Page 4 of 21
IM18.3-7 | Stroke Clinical Evaluation — SDL Guide
Learning Objectives
- Elicit, document, and present a focused stroke history including last-known-well time, deficit characterisation, vascular risk factors, medications, and contraindications to thrombolysis
- Perform a systematic neurological examination in a stroke patient using the NIHSS framework — consciousness, gaze, visual fields, facial palsy, motor, coordination, sensation, language, dysarthria, and neglect
- Localise the lesion based on UMN vs LMN pattern, side, and anatomical level using clinical signs — distinguishing cortical, capsular, brainstem, and cerebellar syndromes
- Distinguish and classify the major aphasia syndromes (Broca's, Wernicke's, global, conduction) by fluency, comprehension, and repetition, and localise each to the appropriate cortical region
- Describe the patterns of neurogenic bladder dysfunction associated with upper and lower motor neuron lesions
INSTRUCTIONS
This skills module builds the practical clinical assessment framework for the stroke patient. Work through each section with a simulated patient or mannequin if available. The NIHSS scoring items correspond directly to the examination steps described — practise calculating an NIHSS score from the clinical vignettes provided. The aphasia classification section requires repeated active recall: cover the table and see if you can generate each syndrome's features from the lesion location.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 427 — Clinical Examination in Stroke and Chapter on Aphasia (textbook)
- API Textbook of Medicine, 10th ed. — Neurological Examination (textbook)
- AHA/ASA 2019 Acute Ischaemic Stroke Guidelines — Section on Clinical Assessment and NIHSS (guideline)
- DeMyer's The Neurological Examination: A Programmed Text, 7th ed. (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
You are called to see a 68-year-old woman in the emergency department. The triage nurse says 'she can't speak properly and her right arm is weak.' You have about eight minutes to take a focused history, perform a targeted neurological examination, calculate an NIHSS score, localise the lesion, and determine whether she is a thrombolysis candidate — all before the CT scanner is available. Her daughter is with her and is extremely distressed. The patient attempts to speak when you greet her but produces only unintelligible sounds, though she nods when you ask if she understands you. Her right arm falls immediately when you ask her to hold it up. The right nasolabial fold is flattened. You note the time: 09:43 am. The family says she was speaking normally at breakfast at 08:10 am. Every question you ask in the next eight minutes must count. What do you ask? What do you examine? How do you document it? And critically — can she still tell you what happened, even if she can't use words? This module trains the systematic clinical evaluation of the stroke patient.
WHY THIS MATTERS
The clinical evaluation of a stroke patient is the most consequential skill assessment in emergency medicine. It determines the diagnosis, drives the imaging strategy, establishes the NIHSS baseline that all future decisions are compared against, and generates the documentation that medicolegal scrutiny will focus on. The NMC competencies IM18.3–IM18.7 require you to elicit, document, and present the stroke history and neurological examination at the SH (Skills and History-taking) level — meaning you must be able to perform these skills under supervision in a real patient encounter, not merely describe them. For a final-year student rotating through medicine and neurology, the ability to conduct a rapid, systematic, well-documented neurological examination in a stroke patient is a day-one requirement. The examination must be efficient enough to be completed in the acute setting without delaying reperfusion, yet complete enough to localise the lesion and establish the severity baseline.
RECALL
Before proceeding, activate your prior knowledge of the neurological examination from your earlier medicine postings. Recall the upper motor neuron (UMN) pattern: spastic weakness, hyperreflexia, extensor plantar response (Babinski sign), and loss of fine voluntary control — this is the pattern produced by any lesion above the anterior horn cell. Contrast it with the lower motor neuron (LMN) pattern: flaccid weakness, hyporeflexia, fasciculations, and muscle wasting. Recall that in an acute stroke, the reflexes may initially be reduced or absent due to diaschisis (physiological disconnection shock), and hyperreflexia develops only over hours to days — so an acutely flaccid limb with an extensor plantar response is still a UMN lesion. Also recall the concept of crossed signs in brainstem lesions: ipsilateral cranial nerve involvement with contralateral body involvement, because the cranial nerve nuclei are at the level of the lesion while the long tracts cross below. Recall the locations of Broca's and Wernicke's areas, and what aphasia means: a disorder of language (not merely speech articulation) affecting comprehension, expression, repetition, naming, reading, or writing.
