Page 1 of 13
IM20.1-2 | Seizure Disorder Foundations and Diagnosis — SDL Guide
Learning Objectives
- Define seizure, convulsion, and epilepsy with precision using the ILAE 2014 operational definition
- Classify seizure types using the ILAE 2017 framework (focal, generalised, unknown onset) with clinical examples
- Enumerate and describe the six aetiological categories of epilepsy with emphasis on the Indian context (neurocysticercosis, cerebral malaria)
- Explain the pathophysiology of seizure generation including the paroxysmal depolarisation shift and the excitation-inhibition imbalance
- Describe a systematic clinical evaluation including history, examination, and the differential diagnosis of seizure mimics
- Outline the diagnostic investigations in epilepsy: blood tests, EEG pattern recognition, MRI protocol, and CSF indications
INSTRUCTIONS
This module builds the diagnostic foundation for seizure disorders in general medicine. You will learn to distinguish seizures, convulsions, and epilepsy with precision; classify seizure types using the current ILAE framework; identify the six aetiological categories with special attention to the Indian context; understand the pathophysiology underpinning treatment choices; evaluate a patient after a first seizure; and interpret EEG patterns and neuroimaging findings. These competencies underpin the management decisions covered in the companion module.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 418 — Seizures and Epilepsy (textbook)
- API Textbook of Medicine, 10th ed. — Neurology: Epilepsy and Seizure Disorders (textbook)
- Davidson's Principles and Practice of Medicine, 23rd ed., Ch. 28 — Neurological Disease: Epilepsy (textbook)
- ILAE Classification of Seizures, 2017 (Fisher et al., Epilepsia) (guideline)
- ILAE Operational Classification of Seizure Types, 2017 (Fisher et al., Epilepsia 58:522–530) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 24-year-old engineering student collapses in the college canteen. Witnesses describe rhythmic jerking of all four limbs lasting about two minutes, eye deviation to the right, clenched jaw, and complete unresponsiveness during the episode. By the time the ambulance arrives, he is drowsy but rousable. This is the first episode anyone has ever seen. In the emergency department, his vital signs are now normal, neurological examination is unremarkable, and blood glucose is 92 mg/dL. His mother tells you that he had a 'funny turn' three months ago — he stared blankly for about 20 seconds, made chewing movements, and afterwards could not recall what he had been saying. A different clinician dismissed that episode as a vasovagal faint. Now consider: were these two episodes the same phenomenon? What is the correct label — seizure, convulsion, or epilepsy — for what happened today and for what happened three months ago? And critically: does a single convulsion in a 24-year-old mandate immediate antiepileptic drug therapy, or does the decision rest on something more? This module builds the diagnostic framework that turns these questions from uncertainty into clinical clarity.
WHY THIS MATTERS
Seizure disorders represent one of the most common neurological presentations in general medicine, affecting approximately 1–2% of the world population. In India, the estimated prevalence of epilepsy is 5–10 per 1000, with a disproportionate burden in rural areas where birth asphyxia, neurocysticercosis, and febrile convulsions are prominent contributors. Every general physician — not just a neurologist — will encounter a post-ictal patient in casualty, be asked to counsel a family after a first seizure, or advise a patient with known epilepsy about medication adherence, driving, and pregnancy. The NMC competencies IM20.1 and IM20.2 require you to define and differentiate seizures, convulsions, and epilepsy (IM20.1, Knowledge level) and to discuss aetiological classification, pathophysiology, clinical evaluation, and diagnostic workup (IM20.2, Knowledge with application). Mastering this diagnostic framework is prerequisite to the management decisions in the companion module.
