Page 4 of 20
IM21.4-6 | Snake Bite Clinical Evaluation and Testing — SDL Guide
Learning Objectives
- Conduct a structured 7-domain snakebite history capturing all clinically actionable elements
- Perform and document a systematic physical examination including local wound, haemostasis, cardiovascular, and the 5-element serial neurological examination for neurotoxic envenomation
- Perform and interpret the 20-minute whole-blood clotting test (20WBCT) correctly, including the glass-tube requirement and repeat-testing protocol
- Select and interpret a targeted investigation panel for haematotoxic and neurotoxic envenomation
- Recognise the count test as the key bedside indicator of impending respiratory failure in neurotoxic snakebite
INSTRUCTIONS
The clinical evaluation of snakebite is both a diagnostic skill and a monitoring discipline. This module builds the structured approach to history, examination, and investigations that transforms a disorganised emergency encounter into a purposeful clinical assessment. The 20WBCT and serial neurological exam are the two procedural anchors — master these and you have the essential toolkit for managing India's most common envenomation emergency.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 457 — Venomous Snakebites (textbook)
- API Textbook of Medicine, 10th ed. — Chapter on Envenomation (textbook)
- WHO Guidelines for the Management of Snakebites in South-East Asia, 2nd ed., 2016 (guideline)
- National Snakebite Management Protocol, Ministry of Health and Family Welfare, India, 2008 (revised) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two patients arrive within an hour of each other at the district hospital emergency department. The first is a 40-year-old farmer bitten on the right forearm two hours ago while cutting grass. The forearm is swollen to the elbow, there are two fang marks with surrounding ecchymosis, and he says his vision has become blurred. His blood pressure is 90/60 mmHg. The second is a 55-year-old woman brought by her son who found her unable to get out of bed at 5 AM. She has bilateral ptosis, cannot lift her head, and her voice is nasal and weak. The son says she may have stepped on something last night. The first patient has a dramatic wound; the second has barely anything to look at. Yet both are critically envenomated. How do you take a history that captures the critical features of each presentation? What examination findings do you specifically seek in each? Which investigations do you order — and which single bedside test, requiring nothing more than a clean dry glass tube, tells you whether the first patient needs antivenom right now?
WHY THIS MATTERS
The clinical evaluation of snakebite is a procedural skill that goes beyond ordinary history-taking and physical examination. It demands knowledge of which species-specific features to probe in the history, which systemic signs to actively elicit on examination, and which investigations to select and interpret to quantify envenomation severity. NMC competencies IM21.4–21.6 specifically require the ability to elicit and document a structured snakebite history, perform and present a systematic physical examination including neurological and cardiac components, and choose and interpret the appropriate diagnostic tests. These are skills assessed in clinical postings and OSCEs — the ability to articulate a structured approach demonstrates competency that a disorganised examination of 'swelling and bite marks' does not. The two cases in the hook illustrate the full spectrum: the evaluation of haematotoxic envenomation focuses on coagulation status and end-organ injury, while the evaluation of neurotoxic envenomation is a serial bedside neurological examination against the clock.
RECALL
Activate your prior knowledge of the neuromuscular junction and the coagulation cascade. Recall that ptosis results from weakness of the levator palpebrae superioris (CN III and sympathetic), that the earliest sign of neuromuscular blockade by neurotoxic venom is loss of voluntary eyelid elevation. Recall the components of respiratory muscle assessment — diaphragm, intercostal muscles, accessory muscles — and that the 'count test' (counting aloud to 20 in a single breath) gives a rapid bedside measure of vital capacity equivalent. Recall from pharmacology that acetylcholinesterase inhibitors (neostigmine) prevent breakdown of acetylcholine at the synapse, increasing its effective concentration; this can partially overcome post-synaptic (cobra) blockade but cannot compensate for absent presynaptic acetylcholine release (krait). Recall the 20-minute whole-blood clotting test principle: blood placed in a clean dry glass tube will clot within 8–10 minutes under normal circumstances; failure to clot at 20 minutes indicates severe defibrination.