Taking a Focused Stroke History
The stroke history in the acute setting must achieve three goals simultaneously: establish the onset time (which governs thrombolysis eligibility), characterise the neurological deficit (which guides lesion localisation before imaging), and identify contraindications to thrombolysis or other therapies. It must be accomplished within minutes and may need to be taken from a relative or bystander if the patient has aphasia or reduced consciousness. Practising a structured, memorised approach — rather than improvising — is essential under acute time pressure.
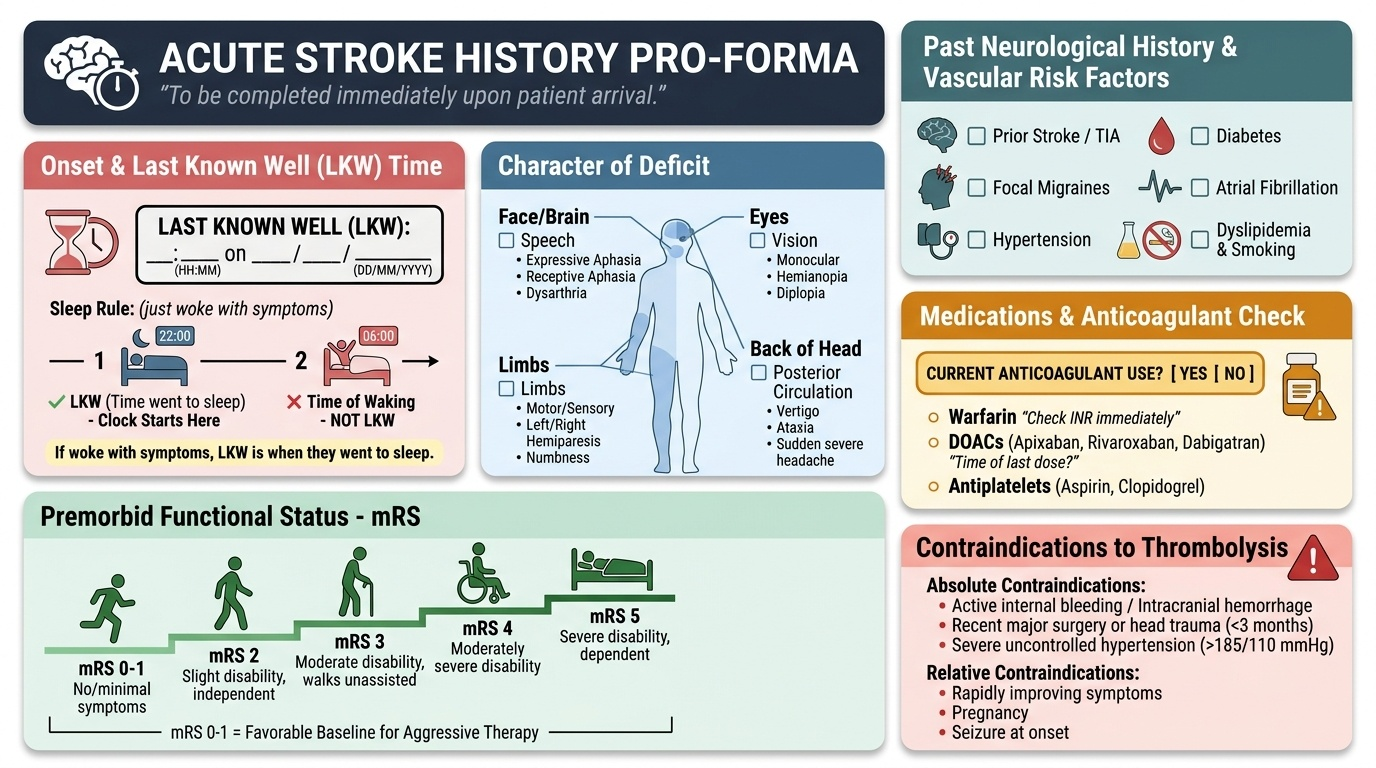
Provided image
Onset and progression — the most critical data point:
The first and most important question is: when was the patient last seen or known to be well? This is the last-known-well (LKW) time, not the time symptoms were first noticed. If a patient wakes from sleep with a stroke, the LKW time is when they went to sleep — not the time of waking. This is because the stroke could have occurred any time during sleep. For thrombolysis, the clock starts from the LKW time; a wake-up stroke where the patient was last seen well 8 hours earlier is outside the 4.5-hour window for IV thrombolysis (though DWI/FLAIR mismatch on MRI can identify patients with small DWI lesion and negative FLAIR who may still be treated). The onset must be documented in the notes as: 'last known well: HH:MM on DD/MM/YYYY.' The mode of onset is characteristically sudden in stroke (seconds to minutes) — a focal deficit that develops over hours or progresses stepwise over days is more likely a mass lesion, abscess, or Todd's paresis.
