Page 3 of 21
IM17.{1,3} | Headache Foundations — SDL Guide (Part 3)
Diagnosis and Investigation Strategy
The diagnostic approach to headache integrates careful history-taking with judicious use of investigations. In primary headaches — migraine, tension-type, and cluster — the diagnosis is entirely clinical, based on pattern recognition against ICHD-3 criteria. Investigations are NOT required to confirm a primary headache diagnosis in a typical presentation; their role is to exclude secondary causes when red flags are present or when the clinical pattern is atypical. A common error in clinical practice is to reflexively order a CT brain for every patient presenting with headache, which wastes resources, exposes the patient to radiation, and provides false reassurance (a normal CT does not exclude SAH, meningitis, or early raised ICP from a small lesion). The correct approach is to use the clinical information gathered in the history and examination to determine which — if any — investigation is indicated, and to match the investigation to the specific secondary diagnosis under consideration. This targeted approach is both more efficient and more diagnostically reliable than a shotgun panel. The following framework structures the investigation decision systematically: first apply the SNNOOP10 red-flag screen, then determine the specific pathology suspected, then order the single most diagnostic test for that pathology before considering additional investigations.
The diagnostic decision framework operates as follows. First, apply the SNNOOP10 red-flag screen. If ANY red flag is present, proceed to targeted investigation before labelling the headache as primary:
- Thunderclap headache: non-contrast CT head → LP at ≥12 hours if CT negative → rule out SAH, cerebral venous thrombosis (CVT), pituitary apoplexy
- Fever + headache + neck stiffness: CT head to rule out raised ICP → LP for CSF analysis (cell count, protein, glucose, culture, India ink, AFB stain for TB)
- Progressive headache + papilloedema + focal deficit: MRI with gadolinium → rule out tumour, abscess, subdural haematoma
- Headache + scalp tenderness + ESR >50 + age >50: ESR, CRP, temporal artery biopsy → giant cell arteritis
- Headache + HIV or immunocompromised: India ink staining and cryptococcal antigen in CSF → cryptococcal meningitis
When to image in primary headache: The American Headache Society criteria identify the following as indications for neuroimaging in an apparently primary headache: headache always on the same side (strictly unilateral without variability), headache not responding to multiple appropriate treatments, patient or physician anxiety about an underlying cause, atypical features, first/worst headache of life, rapid increase in headache frequency, and onset of new headache in a patient with HIV or cancer.
In the Indian context, additional considerations apply: tuberculous meningitis (TBM) must be considered in any subacute or chronic headache with meningism, particularly in immunocompromised patients or those from TB-endemic areas. The CSF in TBM characteristically shows: lymphocytic pleocytosis (20–500 cells/mm³), elevated protein (100–500 mg/dL), and low glucose (CSF:serum glucose ratio <0.5). AFB smear and mycobacterial culture confirm the diagnosis; GeneXpert has improved sensitivity substantially.
For routine follow-up of established migraine, investigations are not required unless the headache pattern changes significantly (new features, increased frequency, new neurological signs).