RECALL
Activate your prior knowledge of neuroanatomy and neurophysiology before proceeding. A neuron generates an action potential when its membrane depolarises beyond threshold, driven by rapid influx of Na⁺ through voltage-gated sodium channels. The resting membrane potential (approximately −70 mV) is maintained by the Na⁺/K⁺-ATPase pump and the relative impermeability of the resting membrane. GABAergic inhibitory interneurons maintain a tonic brake on cortical excitability; when this inhibition is impaired — by hypoxia, hypoglycaemia, drug withdrawal, or genetic channel dysfunction — widespread synchronous neuronal discharge can occur. Glutamate, the principal excitatory neurotransmitter acting through AMPA and NMDA receptors, drives excitation; GABA (gamma-aminobutyric acid) acting through GABA-A and GABA-B receptors drives inhibition. Also recall the concept of the blood-brain barrier (BBB), which normally excludes many large molecules and pathogens from the CNS but is disrupted in acute meningitis and encephalitis — an important background for understanding symptomatic seizures. Finally, recall that the EEG (electroencephalogram) records the summated postsynaptic potentials of pyramidal neurons in the cortex — the substrate that is abnormally synchronised during a seizure.
Defining Seizures, Convulsions, and Epilepsy
The terms seizure, convulsion, and epilepsy are frequently used interchangeably in lay and even clinical discourse, but they carry distinct meanings that have direct implications for diagnosis, investigation, and management. Precision in terminology is not pedantic — it prevents treatment errors and shapes the conversation with patients and families.
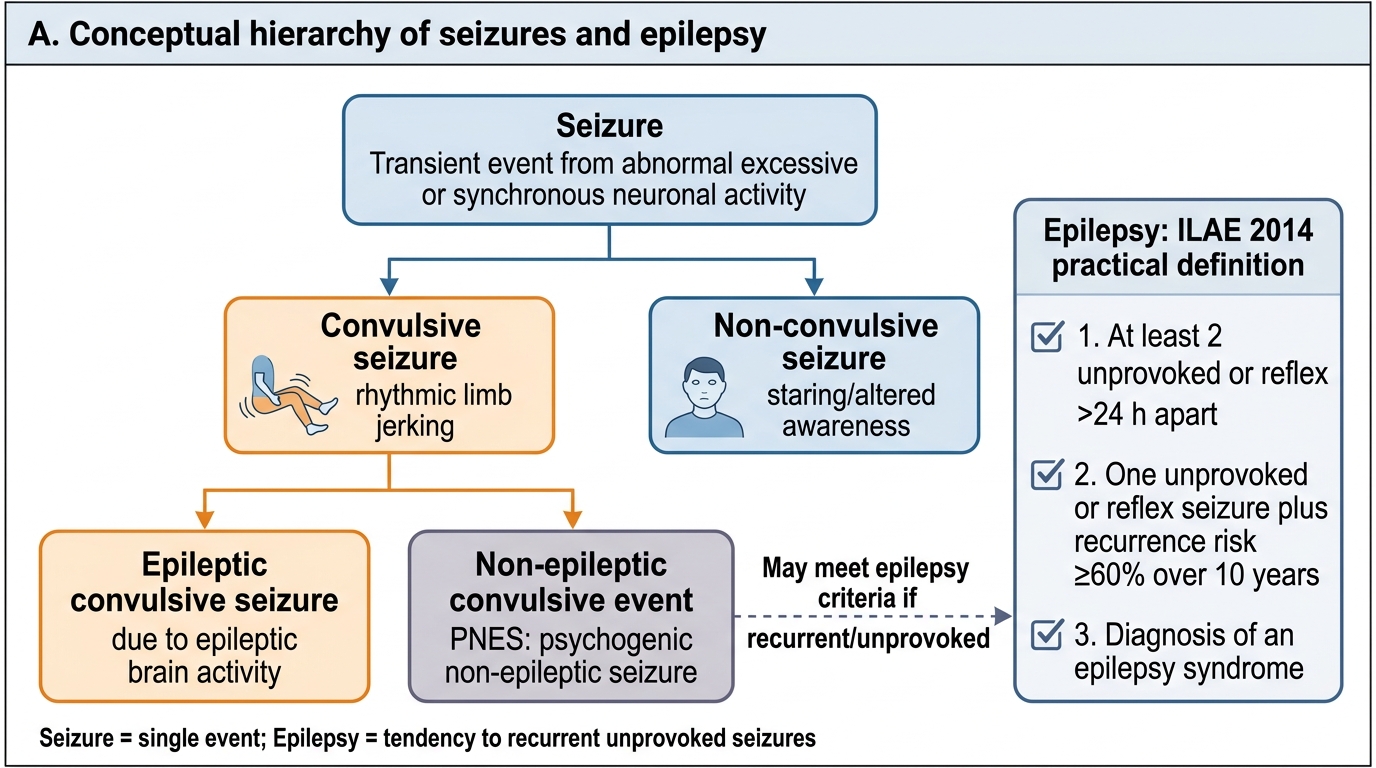
A seizure (also termed an ictus) is defined as a transient occurrence of signs or symptoms due to abnormal, excessive, or synchronous neuronal activity in the brain. This is the broadest and most fundamental category. The neurophysiological substrate is a paroxysmal discharge — a sudden, self-limited burst of abnormal electrical activity — arising from a population of neurons that fire simultaneously rather than in the normal asynchronous pattern. Seizures may be convulsive (accompanied by motor manifestations) or non-convulsive (absence of prominent motor activity, as in absence seizures or focal impaired awareness seizures). A seizure may also be provoked — occurring as a direct, time-limited response to a known and reversible cause — or unprovoked, in which no such precipitant is identified.