Key historical features to document:
- Character of the deficit: weakness (which limbs? how severe?), speech difficulty (unable to find words = expressive aphasia? unable to understand = receptive aphasia? slurred but fluent = dysarthria?), visual symptoms (one eye or both? visual field loss or diplopia?), headache (sudden severe headache suggests SAH or large ICH), dizziness/vertigo (posterior circulation?), loss of consciousness (suggests large hemispheric, basilar, or ICH), sensory symptoms (numbness, tingling), swallowing difficulty, ataxia
- Previous neurological episodes (prior TIA or stroke — establishes vascular disease; focal migraines — differential)
- Vascular risk factors: hypertension (current BP medications?), diabetes, AF (on anticoagulant?), dyslipidaemia, smoking, prior cardiac disease or valve surgery
- Medications: anticoagulants (warfarin — need INR; DOACs — last dose and when), antiplatelets, antihypertensives, insulin/oral hypoglycaemics
- Contraindications to thrombolysis: recent surgery (within 14 days), recent significant trauma, active bleeding, prior intracranial haemorrhage, recent stroke within 3 months, known coagulopathy, uncontrolled blood pressure
- Functional baseline: was the patient independent before this event? What is the premorbid modified Rankin Scale (mRS) — a patient who was already severely disabled (mRS 4–5) may not benefit from thrombolysis
When the patient has aphasia, take the history from the family or bystander, but also attempt to assess the patient's comprehension by asking simple yes/no questions and following commands. Document both what the patient communicates and what the informant reports. Never assume a patient with aphasia has impaired comprehension — many patients with Broca's (expressive) aphasia have preserved understanding and are acutely aware of their situation.
Neurological Examination in Stroke — Systematic Approach
The neurological examination in a stroke patient must be systematic, reproducible, and efficient. In the acute setting it should be completed within 5–8 minutes. The examination follows a standard sequence and directly generates the NIHSS score — so learning the NIHSS structure is simultaneously learning the examination.
General and vital signs (always examine first):
Blood pressure (both arms if time permits — difference >20 mmHg suggests aortic dissection, an important stroke mimic), heart rate and rhythm (irregular pulse → AF), temperature (fever = infection driving encephalopathy?), oxygen saturation, and blood glucose (point-of-care glucose is mandatory — hypoglycaemia is the most important reversible stroke mimic and must be checked before CT). On general examination, assess for signs of cardiac disease (murmurs suggesting valvular disease, atrial fibrillation on auscultation), evidence of peripheral vascular disease, carotid bruits (though a bruit does not correlate reliably with significant stenosis), and skin (petechiae suggesting endocarditis, livedo reticularis suggesting APS).
Level of consciousness (GCS and NIHSS 1a/1b/1c):
Assess using the Glasgow Coma Scale (eye opening, verbal response, motor response) and the first three NIHSS items: level of consciousness (0=alert; 1=arousable by minor stimulation; 2=obtunded requiring repeated stimulation; 3=responds only reflexively or unresponsive), LOC questions (what month and how old? 0=both correct; 1=one correct; 2=neither), and LOC commands (open/close eyes, grip/release hand; 0=both; 1=one; 2=neither). Reduced consciousness in a patient who appeared clinically to have a cortical stroke suggests either a very large hemisphere infarct with mass effect, a thalamic or brainstem infarct, or a haemorrhagic component.