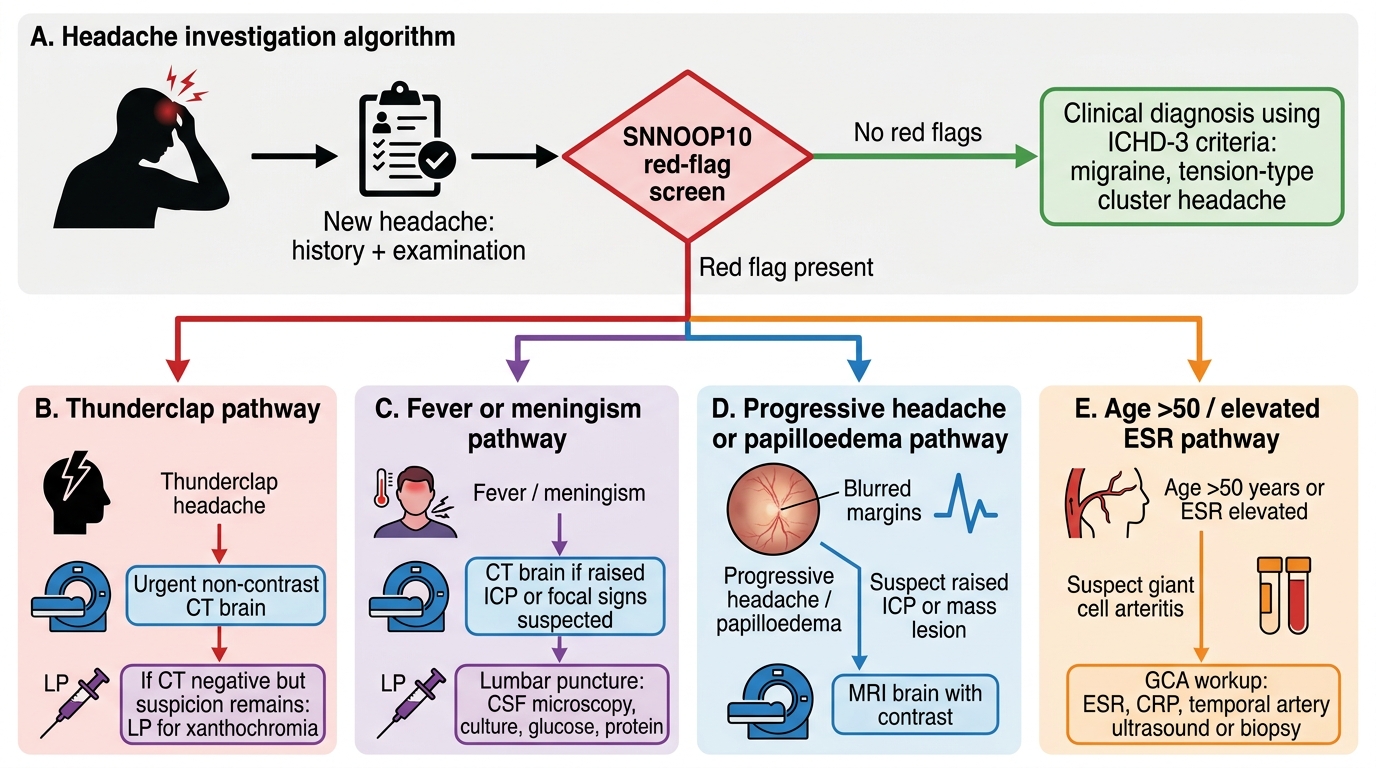
Investigation Algorithm for a New Headache
SELF-CHECK
A 50-year-old man presents to the emergency department with the 'worst headache of his life,' reaching maximum intensity within 30 seconds while straining in the toilet. He has no focal neurological deficits, no fever, and the neurological examination is normal. Non-contrast CT head is reported as normal. What is the correct next step?
A. Discharge with diagnosis of primary exertional headache and analgesia
B. Perform MRI brain with gadolinium
C. Perform lumbar puncture at ≥12 hours after headache onset to test for xanthochromia
D. Order serum ESR and CRP to rule out giant cell arteritis
Reveal Answer
Answer: C. Perform lumbar puncture at ≥12 hours after headache onset to test for xanthochromia
A thunderclap headache — maximal intensity within 60 seconds — is a medical emergency and must be assumed to be subarachnoid haemorrhage (SAH) until proven otherwise. A normal CT does NOT exclude SAH, especially if performed early or if the subarachnoid blood volume is small. The sensitivity of CT for SAH is ~98% within 6 hours but falls to ~85% by 24 hours. Lumbar puncture at ≥12 hours post-onset is the definitive next step — xanthochromia (detected by spectrophotometry) indicates prior subarachnoid blood. Discharging this patient with 'primary exertional headache' without LP is dangerous. MRI does not reliably detect acute subarachnoid blood. GCA is unlikely at 50 and does not present as a thunderclap headache.
Management Overview: Migraine, TTH, and Cluster
A comprehensive management plan for primary headache addresses three goals: accurate diagnosis (already established through classification), acute treatment of individual attacks, and prevention of recurrence where attacks are frequent or severely disabling. At the foundation level this module establishes the framework; the detailed pharmacology is addressed in the headache-treatment module.
