Page 2 of 24
IM2.1-5 | Atherosclerosis and IHD Foundations — SDL Guide (Part 2)
Acute Coronary Syndromes: Definition, Spectrum, and Natural History
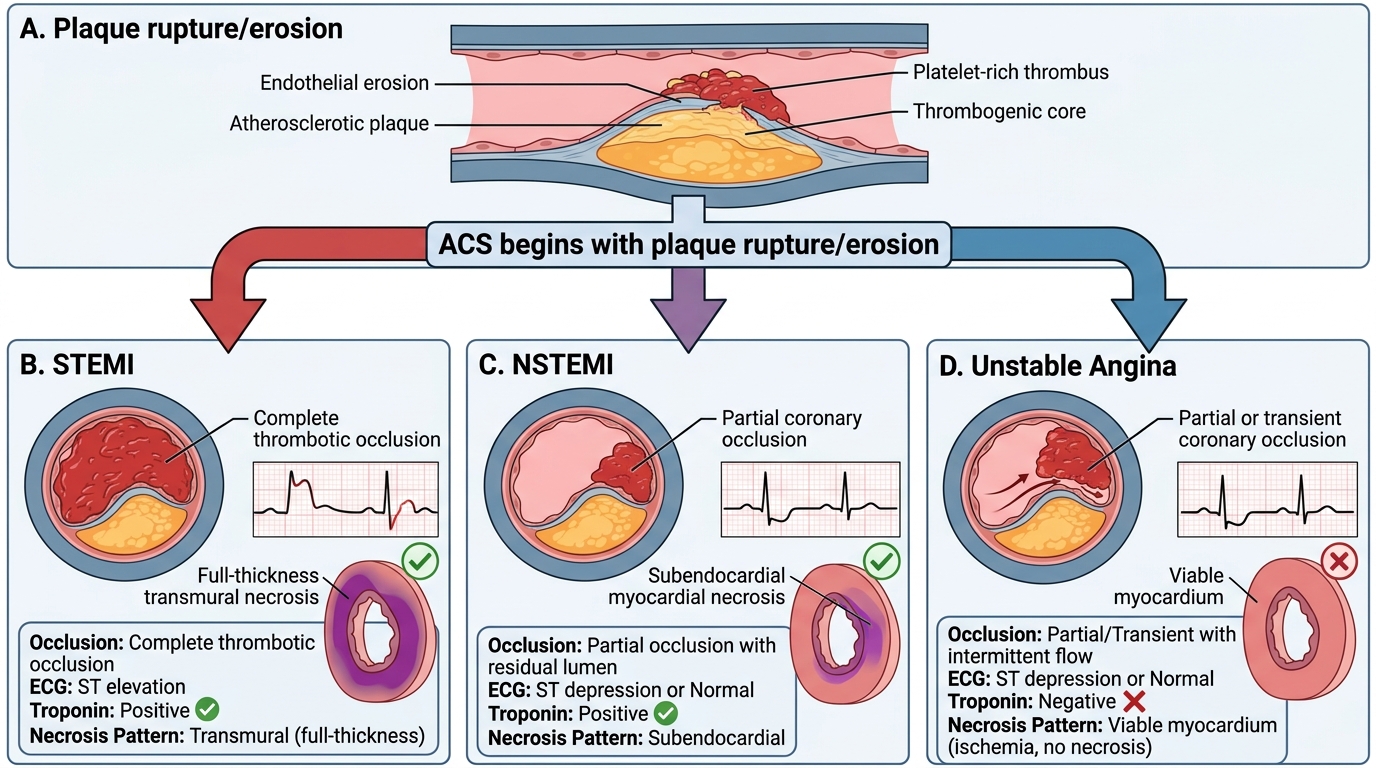
Acute coronary syndromes (ACS) represent the clinical manifestation of acute disruption of coronary blood supply, most commonly due to rupture or erosion of an atherosclerotic plaque with superimposed thrombosis. ACS is not a single diagnosis but a spectrum — distinguished primarily by the ECG pattern and the presence or absence of myocardial necrosis as evidenced by cardiac biomarkers (troponin). Understanding this classification is essential because management differs markedly across the spectrum.