A convulsion is a subtype of seizure characterised specifically by involuntary, rhythmic muscle contractions — the stereotyped tonic-clonic movements that most people envision when they hear the word 'seizure'. It is a motor symptom, not a disease entity. Not all seizures involve convulsions (absence seizures have no convulsive component), and not all convulsions are epileptic (psychogenic non-epileptic seizures — PNES — can produce convulsive movements without any ictal EEG discharge). The clinical and medicolegal importance of distinguishing epileptic convulsions from non-epileptic events cannot be overstated.
Epilepsy is a disease of the brain defined by any of the following three conditions under the International League Against Epilepsy (ILAE) 2014 operational definition: (1) at least two unprovoked (or reflex) seizures occurring more than 24 hours apart; (2) one unprovoked seizure and a probability of further seizures similar to the general recurrence risk after two unprovoked seizures (i.e., ≥60%) over the next 10 years — which applies when there is an identified underlying epileptogenic lesion (e.g., MRI scar, specific epilepsy syndrome, or a brain structural abnormality); or (3) diagnosis of an epilepsy syndrome. The reason for defining epilepsy as a disease rather than simply a symptom is that it implies a lasting predisposition to generate seizures — the two-unprovoked-seizures-more-than-24-hours-apart criterion reflects statistical evidence that the recurrence risk after a second unprovoked seizure is approximately 70–80%. Epilepsy is considered to be resolved if a patient has had an age-dependent epilepsy syndrome (such as childhood absence epilepsy) that is now past the applicable age, or if the patient has remained seizure-free for 10 years and off antiepileptic drugs (AEDs) for the last 5 of those years.
The clinical significance of these distinctions: a provoked seizure (e.g., during acute hypoglycaemia, alcohol withdrawal, acute meningitis, or eclampsia) does not define epilepsy because the brain is reacting to a temporary, reversible insult. Treatment of the precipitant — not long-term AED therapy — is the correct response. Only when seizures are unprovoked does the risk of recurrence justify the diagnosis and treatment decision of epilepsy.
