroke is approximately 8-fold higher in women with migraine with aura who take combined oestrogen-containing contraceptives versus non-migrainous women. A progestogen-only pill (or alternative non-hormonal methods) is appropriate. This contraindication does NOT apply to migraine without aura. Migraine aura status must therefore be specifically documented in every young woman being considered for combined hormonal contraception.
Red Flags in Headache: SNNOOP10 Criteria
While primary headache disorders account for the overwhelming majority of headache presentations, the potentially catastrophic consequences of missing a secondary headache make the systematic screening for red flags a mandatory step in every new headache evaluation. The SNNOOP10 mnemonic provides a structured, validated set of red-flag warning features that should prompt immediate investigation for secondary causes. The term represents 10 major clinical warning signals — each one backed by evidence that its presence increases the likelihood of a serious underlying cause disproportionately enough to warrant investigation before a primary headache label is assigned. Applying the SNNOOP10 at every first headache consultation is not defensive medicine — it is the minimum standard of care that separates a safe diagnostic approach from a dangerous one. The key clinical skill is not to memorise the 10 letters in isolation, but to understand the mechanism behind each flag and the specific secondary diagnosis it points to, so that you can order the correct targeted investigation rather than an untargeted panel. In Indian clinical practice, several of these flags carry additional weight: fever in the context of headache mandates consideration of tuberculous meningitis in addition to bacterial and viral causes; immunocompromised patients with headache must be screened for cryptococcal meningitis; and age over 50 with new headache mandates giant cell arteritis in the differential alongside intracranial malignancy.
The SNNOOP10 red flags are:
- S — Systemic symptoms: fever, weight loss, or significant comorbidity
- N — Neoplasm (history of cancer): primary or metastatic brain tumour
- N — Neurological deficit or dysfunction (including decreased consciousness)
- O — Onset: sudden/thunderclap onset (maximal pain at or within 1 minute of onset)
- O — Older age (>50 years, new headache): risk of giant cell arteritis, malignancy, subdural haematoma
- P — Pattern change or recent headache onset in a previously headache-free patient
- P — Positional headache: orthostatic (better lying down → raised ICP; worse lying down → low CSF pressure)
- E — Precipitated by Exertion (Valsalva/cough/sexual activity): posterior fossa or intracranial lesion
- E — Eye symptoms: visual changes, proptosis, painful eye (suggests glaucoma or cavernous sinus pathology)
- R — Referred headache from cervical spine or other structural causes
- R — Radiation or treatment (post-radiotherapy headache)
- R — Retinal symptoms or monocular visual loss
- R — Risk factors for immunodeficiency (HIV, immunosuppression): opportunistic CNS infection, lymphoma
The single most important red flag is the thunderclap headache — a headache that reaches maximum intensity within 60 seconds (often described as 'the worst headache of my life' or 'like being hit on the back of the head'). This presentation mandates emergency evaluation for subarachnoid haemorrhage (SAH) until proven otherwise. The standard protocol is: (1) Non-contrast CT head first — detects blood in 98% of SAH within 6 hours of onset; sensitivity falls to ~85% at 24 hours and ~50% at 1 week. (2) If CT is negative or equivocal, lumbar puncture at ≥12 hours post-onset to look for xanthochromia (yellow CSF from haemoglobin degradation products) — spectrophotometry is more sensitive than visual inspection. A normal CT + normal LP effectively excludes SAH and allows confident reassurance.
The workup for other red flags is guided by the specific feature: new headache in a patient >50 years with scalp tenderness, jaw claudication, and elevated ESR suggests giant cell arteritis (temporal arteritis) — ESR typically >50 mm/hr; treat empirically with high-dose prednisolone before biopsy to prevent blindness. Headache with fever, neck stiffness, and photophobia suggests meningitis — proceed to CT (to exclude raised ICP) then LP. Progressive headache worse in the morning with vomiting and papilloedema suggests raised ICP from a space-occupying lesion — MRI with contrast.
⚑ AI image — pending faculty review (auto-QA score 3/10; best of 3 attempts)
SNNOOP10 Headache Red Flags and SAH Workup