Page 1 of 20
IM21.1-3 | Snake Bite Foundations and Field Care — SDL Guide
Learning Objectives
- Enumerate the four medically significant ('big four') Indian snakes and describe their distinguishing morphological features
- Explain the pathophysiological mechanisms of haematotoxic (viper) and neurotoxic (elapid) envenomation
- Demonstrate and teach correct field first aid for snakebite, including indications for pressure immobilisation bandage
- List the harmful first-aid practices (tourniquet, incision-suction) and explain why they must be avoided
- Describe the systematic ABCDE-based hospital stabilisation approach for the snakebite patient
INSTRUCTIONS
Snakebite is a medical emergency and a public health crisis in rural India. This module builds your foundational knowledge of the big four venomous snakes, their envenomation syndromes, and the evidence-based field and hospital response. Mastery of this module prepares you to manage acute snakebite, teach community first aid, and prevent the iatrogenic harm caused by harmful traditional remedies.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 457 — Venomous Snakebites (textbook)
- API Textbook of Medicine, 10th ed. — Chapter on Envenomation (textbook)
- WHO Guidelines for the Management of Snakebites in South-East Asia, 2nd ed., 2016 (guideline)
- National Snakebite Management Protocol, Govt. of India, Ministry of Health and Family Welfare, 2008 (revised) (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 35-year-old farm labourer is brought to the primary health centre thirty minutes after being bitten on the left ankle while harvesting rice in a paddy field at dusk. The field worker who accompanies him has tied a tight tourniquet above the knee and made two parallel incisions over the bite wound, which is now bleeding freely. The patient is anxious and his ankle is swollen, but he is conscious and able to speak. There are two puncture marks about 8 mm apart. By the time you see him forty-five minutes later, he has developed oozing from his venepuncture site and his gum margins are bleeding. You notice the snake was killed and brought in — it is brownish, about 80 cm long, with a triangular head, elliptical pupils, and a pattern of dark dorsal blotches with pale centres. The tourniquet has already caused venous congestion and the incisions have created an open wound. What did the first responders do wrong — and what should you do now to prevent further harm and prepare for definitive treatment?
WHY THIS MATTERS
India carries one of the highest snakebite burdens in the world. An estimated 46,000 to 58,000 deaths occur annually from snakebite in India, making it a public health emergency rather than a rare event. The vast majority of victims are agricultural workers, rural poor, and tribal populations bitten during farming activities, which means the average final-year medical student on a rural posting or internship is very likely to encounter snakebite before encountering many other conditions studied in textbooks. The 'big four' venomous snakes of India — Russell's viper, saw-scaled viper, Indian cobra, and common krait — account for nearly all medically significant bites. NMC competencies IM21.1–21.3 require you to identify these species, perform correct first aid, and stabilise the patient — skills that save lives in the field before antivenom is available. Knowing what NOT to do (tourniquets, incisions, suction) is as important as knowing what to do.
RECALL
Activate prior knowledge before reading further. Recall the coagulation cascade: the intrinsic pathway (factors XII, XI, IX, VIII) and the extrinsic pathway (tissue factor, factor VII) converge on factor X, leading to thrombin generation and fibrin clot formation. Viper venoms disrupt this cascade at multiple points, causing consumption coagulopathy. Recall also the neuromuscular junction: acetylcholine is released from the presynaptic terminal, crosses the synaptic cleft, and binds nicotinic receptors on the motor end-plate to trigger muscle contraction. Krait venom blocks this signal presynaptically; cobra venom blocks it postsynaptically. Finally, recall basic wound care: tourniquets applied proximally to a limb cause venous and arterial occlusion — they do not prevent systemic envenomation once venom has entered the lymphatics and bloodstream, but they do cause ischaemia, compartment syndrome, and tissue necrosis when left in place for more than a few minutes.