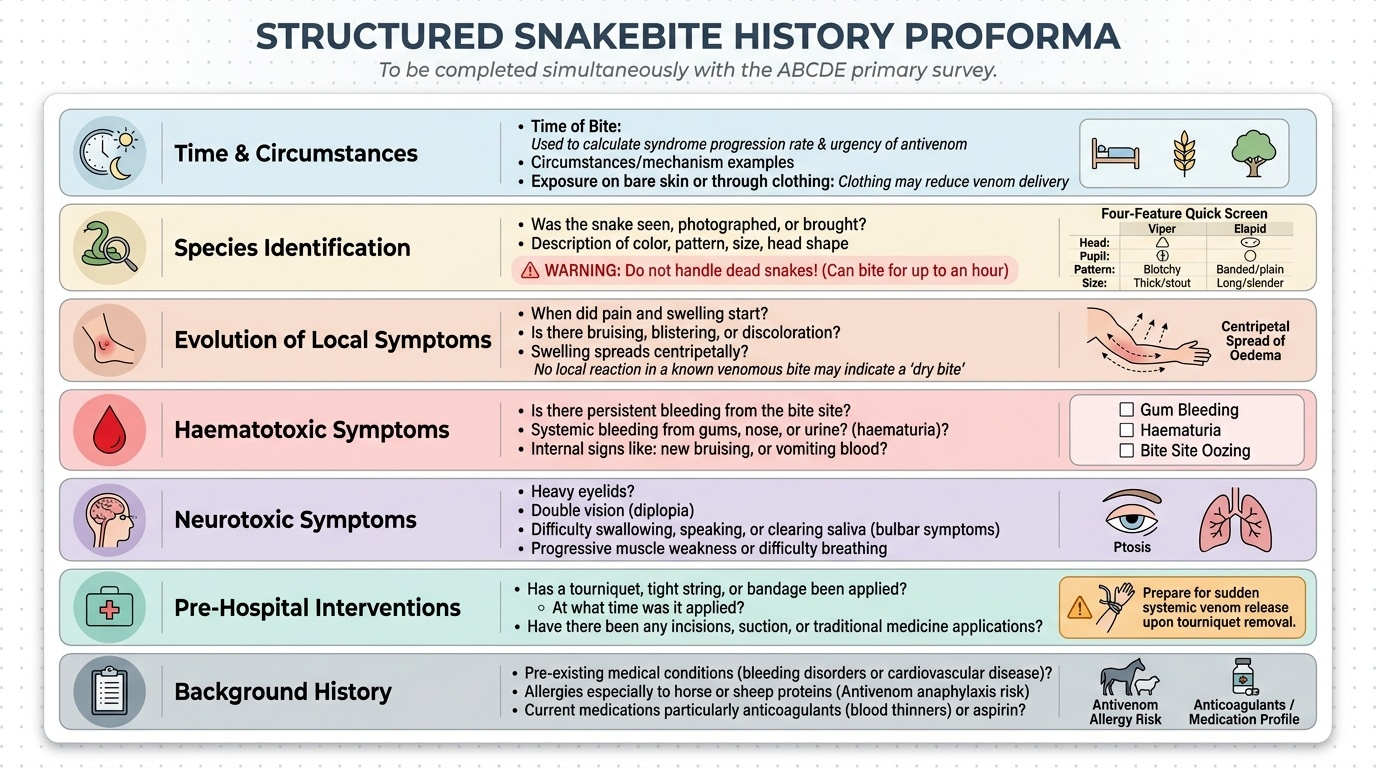
Structured Snakebite History: Key Elements and Clinical Reasoning
A structured snakebite history must capture seven domains in sequence, each informing a specific clinical decision. The history should be completed simultaneously with the primary survey — it is not a luxury to defer until after examination. Skilled clinicians conduct the ABCDE assessment and the history simultaneously by directing questions at both the patient and any accompanying person, because in envenomation, time from bite to antivenom is the single most modifiable determinant of outcome.
Provided image
The seven domains of the snakebite history are as follows:
1. Time and circumstances of the bite. Record the exact time of the bite, because the interval determines the urgency of antivenom and allows calculation of syndrome progression rate. The mechanism also matters: night-time bite while sleeping (krait), agricultural field bite during harvest (Russell's viper, saw-scaled viper), forest or jungle bite (king cobra, bamboo pit viper in north-east India). A bite through clothing may deliver less venom than a direct bite on bare skin.
