Page 5 of 21
IM18.3-7 | Stroke Clinical Evaluation — SDL Guide (Part 2)
Speech and Language Disorders in Stroke
Disorders of speech and language in stroke are among the most distressing features for patients and families, and among the most diagnostically valuable signs for the examining physician. It is critical to distinguish aphasia (a disorder of language processing) from dysarthria (a motor disorder of speech articulation) and from dysphonia (a disorder of vocal production). Each points to a different anatomical lesion and has different prognostic and management implications. A patient who is aphasic is not merely 'confused' or 'demented' — the language network in the brain has been directly damaged, and the patient may have fully intact cognition in all non-linguistic domains.
Provided image
Aphasia is defined as an acquired impairment of language production, comprehension, repetition, naming, reading, or writing caused by brain damage. In clinical practice it is assessed along the following axes:
- Fluency — Is spontaneous speech output fluent (normal rate, normal phrase length, effortless) or non-fluent (slow, effortful, reduced phrase length, agrammatic)?
- Comprehension — Can the patient follow simple commands (close your eyes, hold up two fingers)? Complex commands? Does the response to yes/no questions correlate with reality?
- Repetition — Can the patient accurately repeat a simple phrase (e.g., 'no ifs, ands, or buts')?
- Naming — Can the patient name common objects shown to them (pen, watch, coin)?
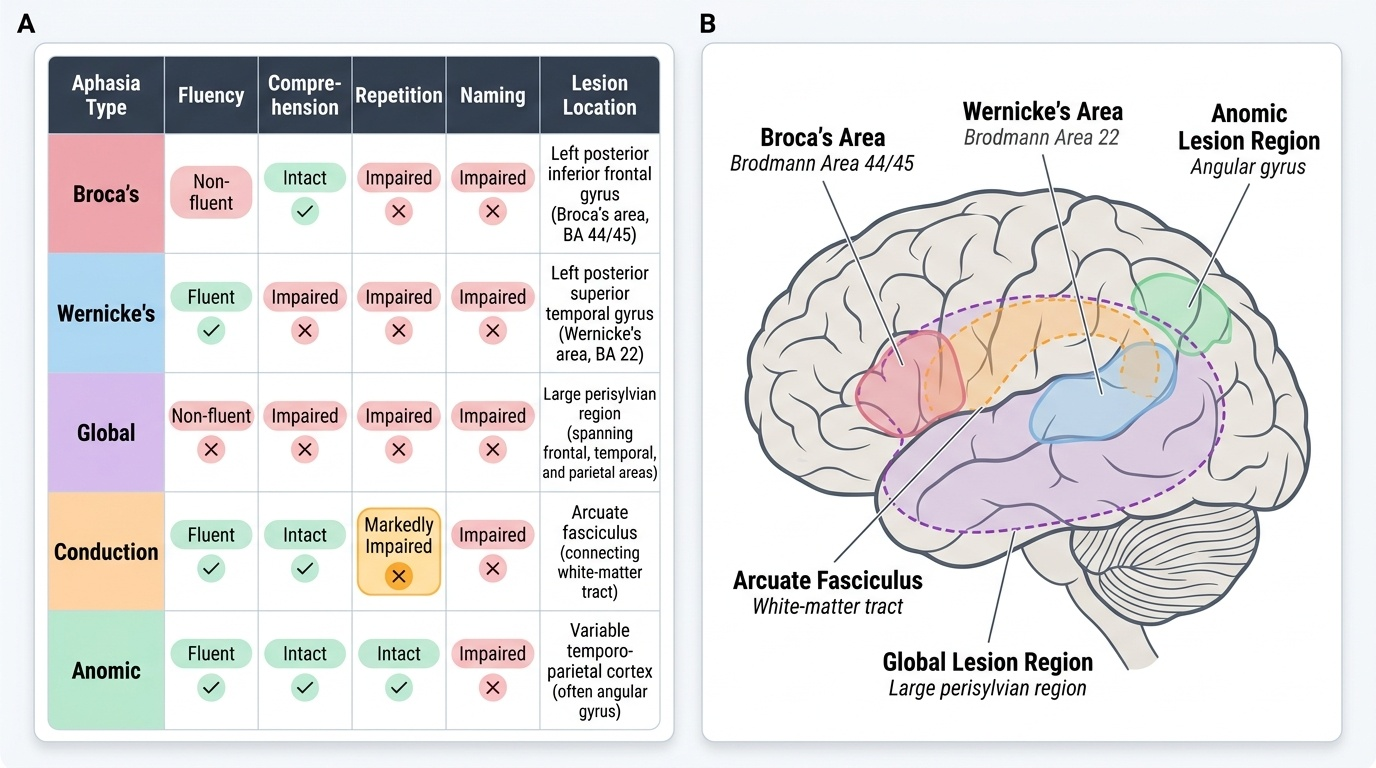
The major aphasia syndromes and their localisation:
- Broca's aphasia (expressive/non-fluent aphasia): non-fluent, effortful speech; comprehension largely intact; repetition impaired; naming impaired; patient is typically frustrated and aware of the problem (which is important for counselling and prognosis). Lesion: posterior inferior frontal gyrus (Broca's area, Brodmann areas 44/45), left hemisphere. Commonly associated with right hemiplegia because Broca's area is close to the motor cortex face/arm representation in the left frontal lobe.
