Page 3 of 24
IM2.1-5 | Atherosclerosis and IHD Foundations — SDL Guide (Part 3)
Self-Assessment: IHD Foundations in Clinical Context
At this stage you have covered the foundational epidemiology, risk factor biology, lipid pathophysiology, plaque pathogenesis, the ACS spectrum, and the overarching management framework. The clinical scenarios below ask you to integrate this knowledge — connecting mechanism to presentation to risk classification — before you encounter these patients in the wards. For each scenario, work through the reasoning steps independently before reading the analysis. The goal is not to test recall of isolated facts but to practise the clinical reasoning chain: from patient characteristics to risk factor identification, from ECG pattern to ACS classification, and from pathological mechanism to appropriate initial management direction. Integrating these steps is the core competency demanded by the NMC IM2 objectives at the KH level — you must be able to reason through a patient encounter, not merely recite definitions.
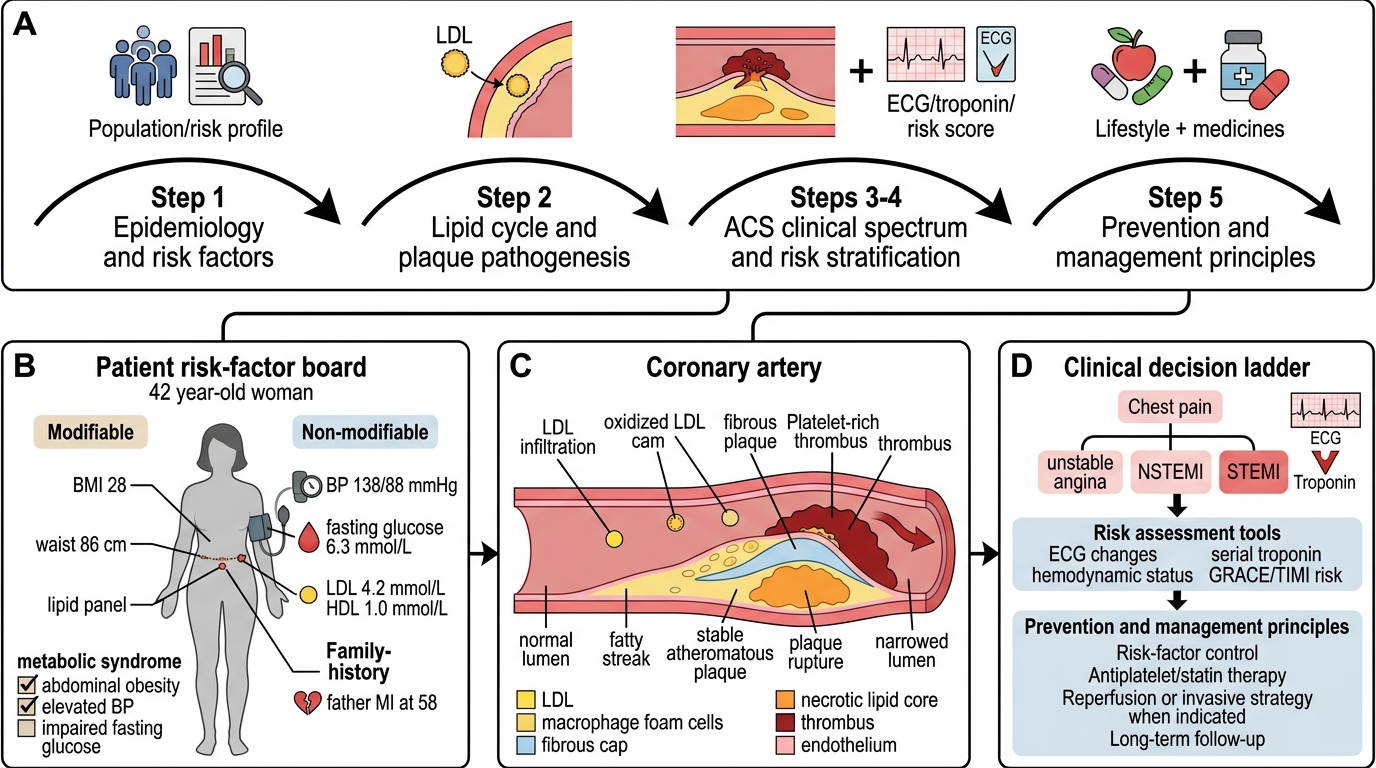
Five-Step Arc of Ischemic Heart Disease
Scenario A: A 42-year-old woman with no cardiac history presents for a routine medical examination. She is a non-smoker, with BMI 28, waist circumference 86 cm, blood pressure 138/88 mmHg (repeated), fasting glucose 6.3 mmol/L, total cholesterol 6.1 mmol/L, HDL 1.0 mmol/L, and LDL 4.2 mmol/L. Her father had an MI at age 58. Identify her modifiable and non-modifiable IHD risk factors and categorise her metabolic status.