The ACS spectrum comprises three entities:
1. ST-Elevation Myocardial Infarction (STEMI) is caused by a complete (100%) acute occlusion of an epicardial coronary artery by thrombus, producing transmural ischaemia of the territory supplied. The hallmark ECG finding is new ST elevation — ≥2 mm (0.2 mV) in at least two contiguous precordial leads (V1–V6) or ≥1 mm in at least two contiguous limb leads — or new left bundle branch block (LBBB). A posterior STEMI (RCA or LCx occlusion affecting the posterior wall) may show ST depression in V1–V3 (the 'reciprocal' change) and is diagnosed by recording posterior leads (V7–V9) or by ST elevation in a right-sided V4R. The degree and distribution of ST elevation indicates the culprit territory: inferior STEMI (II, III, aVF → RCA); anterior STEMI (V1–V4 → LAD); lateral STEMI (I, aVL, V5–V6 → LCx). Without reperfusion, a STEMI evolves to full-thickness myocardial necrosis within 3–6 hours — this is the emergency that demands the fastest treatment. Troponin rises 3–6 hours after symptom onset, peaks at 12–24 hours, and remains elevated for 7–14 days (reflecting the extent of necrosis).
2. Non-ST-Elevation Myocardial Infarction (NSTEMI) occurs when coronary thrombosis is partially occlusive — reducing but not eliminating coronary flow — or when the occlusion is brief and intermittent. Ischaemia is typically subendocardial rather than transmural (the subendocardium is furthest from the coronary orifice and most vulnerable to ischaemia). ECG findings are variable: ST depression, T-wave inversion, or a non-diagnostic ECG. The defining feature is troponin elevation confirming myocardial necrosis — even a small rise above the 99th percentile upper reference limit of the assay is diagnostic. NSTEMI carries a similar intermediate- to long-term mortality risk to STEMI (because diffuse coronary disease is usually present) but does not require the same emergency reperfusion strategy as STEMI.
3. Unstable Angina (UA) shares the same triggering mechanism (plaque rupture/erosion + thrombosis) as NSTEMI but does not result in permanent myocardial necrosis — the ischaemia is transient (plaque or thrombus resolves spontaneously or with initial therapy) and troponin is NOT elevated (either sensitive or high-sensitivity assay). Clinically, it presents as: rest angina (angina at rest, typically >20 minutes), new-onset angina of at least CCS class III severity, or previously stable angina that has increased in frequency, duration, or occurs at lower levels of exertion (crescendo pattern). Distinguishing UA from NSTEMI requires high-sensitivity troponin assays — the universal availability of these assays has substantially reduced the diagnosis of 'true' UA and reclassified many previously labelled UA cases as NSTEMI.
NSTEMI and UA together are often grouped as NSTE-ACS (non-ST-elevation ACS) for management purposes. The TIMI risk score (7 criteria, 0–7 points) and the GRACE score (Global Registry of Acute Coronary Events — uses age, heart rate, blood pressure, creatinine, Killip class, cardiac arrest at admission, ST deviation, and troponin) stratify NSTE-ACS patients by 30-day mortality/re-MI risk and guide the urgency of invasive strategy (coronary angiography).
Chronic coronary syndrome (stable angina) — previously 'stable CAD' — is not an ACS but represents the chronic symptomatic stage: exercise-induced chest pain from a fixed stenosis that limits coronary flow reserve but has not acutely ruptured. It is defined by the pattern (predictable, exertional, relieved by rest or sublingual nitrate within 5 minutes) and Canadian Cardiovascular Society (CCS) class (I–IV by exertion threshold).
The natural history of untreated ACS is predictable: STEMI without reperfusion carries 30-day mortality of 15–20%; NSTEMI with medical therapy carries ~5% in-hospital mortality; UA carries <1% in-hospital mortality but requires urgent evaluation because 10% will progress to MI within 30 days without treatment. The 1-year mortality post-MI is approximately 10–15%, with most events in the first 30 days. Secondary prevention (antiplatelet therapy, statin, ACE inhibitor/ARB, beta-blocker) and cardiac rehabilitation reduce this risk substantially.
Acute Coronary Syndrome Spectrum
SELF-CHECK
A 60-year-old diabetic man presents with 3 hours of severe chest pain. ECG shows 2.5-mm ST depression in V4–V6 and T-wave inversion in I, aVL. High-sensitivity troponin T at 3 hours is 180 ng/L (99th percentile URL = 14 ng/L). Which ACS category does this represent?