2. Species identification. Ask: Did anyone see the snake? Was it killed and brought? If available, do not handle it (even a dead snake can reflexively bite for up to an hour). Describe the snake's colour, pattern, body shape, head shape, and approximate length — the four-feature quick screen is: head shape (triangular = viper; rounded/narrow = elapid), pupil shape (if seen: elliptical = viper; round = elapid), body pattern (blotches/bands/plain), and size. Even partial identification guides syndrome expectation.
3. Evolution of local symptoms. Document the onset and progression of pain, swelling, bruising, and any visible blistering or skin discolouration at or distal to the bite site. Local oedema spreads centripetally from the bite; its rate of spread and how far it has reached informs the degree of venom injection. A bite with absolutely no local reaction in a species known for significant local effects raises the possibility of a 'dry bite' (venom not injected) — though all patients should be observed for at least 24 hours regardless.
4. Evolution of systemic haematotoxic symptoms. Specifically ask about: spontaneous bleeding from any site (gums, nose, venepuncture sites, conjunctivae, urinary tract), coloured urine (haematuria from bleeding, red-brown myoglobinuria from myonecrosis), decreased urine output (early AKI), and abdominal pain (may indicate visceral haemorrhage). The sequence and timing of these symptoms guides whether the coagulopathy is worsening or improving after antivenom.
5. Evolution of systemic neurotoxic symptoms. Ask about: drooping eyelids (ptosis — the first symptom the patient or family often notices), double vision (ophthalmoplegia), difficulty swallowing or speaking (bulbar palsy), generalised weakness, and any difficulty breathing (impending respiratory failure). The timeline from bite to first neurotoxic symptom is critical — krait envenomation may present 6–12 hours after an apparently trivial bite.
6. Pre-hospital interventions. Document every intervention applied before arrival: tourniquet (location, how tight, duration applied), incisions or suction, oral medications or herbal preparations, any antivenom already given (where, how much, any reaction). This history directly changes management — a tourniquet that has been in place for two hours requires a specific gradual-release protocol; antivenom already given determines whether the total dose threshold has been approached.
7. Background medical history and allergies. Note prior atopy (asthma, eczema, allergic rhinitis), prior antivenom exposure (sensitisation risk), pregnancy status (antivenom is not contraindicated in pregnancy), and any anticoagulant use (warfarin, antiplatelet agents) that worsens haematotoxic coagulopathy.
Systematic Physical Examination in Snakebite
The physical examination in snakebite is structured around the ABCDE framework but must be extended with specific snakebite components — particularly the neurological examination for neurotoxic envenomation and the haemostasis examination for haematotoxic envenomation. The examination is not a one-time event: it is repeated every 30 minutes in the acute phase and the clinical course is documented serially so that deterioration is detected before it becomes irreversible. Document all findings against time-stamps so that the progression of envenomation can be tracked.
General examination: Assess consciousness level (GCS or AVPU), anxiety, agitation, and whether the patient looks 'toxic'. Note vital signs: pulse rate and character, blood pressure (hypotension in viper envenomation), respiratory rate (rising rate = neuromuscular compromise), temperature (fever may indicate secondary infection or venom-related inflammation), and oxygen saturation (SpO2 < 95% = respiratory compromise in neurotoxic envenomation). A falling SpO2 with ptosis is an emergency — intubation threshold has been reached.
Local examination of the bite site: Inspect the wound carefully. Document: number of fang marks (single or double puncture), distance between fang marks (larger distance = larger snake), local swelling and its extent (measure circumference of the bitten limb at the wound site and 5 cm proximal, mark the leading edge of swelling with a pen and re-check every 30 minutes to track spread rate), bruising, blistering, local necrosis (black or grey discolouration of skin = cytotoxic venom), and lymphangitis or regional lymphadenopathy.
