Page 11 of 20
IM21.8 | Scorpion Envenomation — SDL Guide (Part 2)
Management: Prazosin and Supportive Care
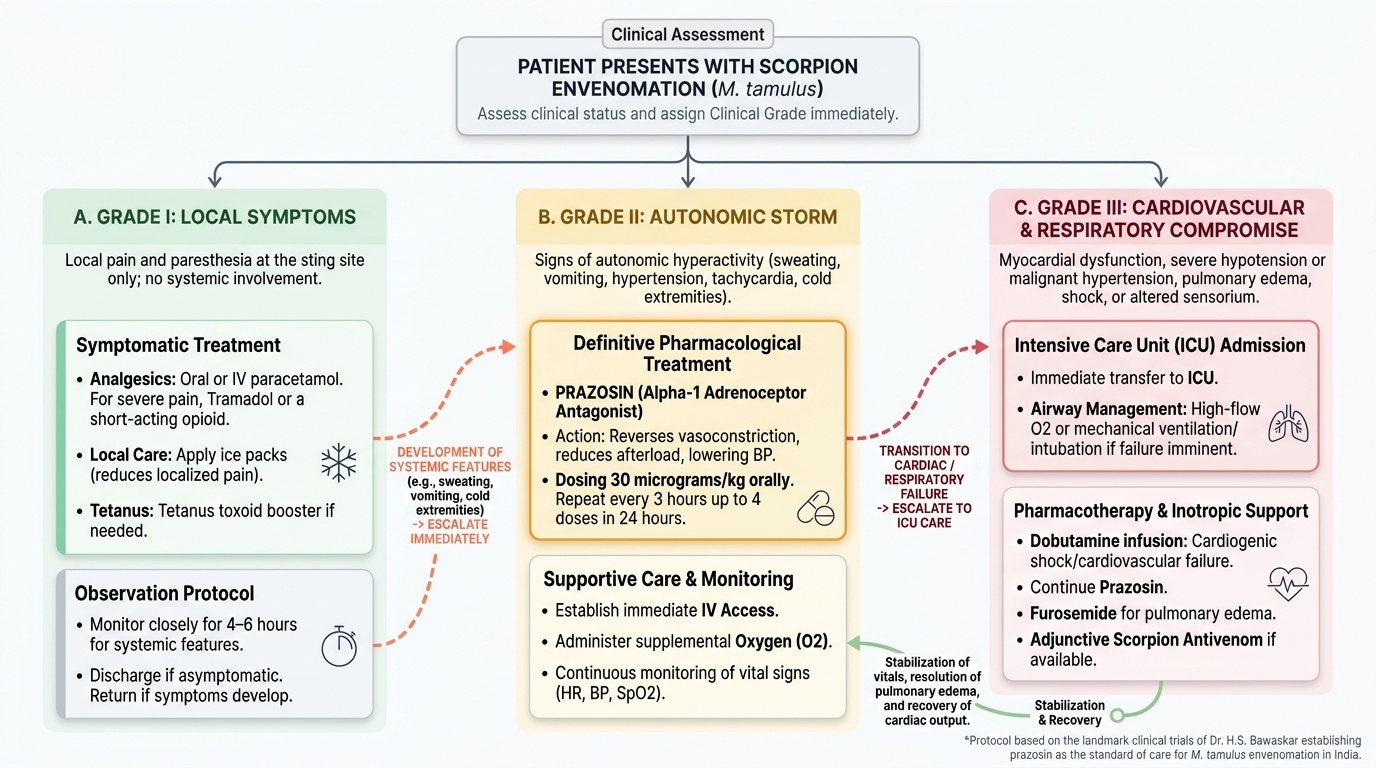
Management of scorpion envenomation is a stepwise protocol based on clinical grade, with prazosin as the specific pharmacological treatment for Grade II and III envenomation. Supportive care addresses cardiovascular failure, respiratory compromise, and pain. There is no widely available scorpion antivenom in India; even where available, antivenom is adjunctive. The treatment protocol outlined below is based on the work of Dr H.S. Bawaskar (Karjat, Maharashtra), whose landmark clinical trials established prazosin as the standard of care for M. tamulus envenomation in India. The critical principle is that treatment must be matched to grade: Grade I requires only symptomatic treatment, but Grade II demands immediate specific pharmacological intervention with prazosin to prevent progression to the life-threatening Grade III. Delayed or withheld prazosin is the single most common preventable cause of death from scorpion envenomation in India. Similarly, Grade III requires intensive care resources and inotropic support in addition to prazosin — the clinician must recognise the transition and escalate accordingly.