Provided image
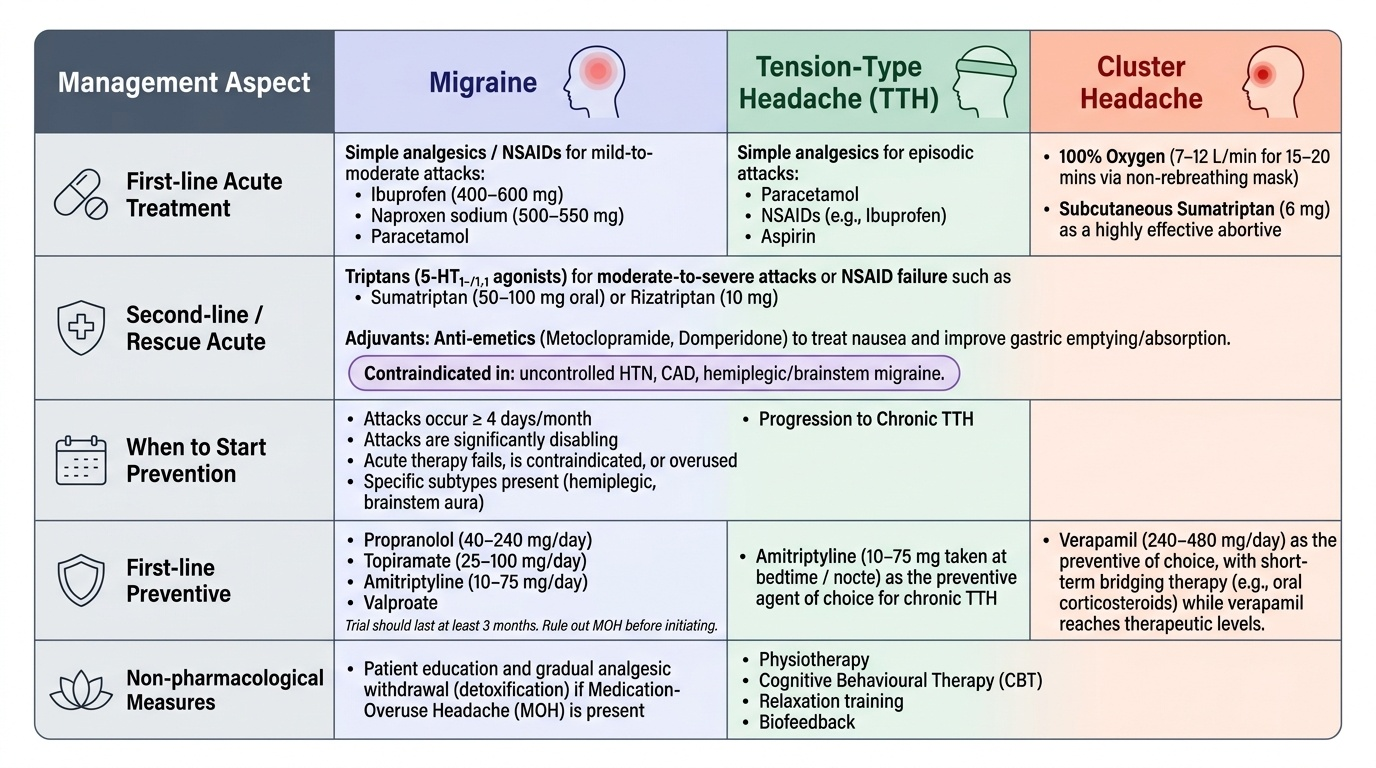
Migraine — acute (abortive) therapy aims to abort an individual attack. The stepwise approach begins with NSAIDs (ibuprofen 400–600 mg, naproxen sodium 500–550 mg) or paracetamol for mild-to-moderate attacks. For moderate-to-severe attacks or NSAID failure, triptans (selective 5-HT₁B/₁D agonists) are first-line: sumatriptan 50–100 mg oral; rizatriptan 10 mg. Triptans are contraindicated in uncontrolled hypertension, coronary artery disease, haemiplegic migraine, and migraine with brainstem aura. Anti-emetics (metoclopramide, domperidone) both treat nausea and improve oral drug absorption via improved gastric emptying.