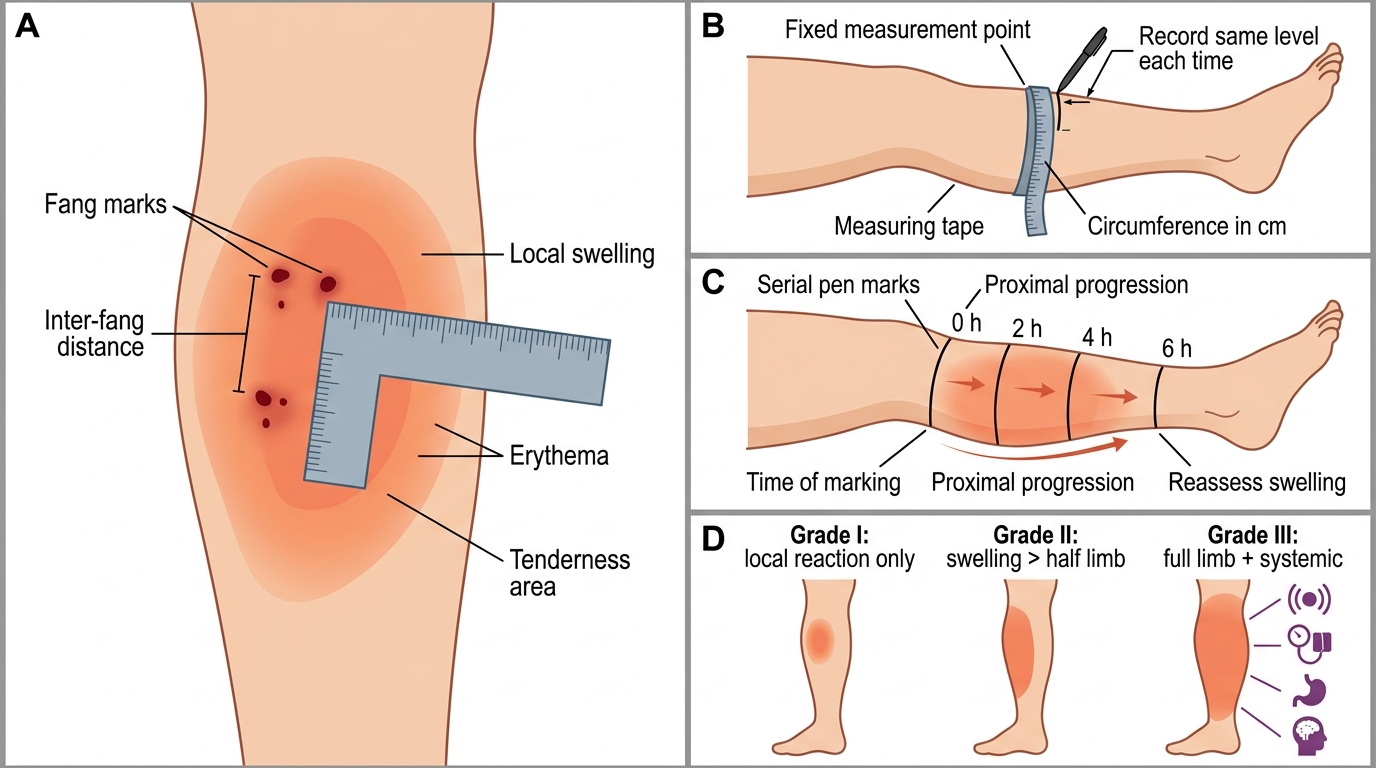
Local Snakebite Site Examination and Severity Grading
Cardiovascular examination: Measure blood pressure in both arms. Tachycardia may reflect pain, anxiety, or autonomic effects of venom. Hypotension indicates systemic envenomation — viper venoms cause vasodilation and distributive shock. A widened pulse pressure or bradycardia can indicate specific autonomic toxicity. Auscultate for pericardial rub (haemopericardium is rare but reported with severe haematotoxic envenomation). ECG is indicated for any haemodynamically unstable patient and for scorpion envenomation (covered in the next module).
Neurological examination — the most critical component in elapid envenomation: Perform and document the following in sequence, repeating every 30 minutes:
- Ptosis assessment: Ask the patient to open their eyes as wide as possible. Measure the palpebral aperture or simply note whether ptosis is present. Ptosis is the earliest and most sensitive sign of neuromuscular blockade; its appearance demands immediate antivenom administration.
- Ophthalmoplegia: Ask the patient to track your finger through the full range of gaze (H-pattern). Any restriction indicates involvement of the extraocular muscles.
- Bulbar function: Ask the patient to speak (note nasal quality indicating palatal weakness), to swallow (inability is a sign of advanced bulbar palsy and aspiration risk), and to protrude their tongue.