The Big Four: Identification and Envenomation Syndromes
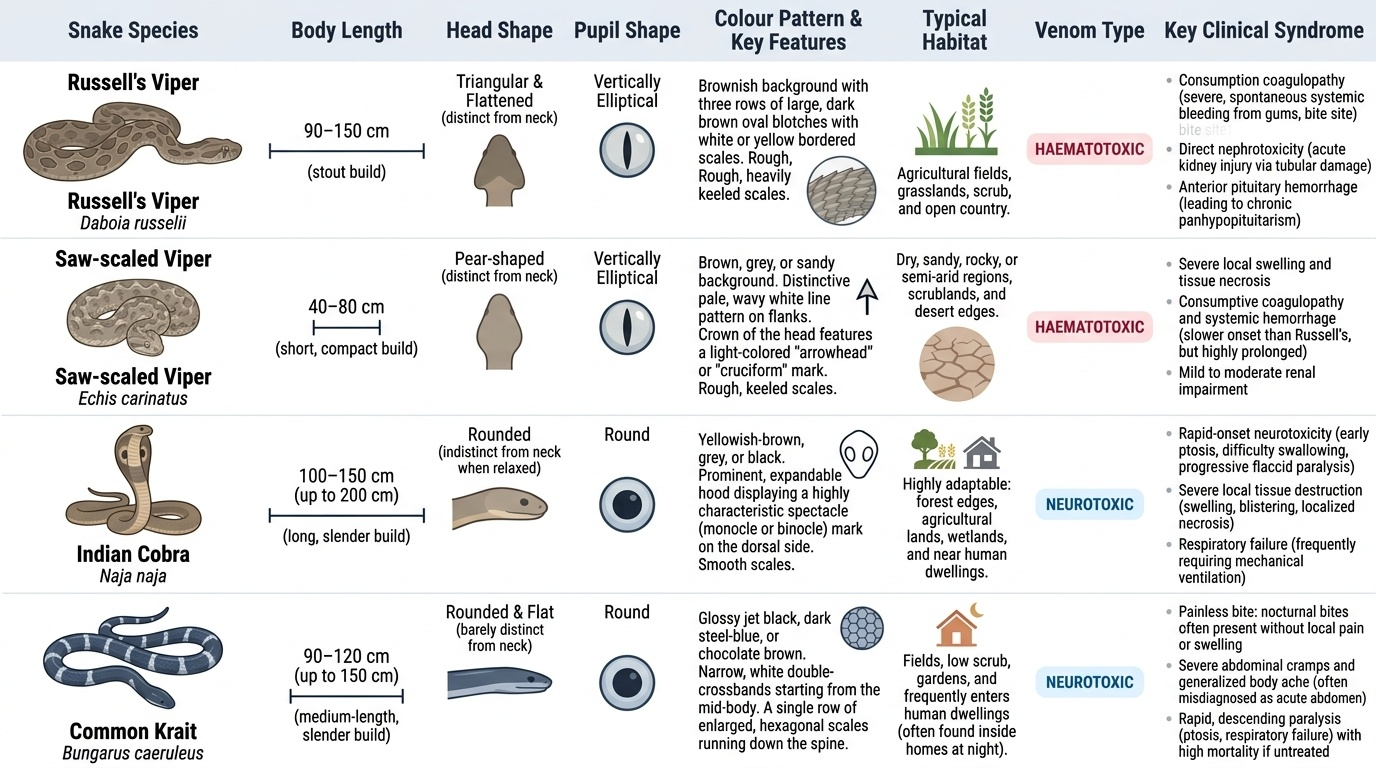
India's medically significant snakebite burden is overwhelmingly accounted for by four species, collectively called the 'big four'. Accurate identification shapes every subsequent clinical decision — which syndrome to anticipate, what investigations to order, and whether to use antivenom. While definitive species identification is often impossible in the field, a working knowledge of their distinguishing features and the syndrome they produce allows the clinician to manage envenomation rationally even when the snake is not available for inspection. The syndrome itself is diagnostic: haematotoxic envenomation (bleeding, coagulopathy, local tissue destruction) points to a viper; neurotoxic envenomation (ptosis, progressive paralysis, respiratory failure) points to an elapid (cobra or krait). Mixed presentations occur.