- Wernicke's aphasia (receptive/fluent aphasia): fluent output but paraphasic (wrong words — phonemic paraphasias: 'tork' for 'fork'; semantic paraphasias: 'spoon' for 'fork'; neologisms: made-up words); comprehension severely impaired; repetition impaired; naming impaired. The patient is unaware of the errors (anosognosia for the language deficit) and may appear agitated or paranoid if their utterances are met with confusion. Lesion: posterior superior temporal gyrus (Wernicke's area, Brodmann area 22), left hemisphere. Patients with pure Wernicke's aphasia often have NO hemiplegia (because the temporal lobe is far from the motor cortex) — a Wernicke's aphasic patient with fluent, paraphasic speech and no weakness is at high risk of being labelled 'confused' rather than 'aphasic.'
- Global aphasia: all language functions severely impaired (production, comprehension, repetition, naming). Large left MCA territory infarct destroying both frontal and temporal language areas. Usually accompanied by right hemiplegia and right hemianopia.
- Conduction aphasia: fluent speech, intact comprehension, markedly impaired repetition (the signature finding). Caused by damage to the arcuate fasciculus (the white matter bundle connecting Broca's and Wernicke's areas through the parietal lobe). Patients make frequent phonemic paraphasias and self-correct repeatedly.
- Anomic aphasia: fluent speech, intact comprehension and repetition, but prominent difficulty naming objects (word-finding pauses, circumlocution). The mildest aphasia type; can occur with lesions in several left hemisphere locations.
Dysarthria is impaired articulation without impairment of language content. The patient can name, repeat, comprehend, and write — but the mechanical production of speech sounds is abnormal:
- Spastic dysarthria (UMN lesion of corticobulbar tract): slow, strained, effortful speech — pseudobulbar palsy; often associated with dysphagia, exaggerated jaw jerk
- Ataxic dysarthria (cerebellar): scanning speech — irregular, varying volume, imprecise consonants; slurred
- Flaccid dysarthria (LMN/bulbar: CN IX, X, XII nuclei): hypophonic, nasal (palatal incompetence), breathy
In the NIHSS, dysarthria is scored item 10 (0=normal; 1=mild to moderate slurring; 2=near-unintelligible or mute) and language is scored item 9 (0=normal; 1=mild to moderate aphasia; 2=severe aphasia — fragments only; 3=mute/global aphasia/coma).