Migraine prevention is indicated when attacks occur ≥4 days/month, when attacks are significantly disabling, when acute therapy fails or is overused, or when certain subtypes (hemiplegic, brainstem aura) are present. First-line preventive agents are propranolol (40–240 mg/day), topiramate (25–100 mg/day), amitriptyline (10–75 mg/day), and valproate. Second-line: candesartan, lisinopril. Newer: monoclonal antibodies against CGRP pathway (erenumab, fremanezumab, galcanezumab) — not yet widely available in India. A prevention trial should last at least 3 months.
Medication-overuse headache (MOH) requires patient education and gradual analgesic withdrawal — the primary treatment is detoxification. Continuing analgesics while adding preventives is futile if MOH is present.
Tension-type headache: simple analgesics (paracetamol, NSAIDs, aspirin) are effective for episodic attacks. Amitriptyline (10–75 mg nocte) is the preventive of choice for chronic TTH. Physiotherapy, cognitive behavioural therapy, relaxation training, and biofeedback are non-pharmacological options.
Cluster headache — acute: 100% oxygen via non-rebreathing mask (7–12 L/min for 15–20 minutes) is first-line; subcutaneous sumatriptan 6 mg is the most effective abortive. Preventive: verapamil (240–480 mg/day) is the agent of choice; short-term bridge with a tapering prednisolone course during cluster periods.
Self-Assessment: Applying Headache Classification
The competencies IM17.1 and IM17.3 are assessed at the KH (Knowledge applied to clinical scenarios) level, meaning you are expected to take a headache history, classify the headache syndrome, and justify your classification using ICHD-3 criteria. The following integrative scenarios consolidate your learning from this module.
Scenario A: A 28-year-old teacher has had recurrent headaches since age 18. Each episode begins with 20 minutes of visual disturbance (zigzag lines on the right side of her visual field), followed within 30 minutes by a throbbing right-sided headache of severe intensity, nausea, and inability to face bright light, lasting 8 hours. She has approximately 2 attacks per month.
Classification: Migraine with typical visual aura (ICHD-3 code 1.2.1). Justification: ≥5 attacks, each with a visual aura lasting <60 minutes developing gradually (zigzag scotoma), followed within 60 minutes by headache meeting migraine criteria (unilateral, pulsating, severe, photophobia, nausea). Frequency: 2/month — episodic migraine, preventive therapy threshold not yet met but worth counselling about if worsening.
Scenario B: A 40-year-old male office worker presents with bilateral pressure headache, band-like, mild-to-moderate intensity, occurring almost daily for 2 years, lasting 4–6 hours. No nausea, no vomiting. He has mild photophobia sometimes. He takes ibuprofen almost daily, 15 days per month. Neurological examination is normal.
Classification: Chronic tension-type headache with probable medication-overuse headache (MOH). Justification: bilateral, pressure quality, mild-to-moderate, no nausea, no aggravation by activity = TTH features; occurring ≥15 days/month for >3 months = chronic TTH. Ibuprofen ≥15 days/month for >3 months = MOH (NSAID-type). First management priority: education about MOH and analgesic detoxification.
Scenario C: A 35-year-old male presents with a cluster of severe, right-sided periorbital pain lasting 45–60 minutes, occurring once to twice nightly for the past 3 weeks, waking him from sleep. He is unable to stay still during attacks and paces the room. He has right-sided lacrimation and nasal stuffiness. He had a similar cluster 2 years ago, then was completely headache-free.
Classification: Episodic cluster headache (ICHD-3 code 3.1.1). Justification: strictly unilateral severe periorbital pain lasting 15–180 minutes (45–60 min), with ipsilateral lacrimation and nasal congestion (cranial autonomic features), restlessness during attacks, periodicity (3-week cluster with prior remission). Acute treatment: 100% oxygen + subcutaneous sumatriptan. Prophylaxis: verapamil.