Provided image
Russell's viper (Daboia russelii) is responsible for the greatest number of snakebite deaths in India. It is a stout, heavy-bodied snake, 90–150 cm long, with a distinctive pattern of three rows of large, dark brown oval blotches with white or yellow borders on a brownish background. The head is triangular, flattened, and clearly distinct from the neck; the pupils are vertically elliptical. The body is rough-scaled. Russell's viper is found throughout the Indian subcontinent in agricultural fields, grasslands, and scrub. Its venom is predominantly haematotoxic: it contains procoagulant enzymes (Russell's viper venom phospholipase A2, a direct prothrombin activator, ecarin-like serine proteases) that trigger a consumption coagulopathy — the clotting factors are consumed in a futile activation cascade, leaving the patient unable to clot. The result is spontaneous bleeding from multiple sites. Additionally, Russell's viper venom causes direct nephrotoxicity (acute kidney injury via tubular cell damage and glomerular injury) and, in some Indian subpopulations, an unusual anterior pituitary haemorrhage that can cause panhypopituitarism — a late complication not seen with other Indian vipers.
Saw-scaled viper (Echis carinatus) is the smallest of the big four, typically 40–80 cm, with a pear-shaped head and a distinctive rough, keeled scales that produce a rasping hissing sound when the snake rubs its coils together ('saw-scaled'). It has a pattern of brown or grey scales with white dorsal blotches and pale lateral spots; a pale arrowhead marking is often visible on the top of the head. It is found in dry, stony, and sandy habitats across India, Pakistan, and the Middle East. Despite its small size, it delivers a strongly haematotoxic venom with phospholipase A2 and haemotoxic enzymes that produce coagulopathy, thrombocytopenia, and local tissue necrosis. It is reputedly responsible for more snakebite deaths in Africa and South Asia combined than any other snake.
Indian cobra (Naja naja) is the iconic hooded snake of South Asia, 120–180 cm, with a rounded head, round pupils, and smooth scales. Its most recognisable feature is the ability to spread its cervical ribs to form a 'hood' when threatened; the dorsal surface of the hood often bears a binocular spectacle mark (two circles joined by a bridge) in some subspecies, though not all Indian cobras show this clearly. Colour varies widely — from pale grey to black, with or without banding. The cobra is a predominantly neurotoxic snake: its venom contains post-synaptic alpha-neurotoxins that bind irreversibly to nicotinic acetylcholine receptors at the motor end-plate, blocking neuromuscular transmission. Clinically this causes descending flaccid paralysis — first ptosis (drooping eyelids), then ophthalmoplegia, then bulbar palsy (dysphagia, dysphonia), and finally respiratory muscle paralysis. Cobra venom also has significant cytotoxic components that cause severe local tissue necrosis, making cobra bite one of the most destructive local wounds among the big four.
Common krait (Bungarus caeruleus) is 90–175 cm, slender, with a smooth shiny appearance, a narrow head barely distinct from the neck, round pupils, and a characteristic pattern of white crossbands (or paired white spots) on a glossy blue-black or dark background. The scales are smooth and highly polished — the dorsal mid-body row is enlarged and hexagonal, giving a ridge-like appearance along the spine. Kraits are nocturnal and frequently bite sleeping victims in rural households — a victim may not even feel the bite (the krait bite is often painless or minimally painful) and may present with progressive paralysis of unclear onset. The krait venom is pre-synaptic neurotoxic: beta-bungarotoxin irreversibly destroys the presynaptic terminal and prevents acetylcholine vesicle release, causing a flaccid paralysis that is typically more complete and more difficult to reverse with anticholinesterase drugs than cobra envenomation. The absence of pain and minimal local reaction makes krait envenomation underdiagnosed and particularly dangerous — a patient may be sleeping and not be brought to attention until respiratory failure is imminent.