Provided image
Grade I — Local pain only:
- Analgesics: paracetamol oral or IV; for severe local pain, tramadol or a short-acting opioid.
- Local: ice pack application to the sting site (reduces pain).
- Tetanus toxoid if not up to date.
- Observation for 4–6 hours for development of systemic features. If none, discharge with advice to return if sweating, vomiting, or difficulty breathing develops.
Grade II — Autonomic storm (prazosin is the definitive treatment):
Prazosin is an alpha-1 adrenoceptor antagonist that blocks the noradrenaline-mediated peripheral vasoconstriction at the root of the pathophysiology. By blocking alpha-1 receptors, prazosin reverses the peripheral vasoconstriction, reduces afterload on the failing left ventricle, lowers blood pressure, and allows cardiac output to recover. The drug acts both as an antihypertensive and as an afterload-reducing agent in incipient cardiac failure.
Dose: Prazosin 30 micrograms/kg orally (maximum 1 mg in children; usual dose 250–500 micrograms in adults). May be repeated every 3 hours up to a maximum of 4 doses in 24 hours if clinical response is incomplete. The oral route is used because prazosin has reliable oral bioavailability and good first-pass absorption. Response is typically seen within 30–60 minutes: reduction in heart rate, fall in blood pressure towards normal, improvement in sweating, and improvement in peripheral perfusion.
Monitoring during prazosin: measure blood pressure every 15–30 minutes for the first 2 hours. Prazosin can cause a first-dose hypotension (a drop in blood pressure with the first dose, especially in a supine patient with already-compromised cardiac function) — monitor carefully and ensure IV access is established before giving the drug.
Additional treatment for Grade II: IV access and crystalloid infusion for mild haemodynamic compromise. Ondansetron or metoclopramide for vomiting. Oxygen if SpO2 < 95%. ECG monitoring. Paediatric patients should be observed in a monitored bed — rapid deterioration to Grade III can occur within 30–60 minutes.
Grade III — Cardiovascular failure:
- Oxygen and respiratory support: high-flow oxygen; intubation and ventilation if pulmonary oedema is severe or SpO2 cannot be maintained > 92%.
- Prazosin continues as the afterload-reducing agent — it remains indicated even in Grade III, but the dose and timing must be calibrated carefully in frank shock (a severely hypotensive patient may not tolerate additional afterload reduction from prazosin; clinical judgement required).
- Dobutamine infusion (5–10 micrograms/kg/min IV) for cardiogenic shock with low cardiac output — a beta-1 agonist that improves myocardial contractility; used when cardiac output is severely compromised despite afterload reduction.
- IV furosemide for pulmonary oedema with adequate blood pressure (40–80 mg IV in adults; 1 mg/kg in children).
- Antivenom (if available): Scorpion antivenom raised against M. tamulus venom is available at some centres in Maharashtra and Gujarat; early administration (within 1–2 hours of sting) may attenuate the autonomic storm, but it is not universally stocked and the evidence base is weaker than for snakebite antivenom. Where available, antivenom is given in addition to prazosin, not instead of it.
- ICU admission for haemodynamic monitoring, continuous ECG, and management of arrhythmias.
SELF-CHECK
A 10-year-old child (20 kg) with scorpion envenomation has BP 165/100 mmHg, HR 145/min, profuse sweating, and vomiting but no evidence of pulmonary oedema. SpO2 is 98% on room air. What is the drug of first choice and its dose?
A. Amlodipine 5 mg orally — calcium channel blocker to reduce hypertension
B. Atenolol 25 mg orally — beta-blocker to reduce heart rate and blood pressure
C. Prazosin 30 micrograms/kg orally (= 600 micrograms for this child) — alpha-1 blocker targeting the pathophysiological mechanism
D. Nifedipine 10 mg sublingually — rapid-acting calcium channel blocker for hypertensive emergency
Reveal Answer
Answer: C. Prazosin 30 micrograms/kg orally (= 600 micrograms for this child) — alpha-1 blocker targeting the pathophysiological mechanism
Prazosin at 30 micrograms/kg orally is the specific treatment for Grade II scorpion envenomation from Mesobuthus tamulus. For a 20 kg child: 30 × 20 = 600 micrograms (maximum 1 mg). Prazosin targets the alpha-1 receptor — the key mediator of the catecholamine-driven vasoconstriction — and reduces both hypertension and cardiac afterload, addressing the pathophysiology rather than just the blood pressure number. Atenolol (beta-blocker) is contraindicated — blocking beta-1 receptors in a patient with catecholamine excess and impending LV failure reduces cardiac output and may precipitate complete cardiovascular collapse. Nifedipine sublingual for hypertensive emergency is an outdated practice. Amlodipine has no proven role.
