Page 10 of 20
IM21.8 | Scorpion Envenomation — SDL Guide
Learning Objectives
- Describe the clinical presentation and grading of scorpion envenomation from Mesobuthus tamulus, distinguishing Grade I, II, and III
- Explain the pathophysiology of the autonomic storm and the transition from hypertension to cardiovascular failure
- Describe the mechanism of action, dose, and route of prazosin in scorpion envenomation
- Explain why beta-blockers are specifically contraindicated in scorpion envenomation
- Outline the complete management protocol for Grade II and Grade III scorpion envenomation including supportive care and ICU indications
INSTRUCTIONS
Scorpion envenomation is a time-critical emergency in which the specific pharmacological treatment (prazosin) dramatically improves survival when given early, and where the wrong treatment (beta-blockers, watchful waiting) causes preventable death. This module equips you with the clinical grading framework, the pathophysiological reasoning, and the precise management protocol needed to act correctly from the first moment.
References
- Harrison's Principles of Internal Medicine, 21st ed. — Scorpion Envenomation (textbook)
- API Textbook of Medicine, 10th ed. — Chapter on Envenomation (textbook)
- Bawaskar HS, Bawaskar PH. Prazosin in management of cardiovascular manifestations of scorpion sting. Lancet. 1986;1(8479):510–511. (journal)
- WHO Guidelines for the Management of Scorpion Envenomation, 2010 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 12-year-old boy is brought to the emergency department of a district hospital in Maharashtra at 2 AM. He woke from sleep screaming with severe pain in his left hand and within an hour developed profuse sweating, vomiting, and agitation. On examination he is distressed, his pulse is 140/min and irregular, BP is 170/110 mmHg, and he has cold, clammy extremities with perioral pallor. There is no visible wound but his mother found a scorpion in his bed. The treating junior doctor has heard that scorpion stings cause only local pain and gives him paracetamol and a sedative. The child deteriorates over the next two hours — his BP drops to 70/40 mmHg, he develops pulmonary oedema, and is transferred critically ill. What was missed, what should have been given instead, and why does prazosin — an alpha-blocker used for hypertension — have a specific role in this condition?
WHY THIS MATTERS
Scorpion envenomation is one of the most underestimated medical emergencies in India. An estimated 100,000–130,000 scorpion stings occur annually in India, with the highest burden in Maharashtra, Andhra Pradesh, Telangana, Tamil Nadu, Rajasthan, and Gujarat. In endemic areas, scorpion sting is the most common cause of toxin-related paediatric intensive care admission. The medically important species in India is Mesobuthus tamulus (the Indian red scorpion), which produces a venom with potent autonomic toxicity that can cause hypertensive crises, acute left ventricular failure, pulmonary oedema, and shock. Children are disproportionately affected due to their smaller body mass per unit venom dose. NMC competency IM21.8 requires the ability to describe the diagnosis, initial approach, stabilisation, and therapy — including the specific role of prazosin, which is the pharmacological cornerstone of management and a frequently examined topic.
RECALL
Activate prior knowledge of the autonomic nervous system. The sympathetic nervous system releases noradrenaline at alpha-1 and beta-1 adrenoceptors: alpha-1 stimulation causes vasoconstriction (raises blood pressure), while beta-1 stimulation causes tachycardia and increased cardiac contractility. Recall also that the parasympathetic nervous system releases acetylcholine at muscarinic receptors, causing bradycardia, increased secretions, and bronchoconstriction. Recall from pharmacology that prazosin is a selective alpha-1 adrenoceptor antagonist used in hypertension; it blocks the vasoconstrictor effect of noradrenaline at peripheral arteries, reducing afterload and blood pressure. Recall from cardiology that pulmonary oedema results when left ventricular failure causes backward rise in pulmonary venous pressure, forcing fluid into the alveoli — clinically manifesting as breathlessness, pink frothy sputum, and crepitations at the lung bases.