Bladder dysfunction in neurological disease (IM18.7):
Stroke and other neurological diseases produce characteristic patterns of bladder dysfunction based on the level of the lesion. The normal bladder is under both voluntary (cortex) and reflex (sacral spinal cord S2–S4) control. Neurological bladder dysfunction is classified as:
- Uninhibited/UMN bladder (suprasacral lesion — most strokes): the sacral detrusor reflex is intact but cortical inhibition is lost → urge incontinence and urinary frequency. The bladder contracts prematurely at low volumes. This is the commonest pattern after stroke.
- Flaccid/LMN bladder (sacral cord or cauda equina lesion): detrusor areflexia → urinary retention and overflow incontinence. The bladder distends without sensation or contraction.
- Autonomous bladder (complete sacral cord lesion): no voluntary or reflex control; automatic contraction at low volumes.
- Sensory neurogenic bladder (posterior column/sensory root lesion — e.g., tabes dorsalis): large capacity, overflow incontinence, loss of bladder sensation.
SELF-CHECK
A 60-year-old man presents with sudden-onset speech difficulty. On examination, his speech is fluent and voluminous but contains incorrect words ('I want the bork' for 'I want the fork') and made-up words. He cannot follow simple commands, cannot repeat a phrase, and cannot name objects. He appears agitated. He has no limb weakness. Which aphasia type is this, and where is the lesion?
A. Broca's aphasia — posterior inferior frontal gyrus, left hemisphere
B. Wernicke's aphasia — posterior superior temporal gyrus, left hemisphere
C. Global aphasia — large left MCA territory
D. Conduction aphasia — arcuate fasciculus, left parietal lobe
Reveal Answer
Answer: B. Wernicke's aphasia — posterior superior temporal gyrus, left hemisphere
The key features are: fluent output (rules out Broca's), severely impaired comprehension (rules out conduction aphasia which spares comprehension), paraphasias (phonemic and neologisms), and no limb weakness (typical of Wernicke's since the temporal lesion is distant from the motor cortex). This is Wernicke's (receptive/fluent) aphasia from damage to the posterior superior temporal gyrus (Wernicke's area, left hemisphere). Global aphasia also has comprehension impairment but speech is non-fluent and usually associated with hemiplegia. Conduction aphasia has repetition as the most impaired function with relatively preserved comprehension. The patient's agitation is characteristic of Wernicke's aphasia — the patient is producing what they believe is meaningful speech but cannot understand why others look confused.
SELF-CHECK
A 55-year-old hypertensive man has sudden-onset right hemiplegia with facial droop. On examination the following are noted: right arm power 1/5, right leg 2/5, right-sided upper motor neuron facial palsy (forehead spared), right extensor plantar response. He is alert, follows commands correctly, names objects, and speaks fluently without paraphasias. Which of the following is the MOST LIKELY lesion site?
A. Left posterior inferior frontal gyrus (Broca's area)
B. Right internal capsule (posterior limb)
C. Left internal capsule (posterior limb)
D. Left anterior cerebral artery territory (medial frontal/parietal)
Reveal Answer
Answer: C. Left internal capsule (posterior limb)
Right hemiplegia with UMN facial palsy (forehead spared = UMN) localises the lesion to the left hemisphere (contralateral to right-sided weakness). The absence of aphasia despite left hemisphere involvement, combined with dense hemiplegia affecting face, arm, AND leg, points to the internal capsule rather than cortex — all corticospinal fibres are compacted into the posterior limb here. A left cortical lesion large enough to cause this degree of hemiplegia would almost certainly also cause aphasia (damage to Broca's, Wernicke's, or both). The ACA territory primarily affects leg > arm (medial cortex). The right internal capsule would cause left hemiplegia.