Cranial nerves (focused on stroke-relevant findings):
- Gaze (NIHSS 2): assess horizontal gaze. Conjugate gaze deviation (both eyes deviated to one side) = frontal lobe lesion in ipsilateral hemisphere or pontine lesion on the contralateral side. Inability to cross the midline = internuclear ophthalmoplegia (MLF lesion, brainstem). A patient with left MCA infarct looks toward the lesion (away from the hemiplegia) because the frontal eye field normally drives gaze to the contralateral side; when destroyed, gaze is directed to the ipsilateral (intact) side
- Visual fields (NIHSS 3): use confrontation — compare each quadrant in each eye. Homonymous hemianopia (same half of visual field in both eyes, right or left) = contralateral hemispheric or optic radiation or occipital cortex lesion. Assess whether macular sparing is present (preserved central vision in hemianopia = occipital cortex lesion with dual blood supply at the tip)
- Facial palsy (NIHSS 4): ask patient to show teeth and close eyes tightly. UMN facial palsy (forehead sparing — upper face bilateral cortical representation) = contralateral hemisphere lesion. LMN facial palsy (forehead involved) = ipsilateral facial nerve nucleus (pons) or nerve trunk lesion. In stroke, you will virtually always see UMN pattern (forehead sparing) for hemispheric lesions; complete facial palsy including forehead = pontine lesion
- Pupillary responses: miosis with ptosis and anhidrosis = Horner syndrome (ipsilateral sympathetic pathway lesion — lateral medulla, hypothalamus, or neck); fixed dilated pupil = compression of CN III (uncal herniation — emergency)
- Hearing, taste, smell: usually not tested in the acute setting unless posterior fossa syndrome is suspected
Motor examination (NIHSS 5–6):
Test each limb individually. The standard NIHSS motor test: hold the arm at 90° (sitting) or 45° (supine) — does it drift down within 10 seconds? 0=no drift; 1=drifts but not to bed; 2=some anti-gravity effort; 3=no effort against gravity; 4=no movement. For legs: hold at 30° supine — drift within 5 seconds? Same scoring. Document power in each limb using the MRC scale (0=no contraction; 1=flicker; 2=movement with gravity eliminated; 3=movement against gravity; 4=movement against resistance; 5=normal). Upper limb pronator drift (ask patient to hold arms outstretched with palms up, eyes closed — the affected limb pronates and drifts down) is a sensitive test for mild corticospinal lesion.
Coordination (NIHSS 7):
Finger-nose-finger and heel-shin tests. Ataxia is scored only if present out of proportion to weakness (if the patient is too weak to move, ataxia cannot be scored). Ipsilateral limb ataxia = ipsilateral cerebellar lesion or superior cerebellar artery territory. Cerebellar gait ataxia (wide-based, staggering, falls to one side) suggests posterior circulation stroke.
Sensory examination (NIHSS 8):
Test pinprick sensation (representing spinothalamic tract). Hemisensory loss = contralateral thalamic, sensory cortex, or internal capsule lesion. Dissociated sensory loss (spinothalamic on one side of body, dorsal column on the other) = brainstem lesion at the decussation levels.
Language and speech (NIHSS 9–10):
Language (aphasia) is assessed by asking the patient to name objects, repeat a sentence, read a standard sentence, and follow commands. Speech (dysarthria) is assessed by articulation quality. These are distinguished and scored separately in the NIHSS.
Extinction and inattention (NIHSS 11):
Double simultaneous stimulation — touch both hands simultaneously; does the patient neglect one side? Neglect (hemispatial inattention) is seen with right parietal lesions; the patient ignores the left side of space and may even deny the weakness (anosognosia).
