Page 5 of 20
IM21.4-6 | Snake Bite Clinical Evaluation and Testing — SDL Guide (Part 2)
Laboratory Investigations: Selection and Interpretation
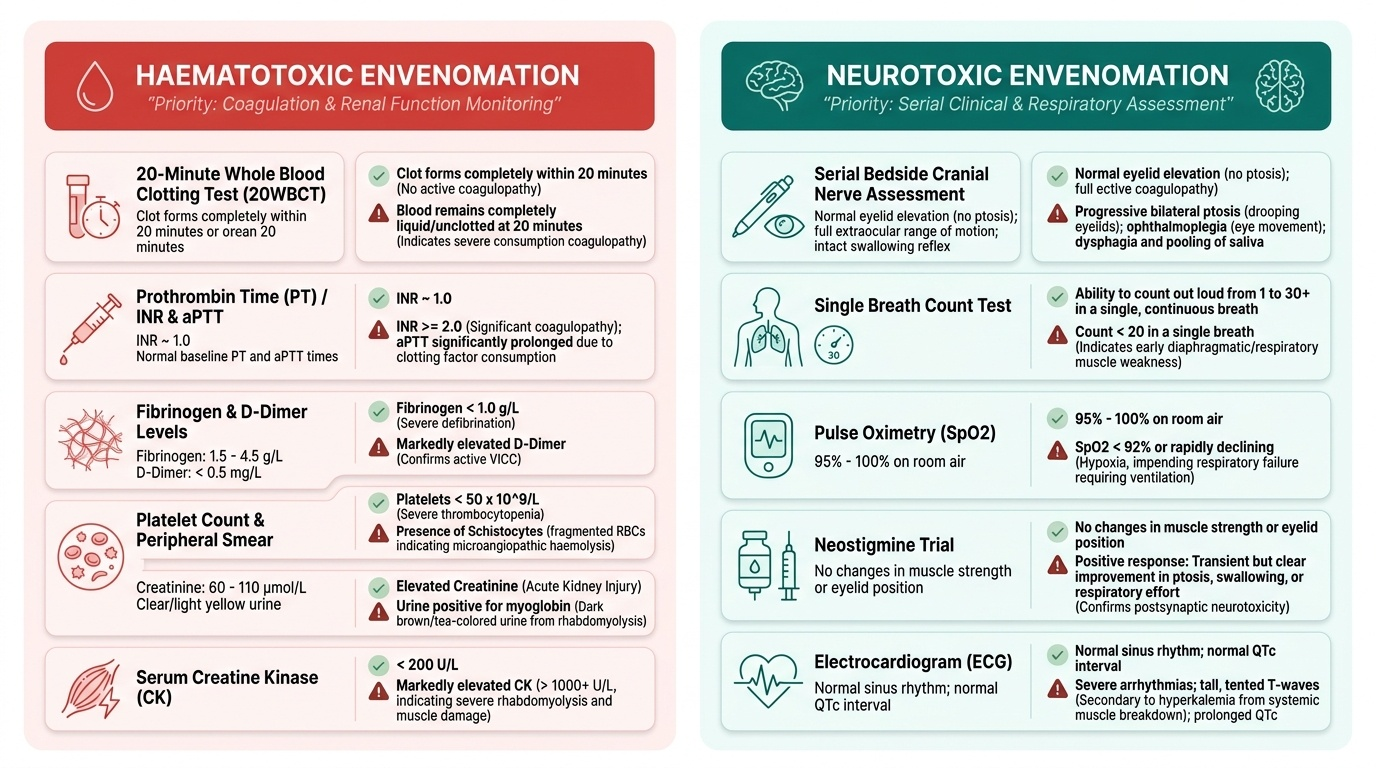
Beyond the bedside 20WBCT, a panel of targeted laboratory investigations provides quantitative data on envenomation severity, guides supportive management decisions, and monitors response to antivenom. The selection of tests should be guided by the anticipated syndrome (haematotoxic vs neurotoxic) and the clinical urgency, but in any patient with suspected systemic envenomation the following panel is standard. Not all tests are available at every level of care — the clinician must know which are priority and which can be deferred during transfer. A key principle is that investigations should never delay antivenom: blood can be drawn at the same time the antivenom infusion is being set up. The priority investigations are those that confirm the envenomation syndrome, quantify end-organ injury, and provide baseline values against which response to antivenom will be measured at 6 and 24 hours. For haematotoxic envenomation, the coagulation panel and renal function are the two most critical data points; for neurotoxic envenomation, the diagnosis is clinical and no blood test substitutes for serial bedside examination.