Integrated Documentation and Presentation of the Stroke Patient
The ability to document and present the stroke patient examination in a clear, structured, and clinically useful way is the fifth and integrating skill in this module — and arguably the one that is most directly assessed in clinical assessments and internship practice. Poor documentation in stroke is not merely an administrative failing: it can directly harm the patient if a critical piece of history (onset time, anticoagulant use, prior stroke) is missing at the moment when the thrombolysis decision is being made. A clear oral presentation delivered in under three minutes is what enables the senior physician or stroke team to act on your assessment without repeating the entire evaluation. In Indian teaching hospital settings, the ability to present a structured, timed, localisation-anchored case summary is an explicit OSCE and viva competency. The elements of good documentation follow directly from the examination framework you have learned: each examination domain you have assessed maps to a distinct section of the written note and a distinct component of the oral presentation. Learning to document is therefore not a separate task from learning to examine — it is the same task, performed in writing.
Provided image
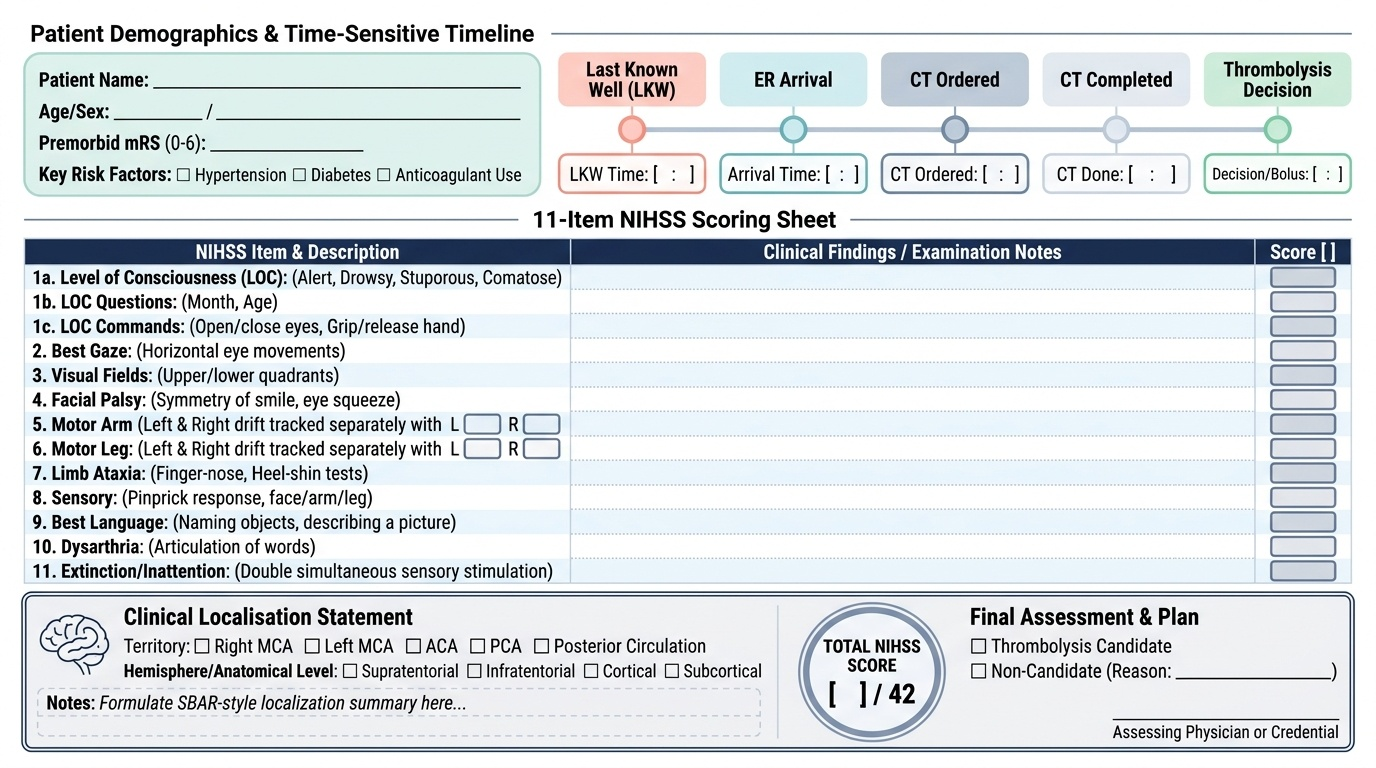
Structured oral presentation format for a stroke patient:
A well-structured acute stroke presentation follows a compressed SBAR-like format in the emergency setting:
- Identification and onset: 'Mr X, a 68-year-old hypertensive and diabetic male, presented at [time] with sudden onset of [deficit] since [last known well time]. Onset was witnessed by his wife at [time].'