Analysis: Non-modifiable: sex (woman, pre-menopausal, so relative protection at this age; however she is approaching the higher-risk window), family history (father MI at 58 = premature if <65 in a female first-degree relative — YES, this qualifies). Modifiable: stage 1 hypertension (138/88 mmHg using ACC/AHA 2017 criteria — threshold ≥130/80), impaired fasting glucose (IFG, 6.3 mmol/L = 113 mg/dL, between normal ≤5.6 mmol/L and diabetic ≥7.0 mmol/L), elevated LDL (4.2 mmol/L = ~162 mg/dL), low HDL (1.0 mmol/L = ~39 mg/dL, borderline), abdominal obesity (waist 86 cm exceeds the 80 cm threshold for Asian women). She has metabolic syndrome (3 of 5 criteria: elevated waist, elevated BP, elevated FBS). Her 10-year ASCVD risk should be formally calculated, but clinically she qualifies as at least intermediate-risk with multiple risk factors.
Scenario B: A 58-year-old man with a history of hypertension and smoking presents with sudden severe central chest pain radiating to the jaw that has lasted 45 minutes. His ECG shows 4-mm ST elevation in leads II, III, and aVF with reciprocal ST depression in I and aVL. Identify the culprit vessel and the ACS category; explain the pathological mechanism.
Analysis: ST elevation in II, III, aVF (inferior leads) with reciprocal changes in I, aVL → inferior STEMI. Culprit vessel is almost always the right coronary artery (RCA) (dominant in 85% of individuals, supplying the inferior wall and posterior LV). ACS category: STEMI — complete occlusive thrombus on a ruptured atherosclerotic plaque in the RCA. Mechanism: decades of atherosclerosis driven by smoking and hypertension → thin-cap fibroatheroma → plaque rupture → platelet aggregation → fibrin thrombus → complete occlusion → transmural ischaemia of inferior wall → ST elevation. Time is muscle: every 30 minutes of additional ischaemia adds 1 year of life lost (Boersma relationship). Reperfusion is needed urgently — primary PCI or thrombolysis if PCI is not available within 120 minutes.
Scenario C: A 50-year-old woman with type 2 diabetes presents with worsening exertional breathlessness and occasional mild left arm heaviness. She denies classic chest pain. Her resting ECG shows non-specific T-wave changes in V4–V6. High-sensitivity troponin at 0 and 3 hours is negative. Exertional stress testing shows ≥2-mm ST depression at moderate exertion. What ACS category (if any) applies, and what additional investigation is most appropriate?
Analysis: No acute troponin elevation → no ACS (STEMI or NSTEMI excluded). Absence of rest symptoms excludes unstable angina. The positive stress test (≥1-mm ST depression at moderate exertion = positive; ≥2-mm = strongly positive) in the context of exertional symptoms suggests significant obstructive CAD causing stable angina. Diabetic patients frequently have 'silent' ischaemia or atypical presentations (breathlessness, arm heaviness without chest pain — neuropathy blunts pain perception). Most appropriate next investigation: coronary CT angiography (CCTA) or direct referral for invasive coronary angiography, depending on clinical probability and local availability. Management: risk factor optimisation, anti-anginal therapy, and if high-grade stenosis confirmed, revascularisation discussion.
SELF-CHECK
Macrophages in an atherosclerotic plaque engulf oxidised LDL (oxLDL) via scavenger receptors rather than via the classic LDL receptor (LDLR). Which statement BEST explains why this leads to foam cell accumulation rather than a regulated cholesterol response?
A. Scavenger receptors are present only on macrophages, restricting uptake to the plaque
B. Unlike LDLR, scavenger receptors are not downregulated by rising intracellular cholesterol, so uptake continues unchecked
C. OxLDL has a higher affinity for LDLR than native LDL, causing receptor saturation
D. Macrophages in the plaque lack the intracellular machinery for cholesterol esterification
Reveal Answer
Answer: B. Unlike LDLR, scavenger receptors are not downregulated by rising intracellular cholesterol, so uptake continues unchecked
The LDLR is subject to feedback inhibition: as intracellular cholesterol rises, LDLR expression is downregulated (via SREBP pathway), capping further LDL uptake. Scavenger receptors (SR-A, CD36) operate outside this feedback loop — they are not downregulated by cholesterol accumulation. Therefore, macrophages continue ingesting oxLDL until they are engorged with cholesterol ester droplets, becoming foam cells. This unchecked uptake is central to atheroma formation. Note that macrophages do esterify cholesterol (ACAT enzyme) — the problem is not the esterification step but the unregulated receptor.
CLINICAL PEARL
The concept of plaque vulnerability overturns the intuitive assumption that 'bigger means more dangerous' in coronary artery disease. In practice, more than 60% of acute MIs arise from plaques that caused less than 50% luminal stenosis at their last angiogram. These lipid-rich, thin-capped plaques are invisible as haemodynamically significant lesions on stress testing — they do not cause exertional ischaemia. It is the quality of the plaque (cap thickness, lipid core size, macrophage burden) rather than the quantity of stenosis that determines acute rupture risk. This is precisely why statins prevent MI not by opening blocked arteries but by stabilising vulnerable plaques — reducing the lipid core, decreasing macrophage infiltration, increasing fibrous cap thickness, and exerting anti-inflammatory effects at the plaque level.
Second pearl: In the Indian context, remember that IHD strikes approximately a decade earlier than in Western populations and that diabetic patients frequently have silent ischaemia — they may present with breathlessness, arm heaviness, jaw pain, or epigastric discomfort rather than the 'textbook' crushing central chest pain. A low threshold for ECG and troponin in these presentations saves lives.