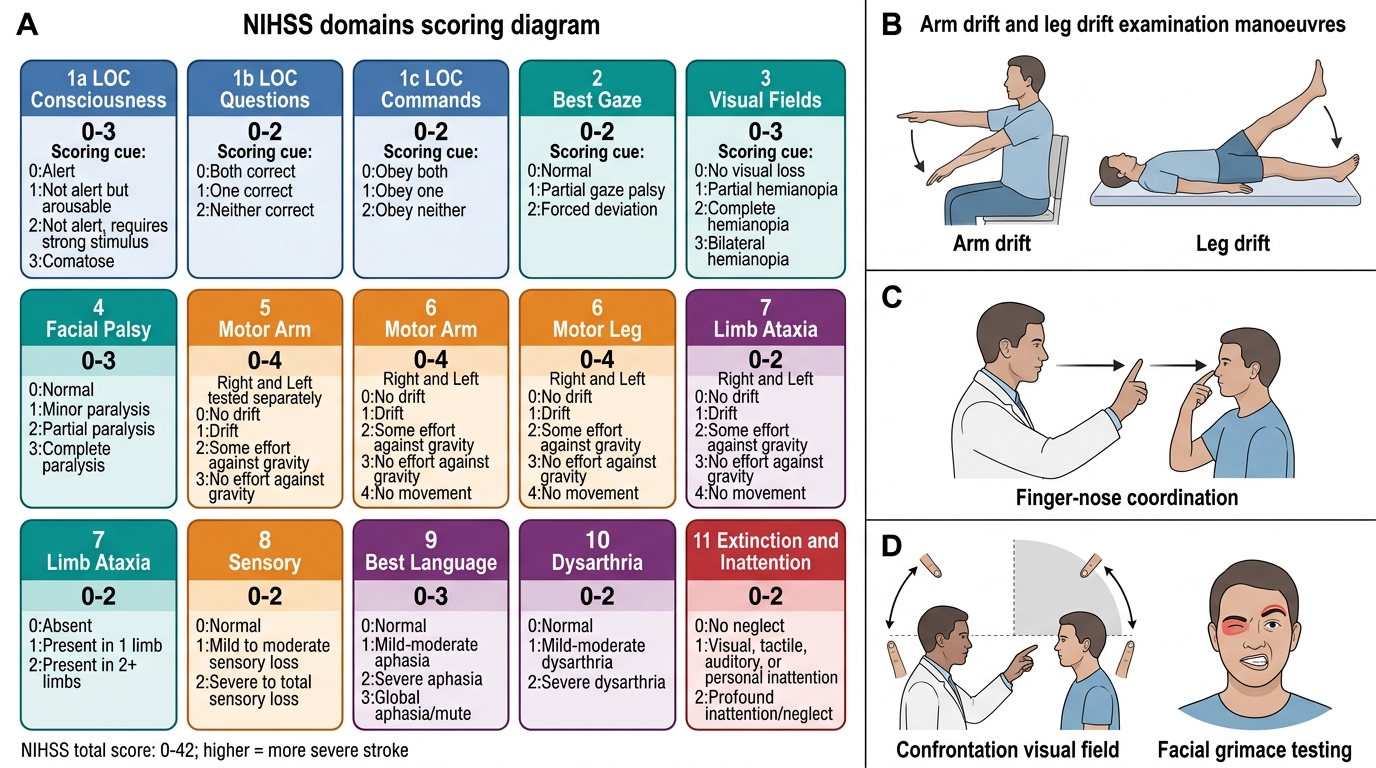
NIHSS Domains and Key Stroke Examination Manoeuvres
SELF-CHECK
A 72-year-old woman is brought with sudden-onset right-sided weakness and inability to speak. On examination she cannot name objects shown to her, cannot repeat a sentence, and does not follow commands. Her right arm and leg have grade 3/5 power. Pupils are equal and reactive. There is no facial droop. What pattern of language deficit does she have, and where in the brain is the lesion most likely located?