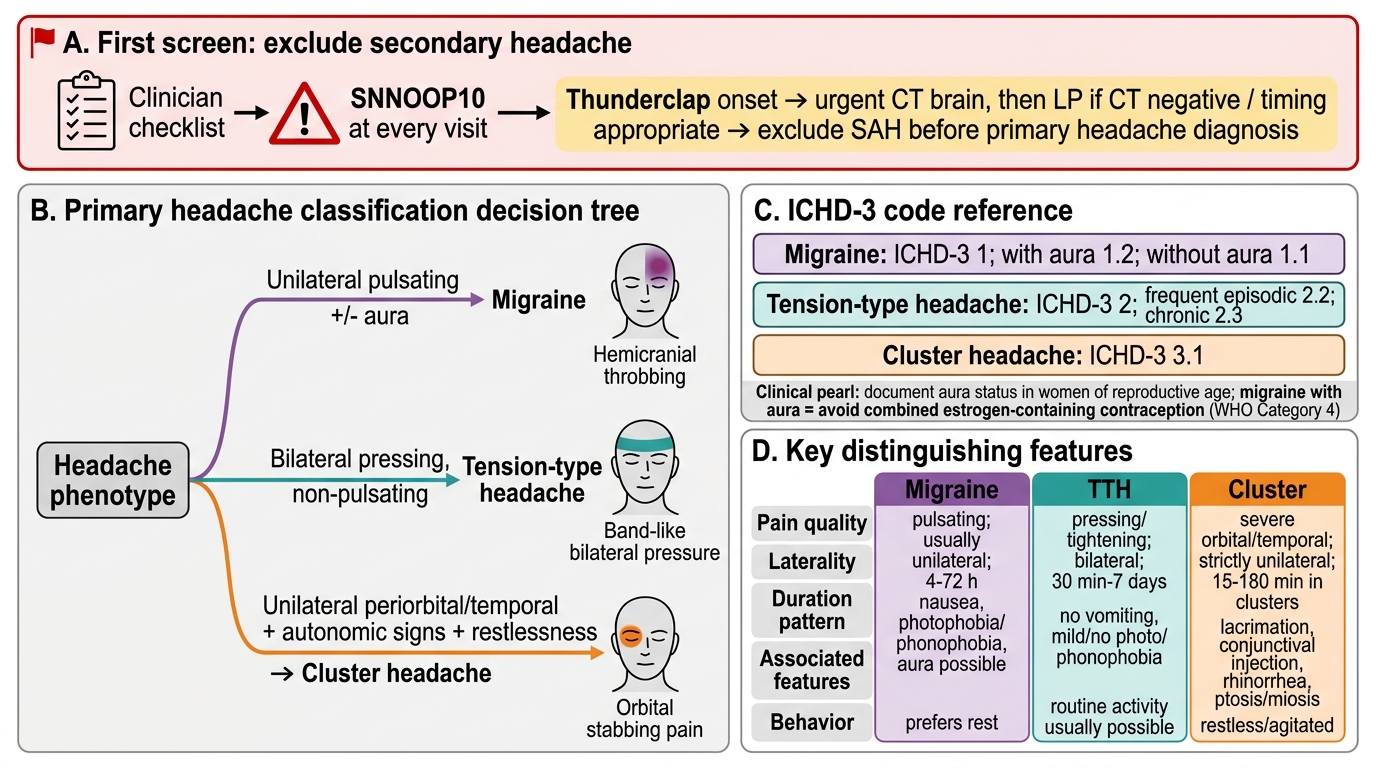
Primary Headache Classification Decision Tree
CLINICAL PEARL
The single most important clinical pearl in headache medicine is the distinction between primary and secondary headache — and the tool that makes this distinction possible is the systematic SNNOOP10 red-flag screen applied at every headache consultation, not just at the first visit. The most dangerous cognitive trap is pattern-matching a 'thunderclap' headache to 'exertional' or 'primary thunderclap' headache without performing the mandatory CT then LP protocol for SAH. Subarachnoid haemorrhage has a re-bleed risk of 20–30% in the first 24 hours, and a missed SAH that re-bleeds carries 40–50% mortality. No level of diagnostic confidence in a primary headache pattern excuses omitting this investigation in a thunderclap onset.
A second high-yield pearl: migraine with aura is an absolute contraindication to combined oestrogen-containing contraceptives. This is a WHO Category 4 contraindication because of the significantly elevated stroke risk. In a busy outpatient clinic, this fact is often overlooked — always document aura status in women of reproductive age presenting with migraine before any contraceptive prescription.