Seizure, Convulsive Events, PNES, and Epilepsy Criteria
ILAE Classification of Seizures and Epilepsy
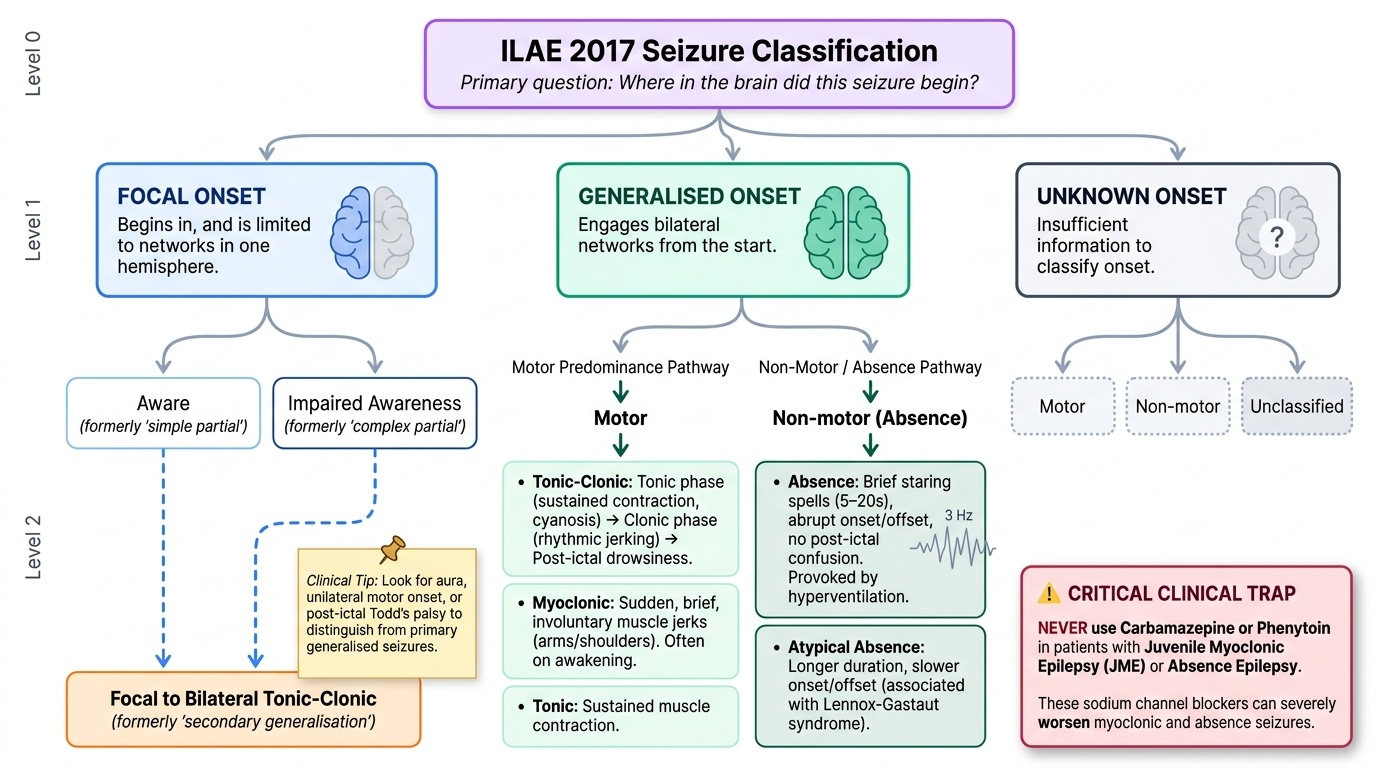
The most widely used framework for classifying seizures is the ILAE 2017 Classification of Seizure Types, which supersedes the older 1981 classification. Understanding the new classification is essential for selecting appropriate antiepileptic drugs, since many AEDs are seizure-type specific, and certain drugs worsen specific seizure types. The classification proceeds from the seizure onset zone — the first question is always: where in the brain did this seizure begin?
Provided image
The primary division is between focal onset seizures (previously termed partial seizures) — those beginning in, and rapidly engaging, networks limited to one hemisphere — and generalised onset seizures — those engaging bilateral networks from the start. A third category is unknown onset when information is insufficient to classify the onset. For focal onset seizures, a secondary descriptor notes whether awareness was retained (formerly simple partial) or impaired (formerly complex partial). Focal seizures may evolve into a focal to bilateral tonic-clonic seizure (formerly called secondary generalisation), a point of critical importance because clinically, a witnessed bilateral tonic-clonic event may in fact be a secondarily generalised focal seizure — recognising the focal onset (aura, unilateral motor onset, post-ictal Todd's palsy) changes both the aetiological workup and the AED choice.
Generalised onset seizures are further classified by their motor or non-motor predominance:
- Tonic-clonic seizures (grand mal): the classic bilateral convulsion — tonic phase (sustained muscle contraction, cyanosis, apnoea) followed by clonic phase (rhythmic jerking), then post-ictal drowsiness.