A. Expressive (Broca's) aphasia — posterior inferior frontal gyrus, left hemisphere
B. Receptive (Wernicke's) aphasia — posterior superior temporal gyrus, left hemisphere
C. Global aphasia — large left MCA territory involving both Broca's and Wernicke's areas
D. Dysarthria — left internal capsule
Reveal Answer
Answer: C. Global aphasia — large left MCA territory involving both Broca's and Wernicke's areas
Global aphasia involves all language functions — production, comprehension, repetition, and naming are all impaired. This occurs with a large left MCA territory infarct that destroys both Broca's area (inferior frontal gyrus) and Wernicke's area (superior temporal gyrus) along with the arcuate fasciculus connecting them. Pure Broca's aphasia spares comprehension (patient understands but cannot produce fluent speech). Pure Wernicke's aphasia impairs comprehension but production is fluent (though paraphasic — wrong words). Dysarthria is a motor speech disorder — articulation is impaired but language content is intact; the patient would be able to name, repeat, and follow commands. The absence of facial droop here is a distractor — global aphasia can exist with or without prominent facial palsy.
Lesion Localisation — UMN vs LMN, Side, Site, and Nature
The ability to localise the lesion from clinical signs — before imaging — is the defining cognitive skill of the neurologist and the examining physician in a stroke encounter. It relies on three sequential questions: (1) Is this an upper motor neuron (UMN) or lower motor neuron (LMN) lesion? (2) What side and level is the lesion at? (3) What is the most probable nature (ischaemic infarct, haemorrhage, demyelination, tumour)? In stroke, the answer to question 3 is largely determined by the clinical context, onset characteristics, and risk factors — imaging then confirms it.
UMN versus LMN localisation:
The fundamental distinction is that UMN lesions occur anywhere from the motor cortex to the synapse with the anterior horn cell (or cranial nerve motor nucleus), while LMN lesions occur at or below the anterior horn cell. In stroke, virtually all motor deficits are UMN. The UMN pattern in the acute phase of stroke may appear flaccid (due to diaschisis), making the distinction from LMN lesion difficult at initial presentation. The key distinguishing feature that persists even in the acute flaccid stage is the extensor plantar response (Babinski sign) — an upgoing great toe with fanning of the other toes on stroking the lateral sole. A Babinski sign in the context of acute-onset hemiplegia = UMN lesion = stroke until proven otherwise.
Other features that help in the acute stroke examination:
- Deep tendon reflexes may be reduced acutely (diaschisis) but will increase over hours to days
- Clonus is a late sign, not expected in the acute phase
- Loss of fine voluntary control (inability to perform finger-thumb opposition) may be present even when gross strength is preserved (corticospinal tract lesion)
Determining the side of the lesion:
The corticospinal tract crosses (decussates) at the medullary-cervical junction. Therefore, all supratentorial (above the pons) UMN lesions cause contralateral weakness. Pontine and below lesions cause ipsilateral weakness of the face (cranial nerve nuclei at the pontine level, above the decussation of cranial nerve fibres) with contralateral body weakness — the crossed pattern. The pattern of lateralisation:
- Left hemisphere lesion (most common dominant hemisphere): right hemiplegia/hemisensory loss, right visual field loss (right homonymous hemianopia), and — crucially — language deficit (aphasia). In approximately 95% of right-handed individuals and 70% of left-handed individuals, the left hemisphere is dominant for language.
- Right hemisphere lesion: left hemiplegia/hemisensory loss, left visual field loss, and — importantly — neglect (hemispatial inattention to the left side), constructional apraxia, and anosognosia (denial of illness/deficit). Right hemisphere strokes are often UNDER-estimated in severity because the deficits of neglect and anosognosia are less immediately apparent than aphasia.
- Brainstem lesion (crossed signs): ipsilateral cranial nerve palsy + contralateral hemiplegia. The specific cranial nerve involved points to the anatomical level: CN III = midbrain (Weber syndrome: ipsilateral CN III palsy + contralateral hemiplegia); CN VI or VII = pons (Millard-Gubler syndrome); CNs IX, X, XI, and Horner = lateral medulla (Wallenberg syndrome).
- Cerebellum: ipsilateral limb ataxia, gait ataxia, dysarthria (scanning speech), nystagmus — NO hemiplegia (the cerebellum has no corticospinal fibres).