A. STEMI — requires immediate primary PCI
B. NSTEMI — myocardial necrosis confirmed by troponin elevation without ST elevation
C. Unstable angina — ischaemia without necrosis
D. Stable angina with demand ischaemia
Reveal Answer
Answer: B. NSTEMI — myocardial necrosis confirmed by troponin elevation without ST elevation
The ECG shows ST depression (not elevation) and T-wave inversion, with a markedly elevated high-sensitivity troponin (180 ng/L vs. URL of 14 ng/L — more than 10× the upper reference limit). This pattern — ischaemic ECG changes + troponin elevation, without ST elevation — defines NSTEMI. STEMI requires ST elevation (or new LBBB). Unstable angina by definition has no troponin elevation. Stable angina does not cause troponin elevation. NSTEMI management involves antiplatelet loading, anticoagulation, and risk-stratified early invasive strategy (coronary angiography within 24–72 hours based on GRACE score).
Risk Stratification and the Concept of Cardiovascular Risk
Translating the epidemiology and pathophysiology of IHD into clinical action requires a framework for quantifying individual cardiovascular risk — both to identify who needs primary prevention and to determine the intensity of intervention. Risk stratification moves beyond the presence or absence of individual risk factors to estimate the absolute probability of a cardiovascular event over a defined time horizon.
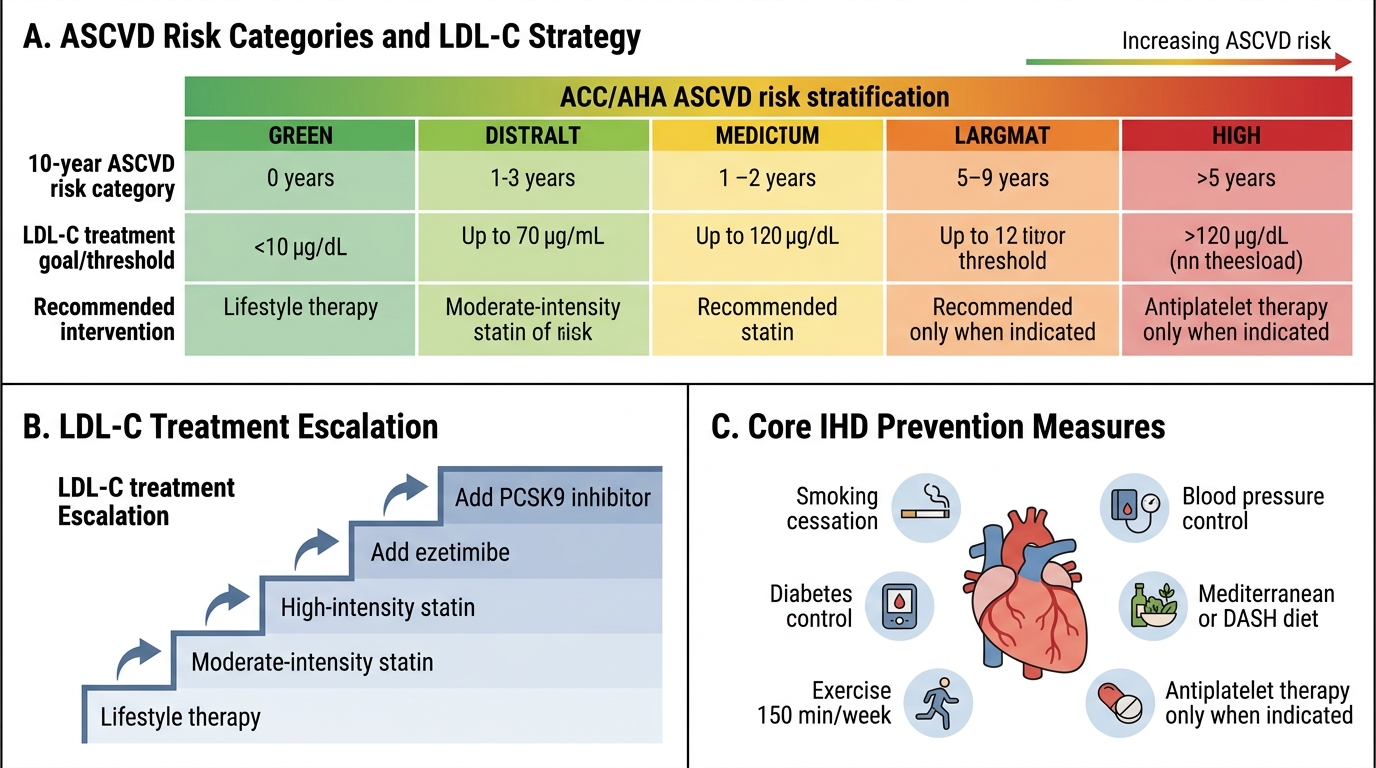
The most widely used tools in India and globally for primary prevention risk stratification include the Framingham Risk Score (FRS) — developed from the Framingham Heart Study cohort — and the ASCVD (Atherosclerotic Cardiovascular Disease) Pooled Cohort Equations (ACC/AHA 2013), which estimate the 10-year risk of a first atherosclerotic event (fatal or non-fatal MI, or fatal stroke). These scores incorporate age, sex, total cholesterol, HDL-cholesterol, systolic blood pressure, smoking status, and diabetic status. Risk is stratified as low (<5%), intermediate (5–10%), high (10–20%), and very high (>20%) for 10-year ASCVD risk. However, the Framingham and Pooled Cohort equations were derived from predominantly White and Black American cohorts and overestimate risk in South Asians in India by 10–30%, so direct application without ethnic correction should be done cautiously.