- Absence seizures (petit mal): brief (typically 5–20 seconds), staring spells with impaired awareness and abrupt onset/offset; no post-ictal confusion; hyperventilation provokes them; 3 Hz spike-and-wave on EEG. There are also atypical absence seizures (longer duration, less abrupt onset/offset) in Lennox-Gastaut syndrome.
- Myoclonic seizures: sudden, brief, involuntary muscle jerks, typically of the arms and shoulders; characteristically occur on awakening (morning myoclonus in juvenile myoclonic epilepsy — JME). Key trap: myoclonic seizures are worsened by carbamazepine and phenytoin — NEVER use these in JME or absence epilepsy.
- Tonic seizures: sustained muscle stiffening without a clonic phase.
- Atonic seizures (drop attacks): sudden loss of muscle tone causing the patient to fall to the ground.
- Clonic seizures: rhythmic jerking without a preceding tonic phase.
For the classification of epilepsy (not just seizure type), the ILAE 2017 framework has four levels: (1) seizure type, (2) epilepsy type (focal, generalised, combined focal+generalised, or unknown), (3) epilepsy syndrome (a specific electroclinical constellation, e.g., childhood absence epilepsy, JME, Dravet syndrome), and (4) aetiology.
Aetiological Classification of Epilepsy
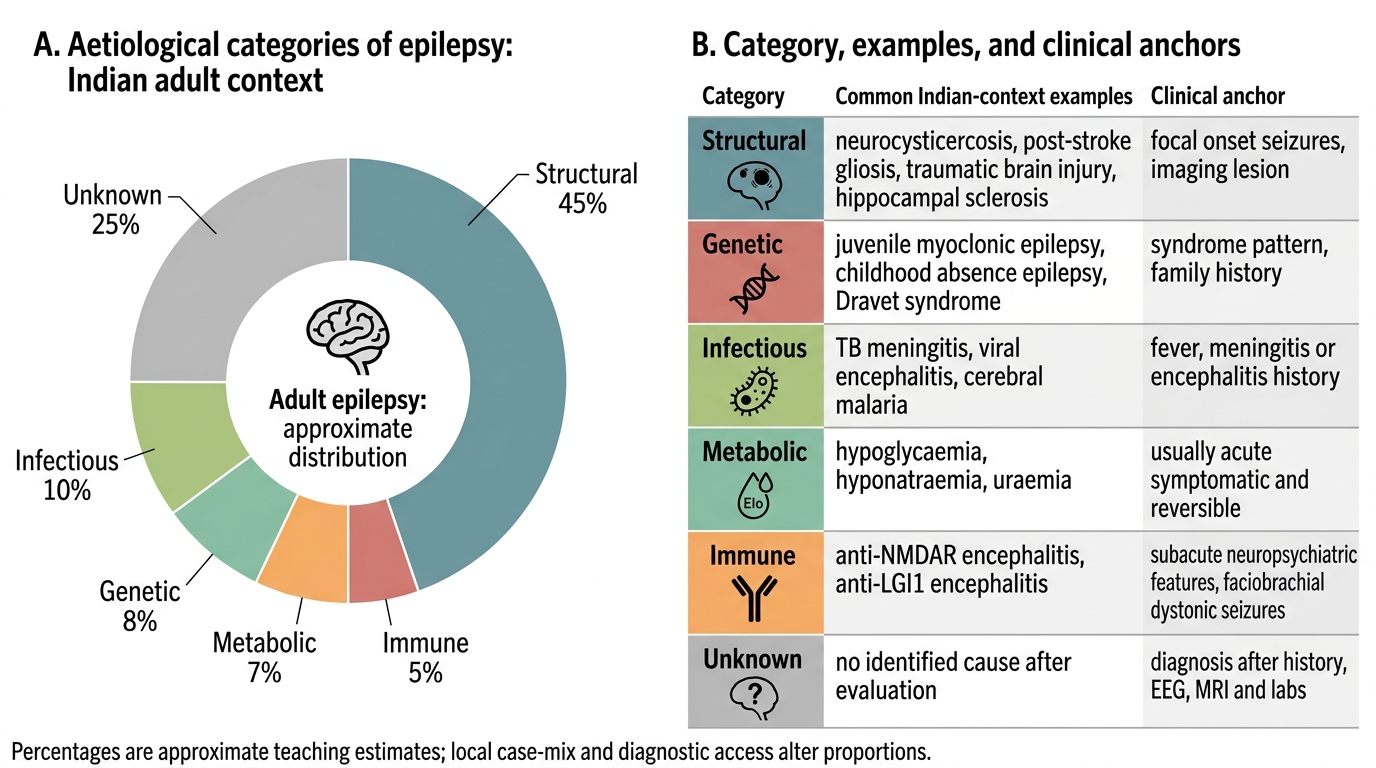
Understanding why a patient has epilepsy — the underlying aetiology — is as important as classifying the seizure type, because it determines prognosis, guides investigation, and may identify a treatable cause. The ILAE 2017 aetiological classification recognises six categories, and a given patient may have more than one relevant aetiology simultaneously. This multi-axial approach reflects the reality that genetic and structural causes, for example, frequently co-exist.