Self-Assessment: Scorpion Envenomation Recognition and Response
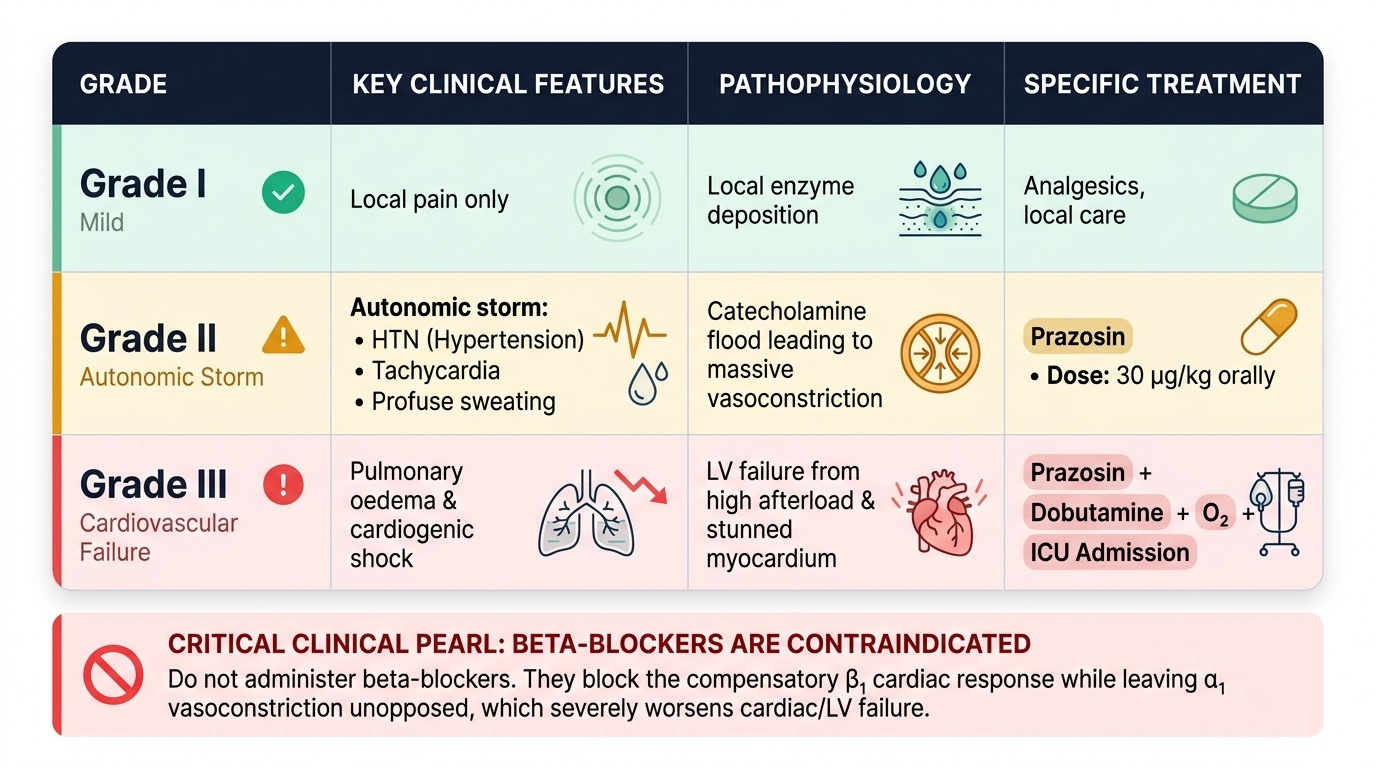
Self-assessment in scorpion envenomation requires mastery of the grading system and the specific therapeutic logic that distinguishes this condition from all other medical emergencies. The two high-yield exam facts are: (1) prazosin is the specific treatment, with the dose of 30 micrograms/kg orally, and (2) beta-blockers are contraindicated because they block the compensatory beta-1 cardiac response while leaving the alpha-1 vasoconstriction unopposed, worsening cardiac failure. These are examined at the KH level (knowledge applied to case scenarios) and appear in case-based MCQs, short answer questions, and clinical vivas. Working through the scenarios below from the perspective of 'which grade? which treatment?' consolidates the competency. The grading schema is the cognitive scaffold that converts a frightening, rapidly deteriorating paediatric emergency into a protocol-driven sequence of assessments and decisions. Once the three grades and their treatments are memorised and logically understood, the clinical encounter becomes manageable even under pressure — and recognising Grade II early, before the child progresses to Grade III, is the skill that saves lives in district hospitals across India.