Clinical Presentation of Scorpion Envenomation
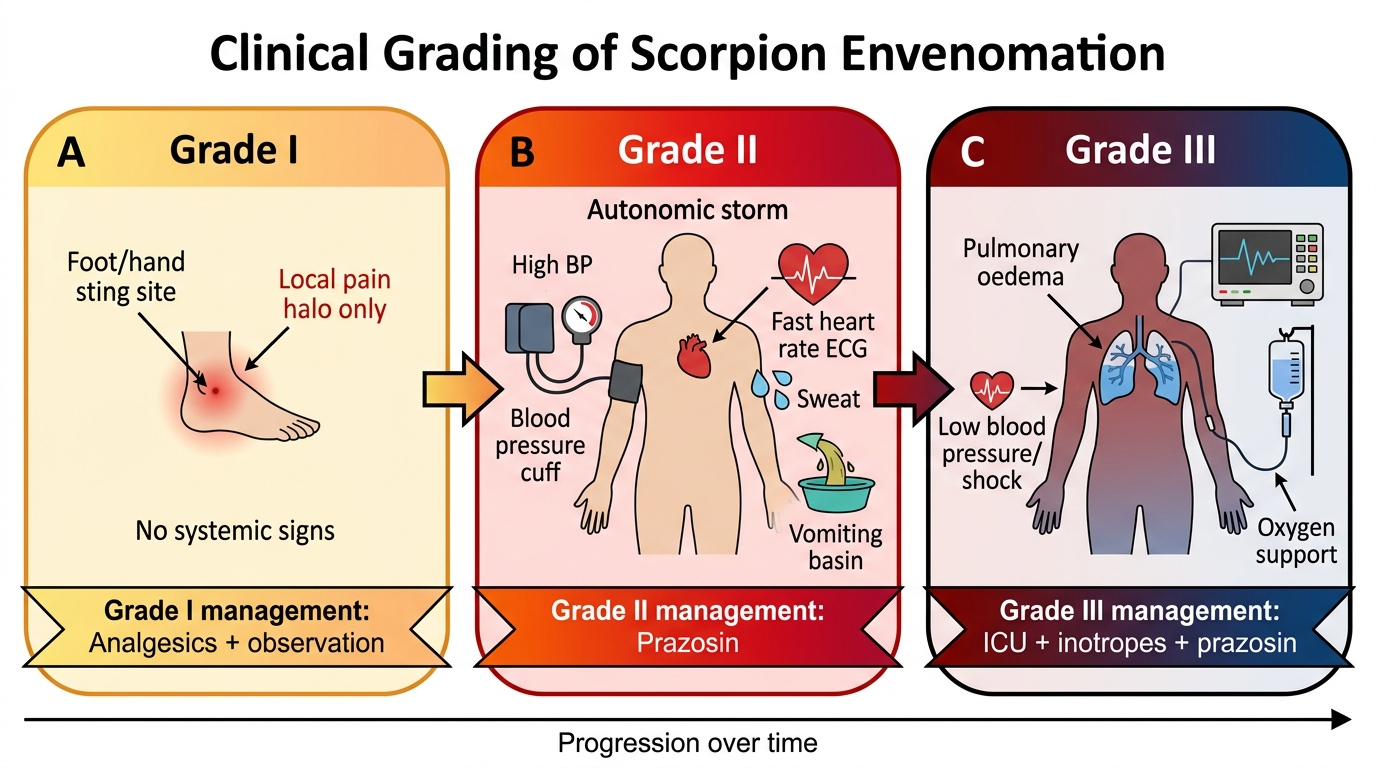
The clinical presentation of scorpion envenomation in India is dominated by autonomic toxicity rather than the neuromuscular paralysis seen with some scorpion species elsewhere in the world. The clinical spectrum ranges from mild local pain (Grade I, the majority of stings) to life-threatening cardiovascular collapse (Grade III, seen in medically significant envenomation from Mesobuthus tamulus).
Grade I (Local envenomation only): The sting causes immediate, severe, burning pain at the site — often described as 'fire in the skin'. There may be local paresthesia, oedema, and erythema. Sweating at the sting site. No systemic features. This is the presentation of most scorpion stings by non-medically-significant species and some stings by medically significant species where venom dose is low. Management is symptomatic (analgesics, local ice). Observe for 4–6 hours for development of systemic features.
Grade II (Systemic — autonomic storm): Reflects systemic venom absorption with activation of the autonomic nervous system. Mesobuthus tamulus venom triggers a massive release of catecholamines (noradrenaline, adrenaline) from adrenal medulla and sympathetic nerve terminals — this is the 'autonomic storm'. Simultaneously, parasympathetic activation occurs. The result is a clinical picture of mixed sympathetic and parasympathetic stimulation:
Sympathetc features: hypertension (often severe, systolic >180 mmHg), tachycardia, cold and clammy extremities (peripheral vasoconstriction), pallor, mydriasis, and agitation.
Parasympathetic features: profuse sweating, excessive salivation, lacrimation, vomiting, bradycardia or heart block (when parasympathetic dominates), and increased bronchial secretions.