- Deficit characterisation: 'He has left hemiplegia [UMN pattern — forehead-spared left facial palsy, left arm power 2/5, left leg 3/5, left extensor plantar], left hemisensory loss to pinprick, and left visual inattention on double simultaneous stimulation. No aphasia. Speech is normally articulated.'
- Localisation statement: 'This clinical picture localises to the right middle cerebral artery territory — right hemisphere, supratentorial, consistent with a right MCA cortical stroke.'
- NIHSS score: 'NIHSS = [X]. [Items contributing to the score].'
- Key risk factors and medications: 'Known hypertension on amlodipine, diabetes on metformin. No anticoagulant use. Premorbid mRS 0.'
- Time to imaging: 'CT brain ordered — last known well 09:15, arrival 09:43, CT at 09:52. Currently within thrombolysis window.'
- Immediate plan: 'BP currently 192/100 mmHg — labetalol given, targeting <185/110 for thrombolysis. Waiting for CT result before proceeding.'
Written documentation should be contemporaneous, timed, and signed. In Indian teaching hospitals the standard format includes: date and time, complaint with duration, presenting symptoms with onset characterisation, past medical and drug history, examination findings (vitals, general, neurological — each cranial nerve, motor, sensory, cerebellar, higher functions), NIHSS score, working diagnosis and differential, immediate investigations ordered, and management plan.
The complete NIHSS examination sequence (for documentation purposes): conscious level (1a, 1b, 1c) → gaze (2) → visual fields (3) → facial palsy (4) → arm motor [right and left] (5a, 5b) → leg motor [right and left] (6a, 6b) → limb ataxia (7) → sensory (8) → language (9) → dysarthria (10) → extinction/inattention (11). Each item scored on a 0–4 scale; total documented as NIHSS = [score]/42.
Self-assessment — clinical application:
Using the examination principles in this module, work through the following case: A 65-year-old right-handed man is brought in acutely. On examination: alert and oriented. Speech is slow, effortful, limited to two or three-word phrases; he understands 'open your eyes' and 'close your fist.' He cannot repeat 'no ifs, ands, or buts.' Right facial droop (forehead spared). Right arm 2/5, right leg 3/5. Right extensor plantar. Sensation intact bilaterally. No visual field deficit. Gait not tested.
Localisation: Non-fluent aphasia (Broca's area, left frontal) + right UMN facial palsy + right arm/leg hemiplegia (arm worse than leg = MCA territory, because ACA territory would give leg > arm) = left MCA cortical territory stroke.
NIHSS estimate: LOC 0, gaze 0, visual fields 0, facial 2, arm motor R 3, leg motor R 2, ataxia 0, sensory 0, language 2 (moderate-severe aphasia), dysarthria 2, extinction 0. Estimated NIHSS ≈ 11 (moderate stroke).
Self-Assessment: Integrating Stroke Clinical Evaluation
Having worked through the full framework of stroke history, neurological examination, lesion localisation, aphasia classification, bladder dysfunction, and integrated documentation, the self-assessment step asks you to apply all these skills together in an integrated clinical encounter. The scenarios below are constructed to mirror what you will encounter in an OSCE station, a neurology ward viva, or the first days of your internship — where you will not be given a pre-labelled problem but will need to generate the diagnosis, localisation, and management plan from the clinical information in front of you. The goal is not to identify the 'right answer' from a list, but to rehearse the cognitive sequence: onset characterisation → examination findings → UMN/LMN decision → side and level → syndrome → likely stroke type → documentation. Work through each scenario before reading the analysis.