Provided image
Coagulation studies (priority in haematotoxic envenomation):
- Prothrombin time (PT) and INR: The PT is prolonged in VICC because factors in the extrinsic pathway are consumed; an INR > 2.0 indicates significant coagulopathy.
- Activated partial thromboplastin time (aPTT): Prolonged when intrinsic pathway factors (VIII, IX, XI) are consumed.
- Serum fibrinogen: The most sensitive marker of VICC — fibrinogen is the first protein consumed; levels < 1 g/L indicate severe defibrination.
- D-dimer: Markedly elevated in VICC, confirming the consumptive process.
- Platelet count: Thrombocytopenia is prominent with saw-scaled viper envenomation specifically; may contribute to bleeding independently of the coagulopathy. A platelet count < 50 × 10⁹/L with active bleeding may warrant platelet transfusion alongside antivenom.
Haematological studies:
- Full blood count: Anaemia from haemolysis or blood loss; neutrophilia from the inflammatory response to venom.
- Peripheral blood smear: Schistocytes (fragmented red cells) indicate microangiopathic haemolysis; this is an important finding in Russell's viper envenomation where microangiopathy contributes to AKI.
- Reticulocyte count: Elevated in haemolytic anaemia.
Renal function (priority in Russell's viper envenomation):
- Serum creatinine and urea: The most important serial parameters for monitoring AKI. A rising creatinine with oliguria demands aggressive IV fluid resuscitation and nephrology review. AKI in Russell's viper envenomation can be severe enough to require dialysis.
- Serum electrolytes: Hyperkalaemia from haemolysis and myonecrosis; metabolic acidosis from AKI.
- Urine dipstick and microscopy: Blood on dipstick = haematuria or myoglobinuria. Red-brown urine with blood on dipstick but no red cells on microscopy = myoglobinuria (pigment nephropathy risk). Casts on microscopy confirm tubular injury.
Muscle enzyme studies:
- Creatine kinase (CK): Markedly elevated in myonecrosis from viper venom phospholipase A2; CK > 10,000 IU/L indicates severe rhabdomyolysis with risk of pigment nephropathy. Serial CK guides the adequacy of IV hydration in rhabdomyolysis management.
Hepatic function:
- ALT, AST, bilirubin: Elevated in hepatocellular injury from viper venom; jaundice may be haemolytic or hepatocellular.
Neurological monitoring investigations (for neurotoxic envenomation):
- No single blood test confirms or grades neurotoxicity. The diagnosis is entirely clinical — serial bedside neurological examination is the monitoring tool.
- Neostigmine test: In suspected cobra envenomation with established ptosis, an empirical trial of neostigmine 1.5 mg IV + atropine 0.6 mg IV (atropine pre-empts muscarinic side effects of neostigmine) may show partial improvement of ptosis within 15–30 minutes if the block is post-synaptic (cobra). No improvement suggests pre-synaptic (krait) or that the block is already irreversible.
- ECG: Mandatory in any patient with haemodynamic compromise or autonomic instability.
SELF-CHECK
A 45-year-old man bitten by a Russell's viper has a positive 20WBCT (no clot). His serum creatinine is 1.8 mg/dL (baseline unknown), urine is dark red-brown, and urine dipstick shows 3+ blood but no red cells on microscopy. His CK is 18,500 IU/L. Which complication is the dark urine most likely indicating, and what is the immediate supportive priority?
A. Haematuria from renal vein thrombosis — start anticoagulation
B. Myoglobinuria from rhabdomyolysis — aggressive IV fluid hydration to prevent pigment nephropathy
C. Bilirubinuria from hepatic necrosis — start N-acetylcysteine
D. Haemoglobinuria from DIC — transfuse packed red cells
Reveal Answer
Answer: B. Myoglobinuria from rhabdomyolysis — aggressive IV fluid hydration to prevent pigment nephropathy
Dark red-brown urine with blood on dipstick but no red cells on microscopy is the classic finding of myoglobinuria — myoglobin is detected as haem by the dipstick but is not visible as intact red cells under the microscope. The markedly elevated CK (18,500 IU/L) confirms severe rhabdomyolysis from viper venom phospholipase A2-mediated myonecrosis. The immediate supportive priority is aggressive IV fluid hydration (normal saline at 200–300 mL/hour targeting urine output ≥200 mL/hour) to flush myoglobin casts from the tubules and prevent pigment nephropathy. Rising creatinine confirms early AKI. Antivenom must also be administered urgently for the underlying VICC.