The six ILAE aetiology categories are:
1. Structural: An identified structural abnormality of the brain that is associated with a substantially increased risk of epilepsy. Structural causes include both acquired lesions (post-stroke epilepsy — the commonest cause of new-onset epilepsy over age 60; traumatic brain injury; post-infectious — tuberculous meningitis or bacterial meningitis with cortical scarring; tumours — primary glioma or metastasis; cavernous malformations; hippocampal sclerosis from prolonged febrile seizures) and congenital malformations (focal cortical dysplasia, cortical tubers in tuberous sclerosis, heterotopia). In India, neurocysticercosis — infection by the larval stage of Taenia solium (the pork tapeworm) — is the single most common identified structural cause of new-onset epilepsy in adults, accounting for up to 50% of adult-onset epilepsy cases in some studies from rural areas. The CT or MRI appearance (calcified granuloma, ring-enhancing lesion in an appropriate clinical context) is pathognomonic when combined with serology.
2. Genetic: Epilepsy resulting directly from a known or presumed genetic defect in which seizures are a core symptom. This includes both single-gene defects (e.g., SCN1A mutation in Dravet syndrome, KCNQ2/3 in benign neonatal epilepsy, CDKL5 in early myoclonic encephalopathy) and polygenic contributions to common epilepsy syndromes like JME and childhood absence epilepsy. The term 'genetic' does not preclude treatment; rather, it guides the choice of AED and genetic counselling.
3. Infectious: Both acute CNS infections (bacterial meningitis, viral encephalitis — HSV, Japanese encephalitis — TB meningitis) can cause acute symptomatic seizures (provoked, not epilepsy), while the brain damage resulting from healed infections creates structural epilepsy. Cerebral malaria is an important cause in India — Plasmodium falciparum causes seizures through cerebral oedema, microvascular occlusion, and metabolic dysfunction.
4. Metabolic: A metabolic or biochemical abnormality directly causing seizures. Acute metabolic causes of provoked seizures include: hypoglycaemia (most important — always check glucose first), hyponatraemia (Na⁺ <125 mEq/L), hypocalcaemia, hypomagnesaemia, uraemia (end-stage renal disease), hepatic encephalopathy, non-ketotic hyperglycaemia (can cause focal motor seizures), pyridoxine deficiency (neonates), and porphyria. Chronic metabolic aetiologies include pyridoxine-dependent epilepsy and glucose transporter deficiency (GLUT1).
5. Immune: Epilepsy resulting from a CNS autoimmune disorder. The most important is autoimmune encephalitis due to antibodies against neuronal surface antigens — anti-NMDAR encephalitis (typically young women; psychiatric prodrome, seizures, movement disorder, autonomic dysfunction), anti-LGI1 encephalitis (faciobrachial dystonic seizures pathognomonic), anti-CASPR2, anti-GABA-B. Rasmussen encephalitis is a progressive inflammatory condition causing refractory focal epilepsy. Paraneoplastic encephalitides (anti-Hu, anti-Ma2) are associated with occult malignancy.
6. Unknown: The aetiology cannot be determined despite adequate investigation. This does not mean the epilepsy is benign — it means current investigations are insufficient to identify the cause.
Aetiological Categories of Epilepsy in Indian Adults