For secondary prevention (patients who have already had a cardiovascular event — MI, stroke, PAD, or coronary revascularisation), the 10-year risk is by definition very high (often >20–30%) and risk stratification tools are not needed to decide whether to treat — all such patients receive intensive secondary prevention. The focus shifts to optimising each modifiable risk factor to target levels: LDL-C <70 mg/dL (or <55 mg/dL in very high risk — ESC/EAS 2019 guidelines), blood pressure <130/80 mmHg, HbA1c <7% in most diabetics, and complete smoking cessation.
The concept of total cardiovascular risk — rather than treatment of individual risk factors in isolation — is the modern approach. A patient with modestly elevated LDL and moderately elevated blood pressure who is diabetic, middle-aged, and male has a much higher absolute risk than a young non-diabetic woman with the same LDL. Treating the man aggressively with a statin and antihypertensive agent prevents far more events per unit cost than treating the low-risk woman with the same drugs. This is the number needed to treat (NNT) framework: absolute risk reduction (ARR) = baseline risk × relative risk reduction (RRR) of the intervention. High-risk patients have low NNTs (many events prevented per 100 treated), making intervention highly cost-effective.
⚑ AI image — pending faculty review (auto-QA score 4/10; best of 3 attempts)
ASCVD Risk Stratification and LDL-C Management in IHD
Overview of Management Principles in IHD
The management of IHD spans a continuum from primary prevention in asymptomatic high-risk individuals through to emergency reperfusion in acute STEMI and long-term secondary prevention after a coronary event. While the detailed pharmacology and procedural management of ACS are covered in subsequent modules (IM2.14–2.23), understanding the fundamental management framework at the level of IM2.1–2.5 is essential for contextualising the epidemiology and pathophysiology covered in this module.
Primary prevention targets individuals who have not yet had a cardiovascular event but are at elevated risk. The cornerstone interventions are: smoking cessation (the single most cost-effective intervention — cessation reduces CAD risk by 50% within 1 year and to near-baseline by 5 years); statin therapy for elevated LDL-C (reduces major cardiovascular events by 22% per 1 mmol/L LDL reduction — CTT meta-analysis); antihypertensive therapy when blood pressure meets threshold criteria; glycaemic control in diabetes (evidence strongest for reducing microvascular disease but also provides cardiovascular benefit); regular aerobic exercise (150 minutes/week moderate intensity); and Mediterranean or DASH dietary pattern. Low-dose aspirin for primary prevention is no longer routinely recommended in all high-risk individuals after the ASPREE and ARRIVE trials showed no net benefit over bleeding risk in the absence of prior events — it should be individualised based on 10-year ASCVD risk and bleeding risk assessment.
Secondary prevention after a documented coronary event or revascularisation involves the ABCDE framework: A — Antiplatelet + ACE inhibitor/ARB; B — Beta-blocker + Blood pressure control; C — Cholesterol reduction (statin targeting LDL <70 mg/dL or <55 mg/dL in very high risk, with the option of ezetimibe or PCSK9 inhibitor if target not reached) + Cigarette cessation; D — Diet and Diabetes control; E — Exercise and cardiac rehabilitation. Dual antiplatelet therapy (aspirin + P2Y12 inhibitor — ticagrelor or clopidogrel) is continued for at least 12 months after ACS; the duration is extended or shortened based on bleeding vs ischaemic risk assessment (DAPT score, PRECISE-DAPT score).