Applied Practice: Putting the Evaluation Together
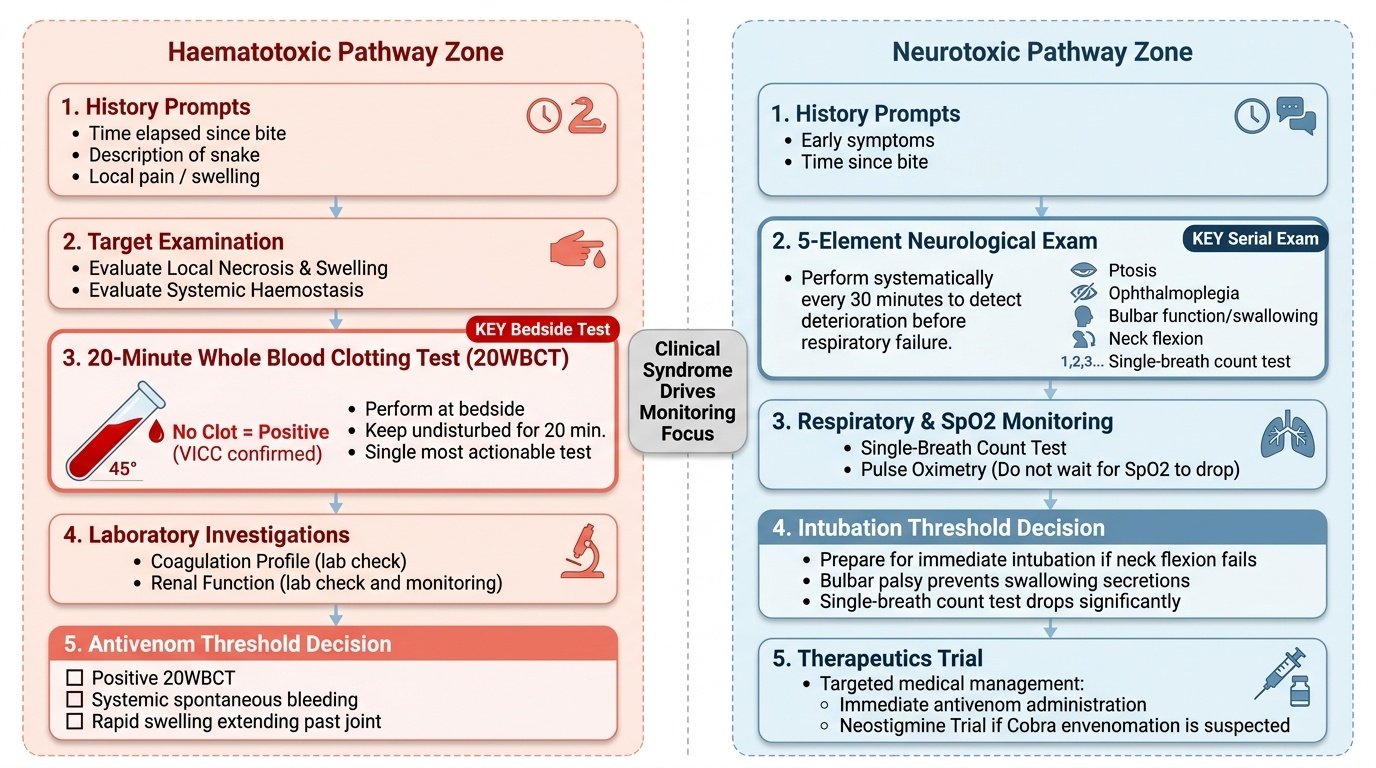
Bringing together the history, examination, and investigations into a coherent clinical evaluation requires a mental algorithm that is practiced until it becomes automatic. In the real snakebite encounter, you will be managing the airway with one hand, drawing blood for the 20WBCT with the other, asking history questions from the accompanying relative, and mentally calculating the syndrome and antivenom need — all simultaneously. The applied practice scenarios below walk you through this integration for both the haematotoxic and neurotoxic presentation.
Provided image
The key principle of integrated snakebite evaluation is that the clinical syndrome drives the monitoring focus, and the 20WBCT is the single most actionable test in haematotoxic envenomation. For neurotoxic envenomation, there is no equivalent bedside lab test — the serial neurological examination is both the diagnostic and monitoring instrument. A clinician who can perform a precise 5-element neurological exam (ptosis, ophthalmoplegia, bulbar function, neck flexion, count test) every 30 minutes and detect deterioration before SpO2 falls has mastered the most important clinical skill in neurotoxic snakebite management.