Determining the anatomical level and site:
Cortex vs subcortex (capsule) vs brainstem distinction:
- Cortex: focal signs matching a functional zone + cortical features (aphasia, neglect, seizures, conjugate gaze deviation)
- Internal capsule: dense hemiplegia affecting face, arm, and leg equally (because all motor fibres are packed into the posterior limb) WITHOUT cortical features
- Brainstem: crossed signs, specific cranial nerve syndromes, gaze palsies, altered consciousness from reticular activating system involvement
- Thalamus: hemisensory loss (all modalities), thalamic pain (delayed), memory disturbance (if bilateral)
- Cerebellum: pure ipsilateral ataxia without pyramidal signs
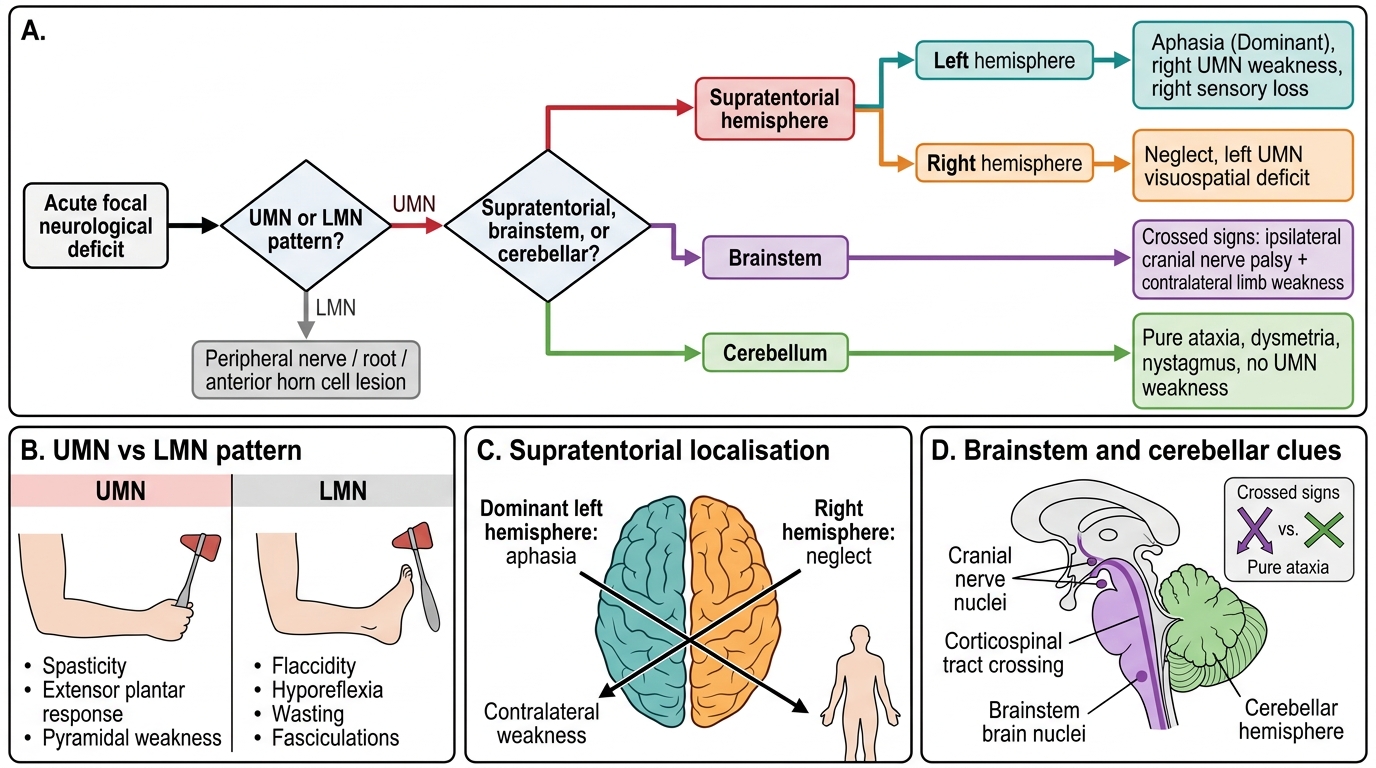
Stroke Lesion Localisation Decision Tree