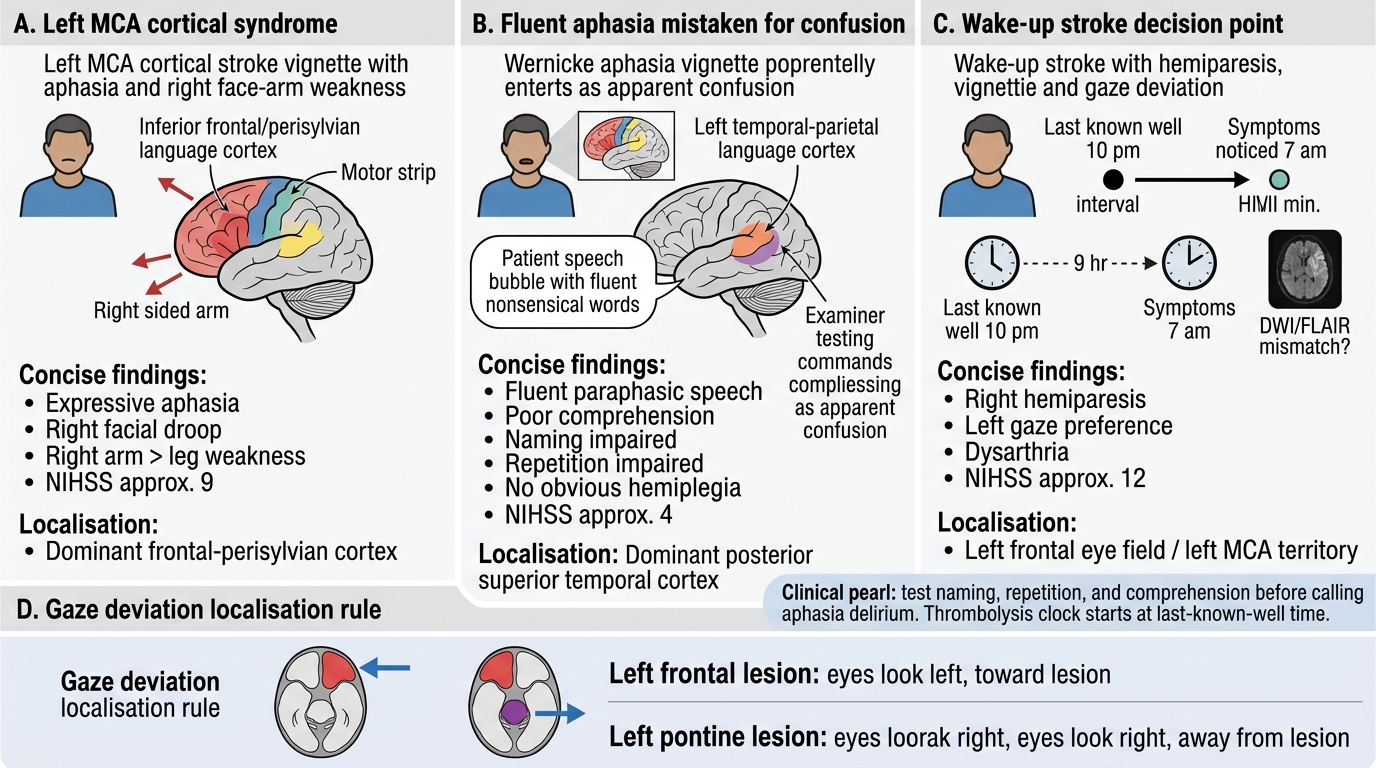
Scenario A: A 74-year-old right-handed woman is brought in by her son at 11:20 am. She was speaking normally when she left for her morning walk at 09:45 am. At 10:55 am she was found sitting on a park bench unable to speak or move her right arm. On examination: BP 178/96 mmHg. Alert, eyes open spontaneously. Gaze deviation to the LEFT. Right facial droop (forehead spared). Right arm 1/5, right leg 2/5. Extensor plantar on right. She cannot follow a single command, cannot name a pen, cannot repeat her name. Speech: mute.