Scenario — Haematotoxic evaluation: A 38-year-old farmer is brought in 90 minutes after a bite on the left calf. The snake was described as brownish with a triangular head and rough scales. On examination: BP 100/70 mmHg, HR 100/min, the wound has two fang marks with swelling extending to mid-thigh, there is bruising tracking up the limb, gum margins are oozing blood, and blood drawn for investigations remains liquid in the collection tube. The 20WBCT is performed: at 20 minutes, the tube is tilted and the blood runs freely — positive test. Summary: this is a haematotoxic envenomation (likely Russell's viper or saw-scaled viper based on description) with VICC confirmed by 20WBCT. Antivenom indication: YES — positive 20WBCT + active systemic bleeding. Send coagulation studies, renal function, CK, urine dipstick simultaneously but do not delay antivenom.
Scenario — Neurotoxic evaluation: The 55-year-old woman from the opening hook: ptosis present bilaterally, count test 8/20, neck flexion power grade 3/5, SpO2 92%. History: found at 5 AM, possible bite overnight, no local swelling. Summary: pre-synaptic neurotoxic envenomation consistent with krait. Antivenom indication: YES — established neurotoxic signs. Neostigmine trial: can be attempted (neostigmine 1.5 mg + atropine 0.6 mg IV) but pre-synaptic block means response is unlikely and airway must be secured first. Intubate first, then administer antivenom and attempt neostigmine. Ventilatory support will be required for days to weeks.
Self-Assessment: Integrating History, Examination, and Investigations
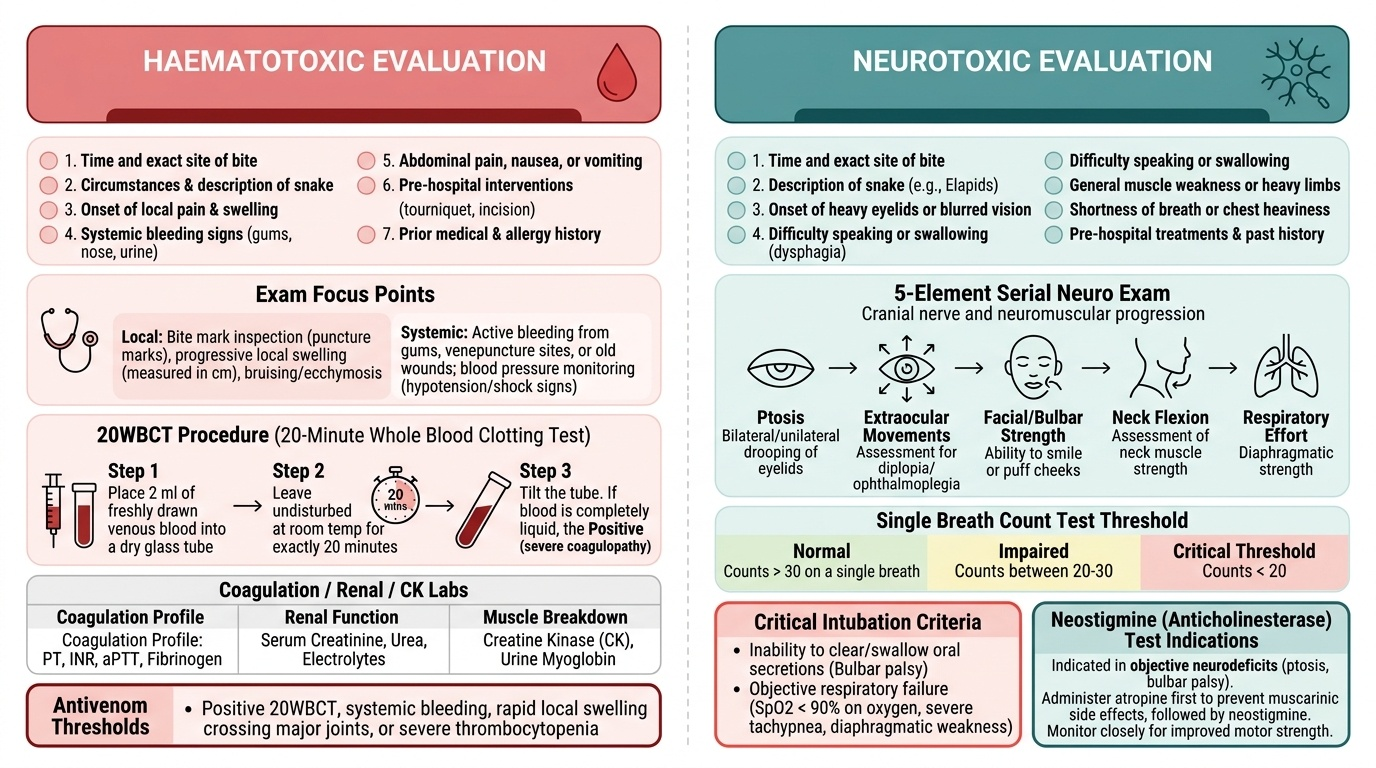
This self-assessment section consolidates your clinical evaluation skills by asking you to apply the full structured approach — history, examination, and investigation selection — to two contrasting presentations. The IM-skills arc for this module requires you to demonstrate the ability to elicit and present a snakebite history (IM21.4), perform and document the systematic examination including neurological components (IM21.5), and select and interpret appropriate diagnostic tests (IM21.6). Each scenario below presents a clinical vignette; work through the structured evaluation mentally before reading the analysis. Aim to complete each scenario in under two minutes, as you would need to in a real emergency. The ability to simultaneously conduct history, examination, and testing while communicating to your team is the hallmark of clinical competency in the acute snakebite encounter.