In children, the mixed autonomic picture is often dominated initially by sympathetic effects — hypertension and tachycardia — which then transitions to cardiovascular failure. The initial hypertension may be dangerously misinterpreted as 'not requiring treatment' by clinicians unfamiliar with the natural history.
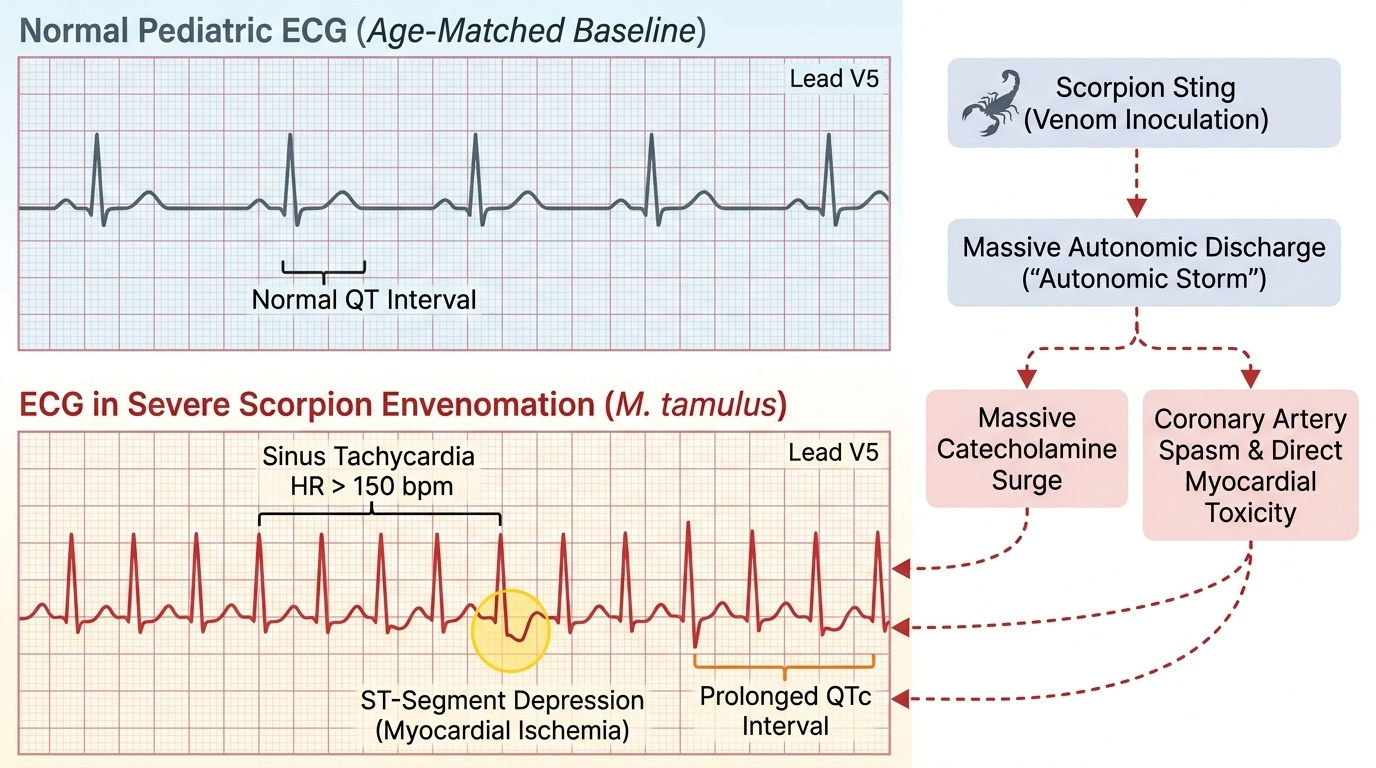
Grade III (Cardiovascular failure): The autonomic storm and excess catecholamine release cause acute myocardial dysfunction (catecholamine-induced cardiomyopathy or 'stunned myocardium'), leading to acute left ventricular failure, pulmonary oedema, and cardiogenic shock. This is the grade that kills. Features include: breathlessness and respiratory distress, pink frothy sputum (pulmonary oedema), basal crepitations, cold shock (peripheral vasoconstriction with falling cardiac output), and severe hypotension. ECG changes include tachyarrhythmias, ST changes, QTc prolongation, and occasionally life-threatening ventricular arrhythmias.
Clinical Grading of Scorpion Envenomation
Pathophysiology of Autonomic Toxicity
The unique pathophysiology of Mesobuthus tamulus (Indian red scorpion) envenomation distinguishes it sharply from snakebite and forms the basis of the targeted treatment with prazosin. Understanding this mechanism explains why prazosin — counterintuitive as it might seem to give an antihypertensive to a child already in shock — is the correct treatment.