Analysis: Last-known-well 09:45 am → presentation 11:20 am = 1h 35min within thrombolysis window. Left gaze deviation = frontal eye field lesion on the left (eyes deviate toward the damaged hemisphere). Right hemiplegia + right UMN facial palsy = left hemisphere. Mute with no comprehension + no naming = Global aphasia. Lesion = large left MCA territory (both frontal and temporal). NIHSS: LOC 0, gaze 1, visual 0 (not assessed yet), facial 2, arm R 4, leg R 3, ataxia 0, sensory 1 (not testable), language 3, dysarthria 2, extinction 0 — estimated NIHSS ≈ 16 (moderate-severe). Immediate: check blood glucose, NCCT brain, BP management to <185/110, thrombolysis assessment.
Scenario B: A 55-year-old man presents with sudden onset of severe vertigo, vomiting, and inability to walk. He cannot stand without falling to the right. On examination: BP 154/90. Alert, speech slightly slurred (ataxic dysarthria). No facial weakness. Right-sided finger-nose test markedly ataxic. Gait: wide-based, ataxic, falls to right. Power normal in all four limbs. Sensation normal. No visual field defect.
Analysis: Pure ataxia without hemiplegia + ataxic dysarthria + ipsilateral (right) limb and gait ataxia = right cerebellar infarction. No motor or sensory deficit because the cerebellum has no corticospinal fibres. The ataxic dysarthria (scanning speech — irregular, variable volume, slurred) is cerebellar, not bulbar or spastic. TOAST subtype: in a 55-year-old hypertensive, small vessel cerebellar infarction is possible; CT must exclude cerebellar haemorrhage (clinically indistinguishable from infarction — and large cerebellar haemorrhage requires neurosurgical decompression). Note: cerebellar stroke can be life-threatening from posterior fossa oedema causing fourth ventricle compression and obstructive hydrocephalus — NIHSS may appear low but clinical urgency is high.
Scenario C: A 48-year-old woman woke at 6 am with right arm weakness. She was last seen well at 11 pm the previous night. NCCT brain: normal. Is she eligible for IV thrombolysis?
Analysis: Last known well 23:00, symptom noticed 06:00 = 7 hours from LKW. Standard IV thrombolysis window is ≤4.5 hours from LKW — she is OUTSIDE the window. However, wake-up stroke with unknown onset time may be eligible for thrombolysis if MRI shows DWI-positive but FLAIR-negative lesion (indicating the stroke occurred within approximately 4.5 hours before imaging, since FLAIR takes 4.5+ hours to become positive). If DWI/FLAIR mismatch is confirmed, she may be treated per the WAKE-UP trial protocol. If MRI is unavailable, she is NOT a candidate for standard IV thrombolysis but may be a candidate for mechanical thrombectomy if a proximal LVO is identified on CTA.
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
Acute Stroke Examination and Localisation Summary
CLINICAL PEARL
The single most common error in acute stroke examination is confusing aphasia with confusion or delirium. A patient with Wernicke's aphasia produces fluent, paraphasic, neologistic speech and has severely impaired comprehension — on a busy ward, this can be mistaken for acute delirium, especially if there is no obvious hemiplegia (Wernicke's area is distant from the motor cortex). Always assess language formally in any patient with an acute change in 'behaviour' or 'confusion' by testing naming, repetition, and comprehension separately before attributing the change to a non-neurological cause.
A second pearl: the last-known-well time, not the symptom-noticed time, is the thrombolysis clock. A patient who 'woke up with weakness' at 7 am but was last seen well at 10 pm the night before has a 9-hour deficit from last-known-well — outside the IV thrombolysis window. Documenting 'wake-up stroke' triggers immediate MRI DWI/FLAIR mismatch assessment rather than automatic IV thrombolysis.