Emergency reperfusion in STEMI requires either primary percutaneous coronary intervention (PCI) — the preferred strategy if door-to-balloon time can be achieved within 90 minutes of first medical contact — or thrombolysis (fibrinolytic therapy with alteplase, tenecteplase, or streptokinase) when primary PCI is not available within 120 minutes of first medical contact. In India, most centres outside metro areas and tertiary care hospitals do not have 24/7 PCI capability, making pharmacological thrombolysis followed by transfer for angiography ('pharmaco-invasive strategy') the practical approach for a substantial proportion of STEMI patients.
The management of chronic coronary syndrome (stable angina) involves anti-ischaemic therapy (beta-blockers as first-line to reduce heart rate and myocardial oxygen demand; calcium channel blockers or long-acting nitrates as alternatives), risk factor modification, and revascularisation (PCI or CABG) when symptoms are refractory to medical therapy or when anatomy confers a survival benefit (left main or three-vessel disease with reduced LV function).
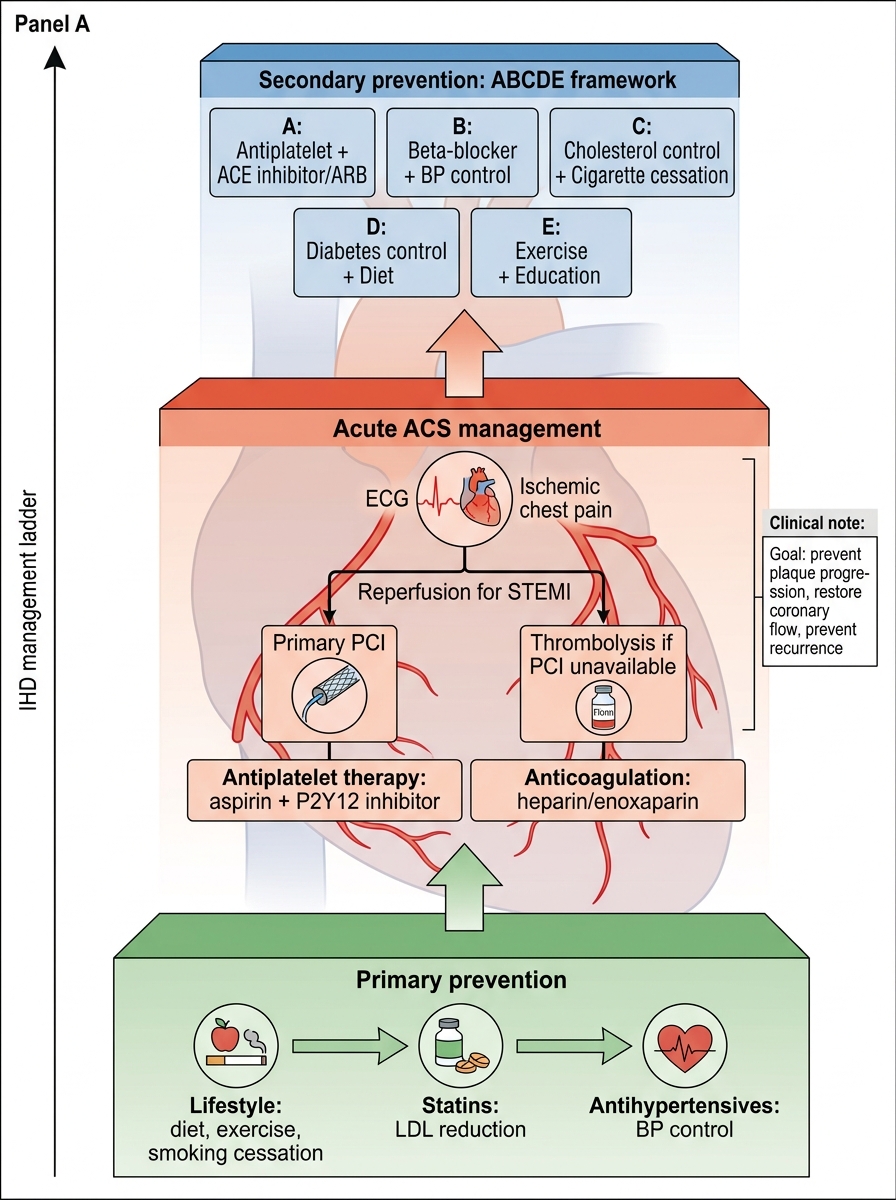
IHD Management Ladder