Provided image
Scenario A: A 7-year-old girl (15 kg) is brought in at midnight with severe pain in her right hand that started 45 minutes ago. She is sweating profusely, has vomited twice, and is agitated. Her BP is 155/95 mmHg, HR 138/min, SpO2 99%. No respiratory distress. What grade is this, what is the treatment, and what is the prazosin dose?
Analysis: Grade II — autonomic storm (hypertension, tachycardia, sweating, vomiting, no pulmonary oedema). Treatment: prazosin orally. Dose: 30 mcg × 15 kg = 450 micrograms orally. Establish IV access. Give oxygen. Monitor BP every 15–30 minutes. Admit to monitored bed — watch for progression to Grade III.
Scenario B: The same child, 2 hours after prazosin dose: BP is now 80/50 mmHg, she has new respiratory distress with SpO2 89% on room air, and basal crepitations are audible. ECG shows sinus tachycardia with ST changes. What has happened and what is the immediate management?
Analysis: Grade III — cardiovascular failure. The prazosin has not reversed the Grade III progression (or may have been inadequate, or the cardiac dysfunction was already severe at presentation). Immediate management: high-flow oxygen (target SpO2 >92%), consider intubation if respiratory failure deepens, dobutamine infusion 5–10 mcg/kg/min IV for cardiogenic shock, IV furosemide for pulmonary oedema, ICU admission, continuous ECG monitoring. Prazosin may be continued with caution. Antivenom if available at the centre.
SELF-CHECK
A colleague suggests giving propranolol (a beta-blocker) to a patient with scorpion envenomation to control the tachycardia of 145/min. Why is this contraindicated?
A. Beta-blockers are nephrotoxic and contraindicated in any envenomation with renal risk
B. Beta-blockers block beta-1 cardiac receptors, reducing the compensatory cardiac output while leaving alpha-1-mediated vasoconstriction unopposed, precipitating cardiovascular collapse
C. Beta-blockers cause sedation and mask the agitation that is used to monitor envenomation severity
D. Beta-blockers are only contraindicated in children; they are safe in adults with scorpion sting
Reveal Answer
Answer: B. Beta-blockers block beta-1 cardiac receptors, reducing the compensatory cardiac output while leaving alpha-1-mediated vasoconstriction unopposed, precipitating cardiovascular collapse
Beta-blockers are specifically contraindicated in scorpion envenomation because of the pharmacological conflict. In an autonomic storm, catecholamines are causing both alpha-1 vasoconstriction and beta-1 cardiac stimulation. The beta-1 cardiac stimulation, while contributing to tachycardia, is also maintaining cardiac output against the high afterload. If beta-1 is blocked, the heart's compensatory response is abolished while alpha-1 vasoconstriction continues unopposed — afterload rises further, cardiac output falls catastrophically. The correct drug is prazosin (alpha-1 block), which removes the pathological vasoconstriction while preserving the beta-1-mediated cardiac compensation.
CLINICAL PEARL
The most dangerous mismanagement error in scorpion envenomation is treating the initial hypertension as an isolated hypertensive emergency and giving calcium channel blockers, sedatives, or simply 'watchful waiting' — all of which fail to address the autonomic storm and allow progression to pulmonary oedema and shock. The key insight from Dr Bawaskar's work in Maharashtra is that the hypertension and tachycardia of scorpion envenomation are not primary diagnoses — they are symptoms of the catecholamine flood from the autonomic storm, and the catecholamine flood is what kills the child. Prazosin addresses the catecholamine flood at its effector (alpha-1 receptor). Treating only the blood pressure number with a non-specific antihypertensive is like treating the smoke instead of the fire.
A practical pearl: when a child in Maharashtra or Andhra Pradesh presents at night with sweating, hypertension, and pain, examine the child first but simultaneously ask the family to look under the bedclothes and in the shoes for a scorpion. The clinical syndrome is so characteristic that in endemic areas it is taught as 'scorpion sting until proven otherwise' for this night-time paediatric presentation.