Provided image
Scenario A: A 52-year-old man is brought in at 9 PM, 2.5 hours after a bite on the right foot while walking in his garden. He is conscious but anxious. No snake was seen. His foot has two puncture marks with 4+ cm of swelling. On examination: BP 95/65 mmHg, HR 110/min. His gum line is oozing blood. Blood drawn for IV cannulation does not clot in the collection tube after 10 minutes. No ptosis. Question: (1) What syndrome is this? (2) What single bedside test confirms the coagulation status? (3) Is antivenom indicated before that test result?
Analysis: Haematotoxic envenomation — gingival bleeding, non-clotting blood, hypotension. Confirming bedside test: 20WBCT in clean dry GLASS tube. Is antivenom indicated before the test: YES — active systemic bleeding (gingival oozing) is itself an indication for antivenom. Do not wait for the 20WBCT result if systemic bleeding is already present. Order the test, start the antivenom infusion simultaneously.
Scenario B: A 24-year-old woman is brought in at 7 AM by her husband. She was found unable to get up, with drooping eyelids. She has a small 3 mm puncture wound on her left ankle. Her voice is nasal. She can count to 12 before becoming breathless. Neck flexion: 3/5. SpO2 94% on room air. Question: (1) What is the most likely species and envenomation type? (2) What is the immediate investigation priority? (3) At what count test value should you prepare for intubation?
Analysis: Pre-synaptic neurotoxic envenomation, consistent with common krait (nocturnal, painless, minimal local reaction, descending paralysis). Investigation priority: this is a clinical diagnosis — no blood test changes immediate management. Serial neurological examination IS the investigation. Intubation preparation: count ≤10, SpO2 <95%, or neck flexion ≤grade 3 — this patient meets all three. Intubate, start antivenom, and arrange ICU ventilatory support.
SELF-CHECK
During the examination of a snakebite patient with suspected neurotoxic envenomation, which of the following bedside assessments is the MOST sensitive early indicator of impending respiratory failure?
A. SpO2 falling below 95% on pulse oximetry
B. Inability to lift the head off the pillow (neck flexor weakness)
C. Inability to count to 20 in one breath (count test), reflecting reduced vital capacity
D. Bilateral ptosis with restricted upward gaze
Reveal Answer
Answer: C. Inability to count to 20 in one breath (count test), reflecting reduced vital capacity
The count test (ability to count to 20 in a single breath) is the most sensitive readily available bedside test of respiratory muscle reserve in neurotoxic envenomation. Inability to reach 20 indicates reduced vital capacity and imminent respiratory muscle failure. SpO2 falls late — by the time SpO2 drops, respiratory failure is already advanced and the window for elective intubation may have closed. Ptosis and neck flexion weakness are important early signs of neuromuscular blockade but are not specific to respiratory failure. The count test integrates the function of the diaphragm, intercostals, and accessory muscles in a single, instantly repeatable bedside measurement.
CLINICAL PEARL
Two clinical traps in snakebite evaluation deserve special emphasis. First: the 20WBCT must be performed in a clean, dry GLASS tube — not a plastic tube or a serum separator tube. Glass contact activation is essential for the clotting reaction; a plastic tube gives a false-negative result and may cause you to withhold antivenom from a defibrinated patient. This error has been documented in Indian hospitals where plastic collection tubes have become the default.
Second: do not be falsely reassured by a normal 20WBCT in the first hour after a viper bite. VICC develops progressively as venom is absorbed; a clot at 30 minutes post-bite does not mean there will be a clot at 2 hours. The 20WBCT must be repeated every 30–60 minutes during the first 3–6 hours of observation. A patient who clots at 1 hour but does not clot at 2 hours has developed VICC in the interval and requires antivenom immediately. Write this on the observation chart as a timed instruction: 'Repeat 20WBCT at [time]'.