- Neck flexion strength: Ask the patient to lift their head off the pillow and resist your hand pushing it down. This tests the cervical flexors — one of the earliest groups to weaken in neurotoxic envenomation. Inability to lift the head is a major danger sign.
- Respiratory function — the 'count test': Ask the patient to take one deep breath and count aloud to 20 in a single breath. If they cannot reach 20 or become breathless, this indicates significant respiratory muscle compromise. A formal bedside spirometry reading of FVC < 15–20 mL/kg is an intubation threshold in neuromuscular disease; in resource-limited settings, the count test serves as a surrogate.
- Limb power and deep tendon reflexes: Grade power (MRC scale 0–5) in all four limbs. Deep tendon reflexes may be preserved early but are reduced as paralysis deepens.
Haemostasis examination: Look specifically for bleeding at the following sites — gingival margin (oozing), conjunctival haemorrhage, petechiae and ecchymoses on the skin, blood at venepuncture sites (failure to clot after needle withdrawal), nasal bleeding, and urinary blood (inspect urine colour). Observe blood drawn for investigations: if it clots normally in the collection tube, gross coagulopathy is unlikely; if the blood remains liquid after 15 minutes, severe VICC is present. This bedside observation supplements the formal 20WBCT.
SELF-CHECK
A 30-year-old man bitten on the left leg 3 hours ago has bilateral ptosis and can only count to 8 before becoming breathless. His oxygen saturation is 92% on room air. The MOST immediately important action is:
A. Order an urgent serum acetylcholinesterase level to confirm neurotoxicity
B. Start neostigmine 1.5 mg IV with atropine 0.6 mg IV and reassess in 30 minutes
C. Prepare for urgent endotracheal intubation and begin antivenom simultaneously
D. Transfer to a higher centre with an ICU before starting antivenom
Reveal Answer
Answer: C. Prepare for urgent endotracheal intubation and begin antivenom simultaneously
SpO2 of 92% with ptosis and a count test of only 8 indicates rapidly progressive neurotoxic respiratory failure. This patient is at or past the intubation threshold. Immediate airway securing by endotracheal intubation is the priority — respiratory arrest can occur within minutes. Antivenom should be started simultaneously (not sequentially) because antivenom will limit further paralysis even if it cannot reverse established blockade quickly. Waiting for neostigmine trial first is too slow in this context. Transferring before airway is secured risks fatal respiratory arrest in transit. Serum acetylcholinesterase is not a clinically useful urgent test in snakebite.
The 20-Minute Whole Blood Clotting Test (20WBCT)
The 20-minute whole-blood clotting test (20WBCT) is the cornerstone bedside investigation for haematotoxic snakebite in resource-limited settings. It requires nothing more than a clean, dry glass tube, 2–3 mL of freshly drawn venous blood, and a 20-minute wait. Its simplicity belies its clinical importance: it directly tests the functional end-point of the coagulation cascade (clot formation) and provides an actionable binary result — clot present or absent — that guides antivenom administration without waiting for formal coagulation studies to return from the laboratory. At a primary health centre where PT/INR facilities are unavailable, the 20WBCT is the entire haematological assessment of envenomation severity.
Technique: Draw 2–3 mL of venous blood into a new, clean, dry glass tube (plastic tubes are unsuitable — glass contact activation is required for the test). Place the tube upright in a test tube rack at room temperature. Do not refrigerate, agitate, or tilt. Leave undisturbed for exactly 20 minutes. At 20 minutes, tilt the tube to 45 degrees and observe whether the blood has clotted. A clot that holds when the tube is tilted = negative test (coagulation is functional). Blood that remains liquid, runs freely when the tube is tilted, or forms only a fragile partial clot = positive test indicating defibrination coagulopathy from VICC.
Interpretation:
- 20WBCT negative (clot at 20 min): No significant coagulopathy. Repeat every 30 minutes for the first 2–3 hours (VICC can develop progressively). If still negative at 6 hours post-bite and no other systemic signs, antivenom is not indicated on coagulopathy grounds.
- 20WBCT positive (no clot at 20 min): VICC is present. This is an absolute indication for polyvalent anti-snake venom (ASV) — administer immediately regardless of which species is suspected (polyvalent ASV covers all four big four species).