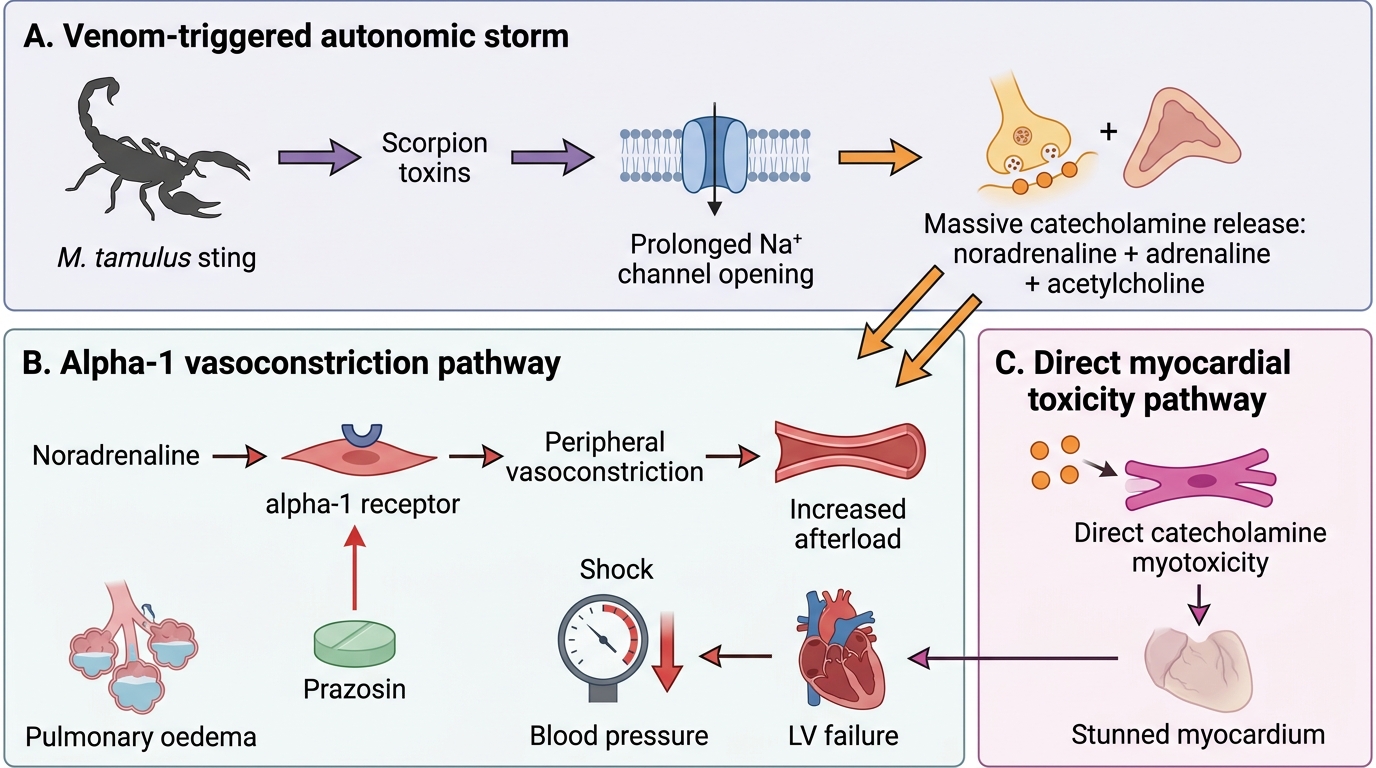
Venom composition and mechanism: The venom of M. tamulus contains scorpion toxins (a family of small peptide neurotoxins) that act by binding to voltage-gated sodium channels in autonomic nerve terminals and the adrenal medulla. Rather than blocking the channels (which would cause paralysis), these toxins prolong the open state of the sodium channel — causing repetitive firing of autonomic neurons. The result is a massive, sustained release of catecholamines (predominantly noradrenaline from sympathetic terminals and adrenaline from the adrenal medulla) into the circulation. Acetylcholine is also released from parasympathetic terminals through the same mechanism.
The catecholamine flood produces the autonomic storm described clinically as Grade II. Circulating noradrenaline activates alpha-1 receptors in peripheral vasculature → intense vasoconstriction → hypertension and increased cardiac afterload. Adrenaline activates beta-1 receptors → tachycardia and increased contractility (initially) but then catecholamine-induced direct myocardial toxicity at high sustained concentrations — causing myocyte damage, impaired calcium handling, and acute reversible cardiomyopathy ('scorpion myocarditis' or stunned myocardium).