Important caveats:
1. The tube MUST be glass and must be dry and clean — even trace moisture or plastic material gives false results.
2. The test detects defibrination (loss of fibrinogen and clotting factors) but does NOT detect isolated thrombocytopenia, which can also cause bleeding in viper envenomation. Therefore, a negative 20WBCT in the presence of active bleeding from multiple sites should prompt formal laboratory coagulation studies.
3. After antivenom administration, repeat the 20WBCT at 6 hours post-antivenom. Correction of the coagulopathy (clot forms at 20 min) is the best evidence that the administered antivenom dose has been effective. If WBCT is still positive at 6 hours post-antivenom, a second dose of antivenom may be required.
4. The 20WBCT does NOT assess neurotoxicity — it is a haematological test only.
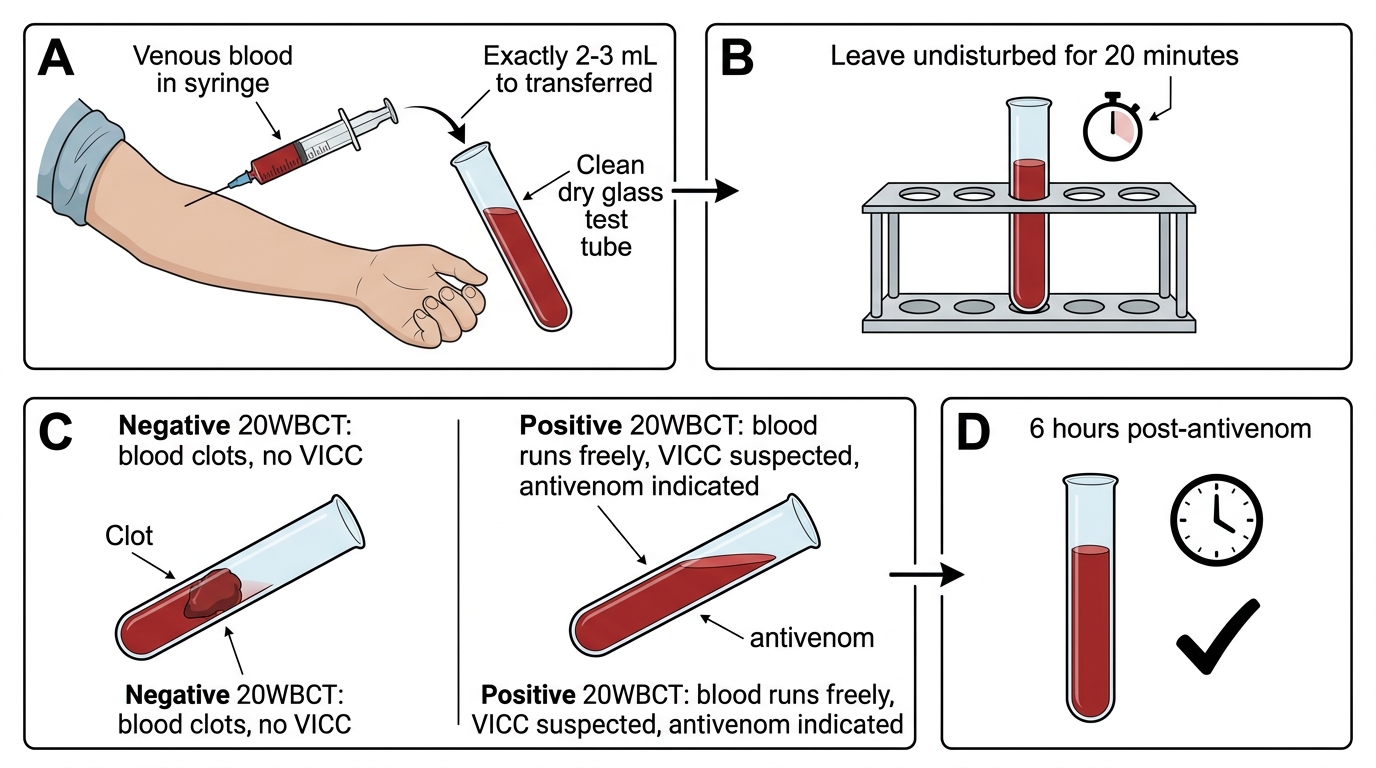
20-Minute Whole Blood Clotting Test for VICC