The transition from hypertension to shock: The paradoxical progression from hypertension to hypotension in severe envenomation is explained by the following sequence: initial catecholamine surge → peripheral vasoconstriction + increased afterload → left ventricular work increases sharply → combined with direct catecholamine myotoxicity → acute LV dysfunction → cardiac output falls despite high SVR → cardiogenic shock with pulmonary oedema. In this context, the peripheral vasoconstriction (high afterload) is the primary driver of the cardiac failure — which is why prazosin, an alpha-1 blocker that reduces afterload, is the correct pharmacological intervention.
Scorpion Envenomation: Catecholamine Storm to Shock
SELF-CHECK
A child with scorpion envenomation initially presents with BP 180/110 mmHg, HR 160/min, profuse sweating, and vomiting. Two hours later his BP falls to 75/40 mmHg with pulmonary oedema. The BEST explanation for the transition from hypertension to hypotension is:
A. The venom has a biphasic effect — initially stimulatory, then directly vasodilatory as the toxin binds to blood vessel walls
B. The sweating and vomiting caused hypovolaemia, reducing blood pressure
C. Catecholamine-induced increased afterload caused LV failure and cardiogenic shock, compounded by direct myocardial toxicity
D. The parasympathetic phase of the autonomic storm is suppressing the sympathetic phase
Reveal Answer
Answer: C. Catecholamine-induced increased afterload caused LV failure and cardiogenic shock, compounded by direct myocardial toxicity
The pathophysiological explanation for the hypertension-to-shock transition is catecholamine-mediated. The initial catecholamine surge causes intense alpha-1-mediated peripheral vasoconstriction, dramatically increasing afterload. The left ventricle, already compromised by direct catecholamine myotoxicity (stunned myocardium), cannot sustain output against this high afterload — it fails acutely, causing cardiogenic shock with pulmonary oedema. The shock is therefore caused by the same catecholamines that initially caused hypertension, by the mechanism of increasing left ventricular work beyond its capacity. This understanding explains why prazosin (afterload reduction) is the specific treatment.
Diagnosis and Initial Assessment
The diagnosis of scorpion envenomation is primarily clinical — there is no bedside confirmatory test and no species-specific laboratory marker. The diagnosis is made on the basis of: a history consistent with a scorpion sting (sudden onset severe pain, usually at night, often while sleeping or putting on shoes), identification of the scorpion if possible (small, dark reddish-brown for M. tamulus), and the presence of the characteristic autonomic features. In endemic areas, a child presenting at night with severe pain, sweating, hypertension, and vomiting after waking from sleep is a scorpion sting until proven otherwise.
Provided image
History: Establish the time of the sting, the location on the body (hands and feet are most common — scorpions hide in shoes, bedclothes, and cracks in walls), and the progression of symptoms. The speed of symptom escalation is clinically important: rapid progression from local pain to systemic features within 1–2 hours indicates significant envenomation and warrants hospital admission regardless of the initial blood pressure.
Physical examination:
- Vital signs: blood pressure (hypertension or hypotension — document both), heart rate and rhythm, respiratory rate, temperature, and oxygen saturation.
- Sting site: local pain, sweating, erythema. Often difficult to see — a small puncture wound or none visible.
- Cardiovascular: apex beat character, added heart sounds (gallop in LV failure), JVP elevation. Look for signs of pulmonary oedema: tachypnoea, accessory muscle use, basal crepitations, SpO2 falling.
- Neurological: pupil size (mydriasis = sympathetic dominant), agitation vs sedation, muscle fasciculations (sympathetic activation at the neuromuscular junction).
- Priapism: a specific sign of autonomic stimulation, reported particularly in children with severe envenomation.
Investigations:
- ECG — mandatory. Look for: sinus tachycardia, ST changes (myocarditis pattern), QTc prolongation, heart block, ventricular arrhythmias.
- Chest X-ray — evidence of pulmonary oedema (bilateral infiltrates, cardiomegaly, Kerley B lines).
- Echocardiogram — if available, LV function assessment is the most informative test for severity; LVEF may be severely reduced (scorpion myocarditis) even with brief envenomation.
- Blood tests: Full blood count, electrolytes, serum creatinine, blood glucose (hyperglycaemia from catecholamine-mediated gluconeogenesis), cardiac troponin (elevated in significant myocardial injury), serum amylase (pancreatitis is a recognised complication).