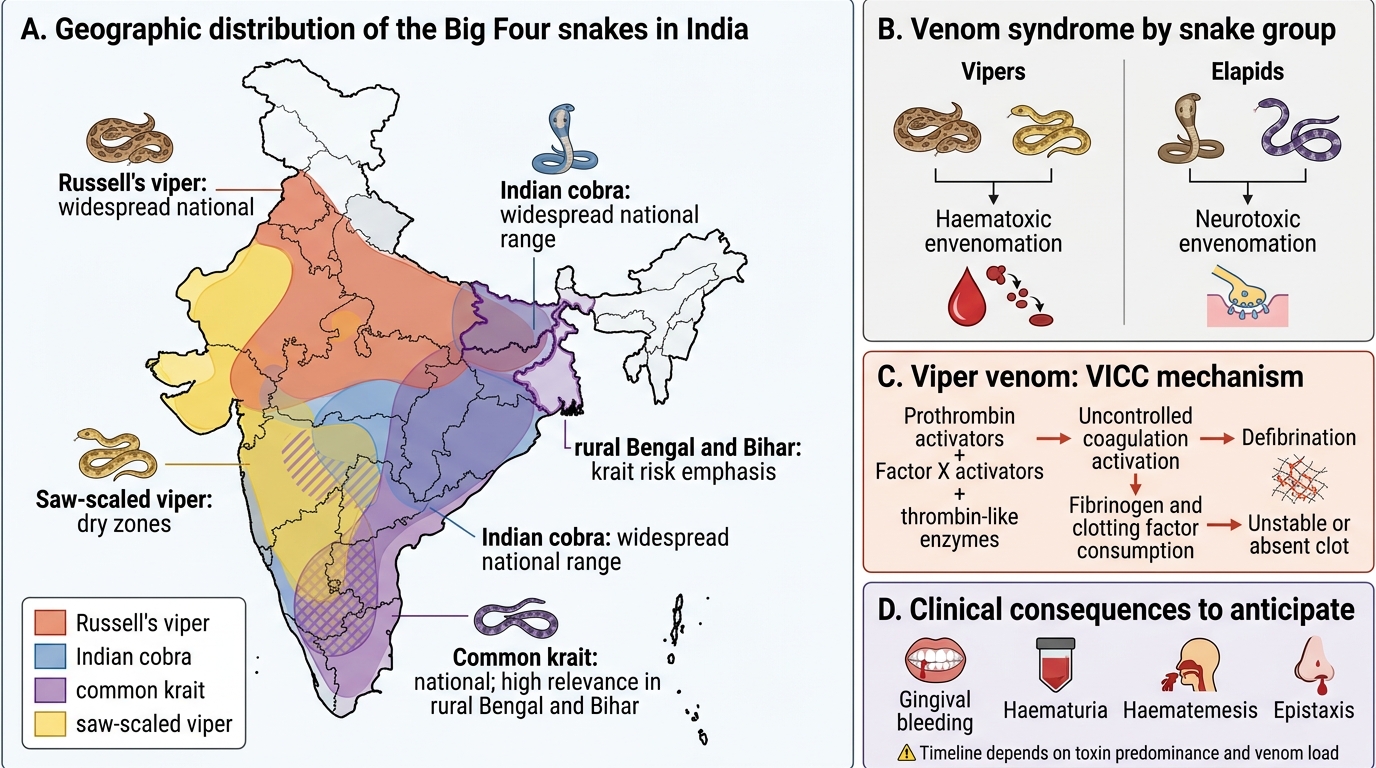
Big Four Snake Distribution and Envenomation Syndromes in India
Pathophysiology of Envenomation Syndromes
Understanding the molecular mechanisms of venom toxicity is essential for logical clinical management and for anticipating the timeline of complications. Snake venoms are complex biological mixtures containing 20–100 distinct proteins with enzymatic or structural toxin functions; the clinical syndrome depends on which toxin classes predominate in the venom of the offending species. The two principal syndromes in India are haematotoxic envenomation (caused by vipers) and neurotoxic envenomation (caused by elapids), though cytotoxic and nephrotoxic components contribute to both.
In haematotoxic envenomation from Russell's viper and saw-scaled viper, the key mechanism is venom-induced consumption coagulopathy (VICC). Viper venoms contain prothrombin activators, factor X activators, and thrombin-like enzymes that trigger uncontrolled systemic activation of the coagulation cascade. This consumes fibrinogen and clotting factors faster than they can be replenished, leaving the patient in a state of defibrination — the blood contains negligible functional clotting factors and cannot form a stable clot. Clinically this manifests as spontaneous bleeding from multiple sites: gingival bleeding, haematuria, haematemesis, epistaxis, intracranial haemorrhage in severe cases. Phospholipase A2 in viper venom also causes direct cell membrane disruption, leading to local tissue necrosis at the bite site, myonecrosis (elevated CK, myoglobinuria), and haemolysis. The combination of haemolysis, direct tubular toxicity, and haemoglobin cast formation causes acute kidney injury (AKI) — one of the major causes of death from Russell's viper bite in India.
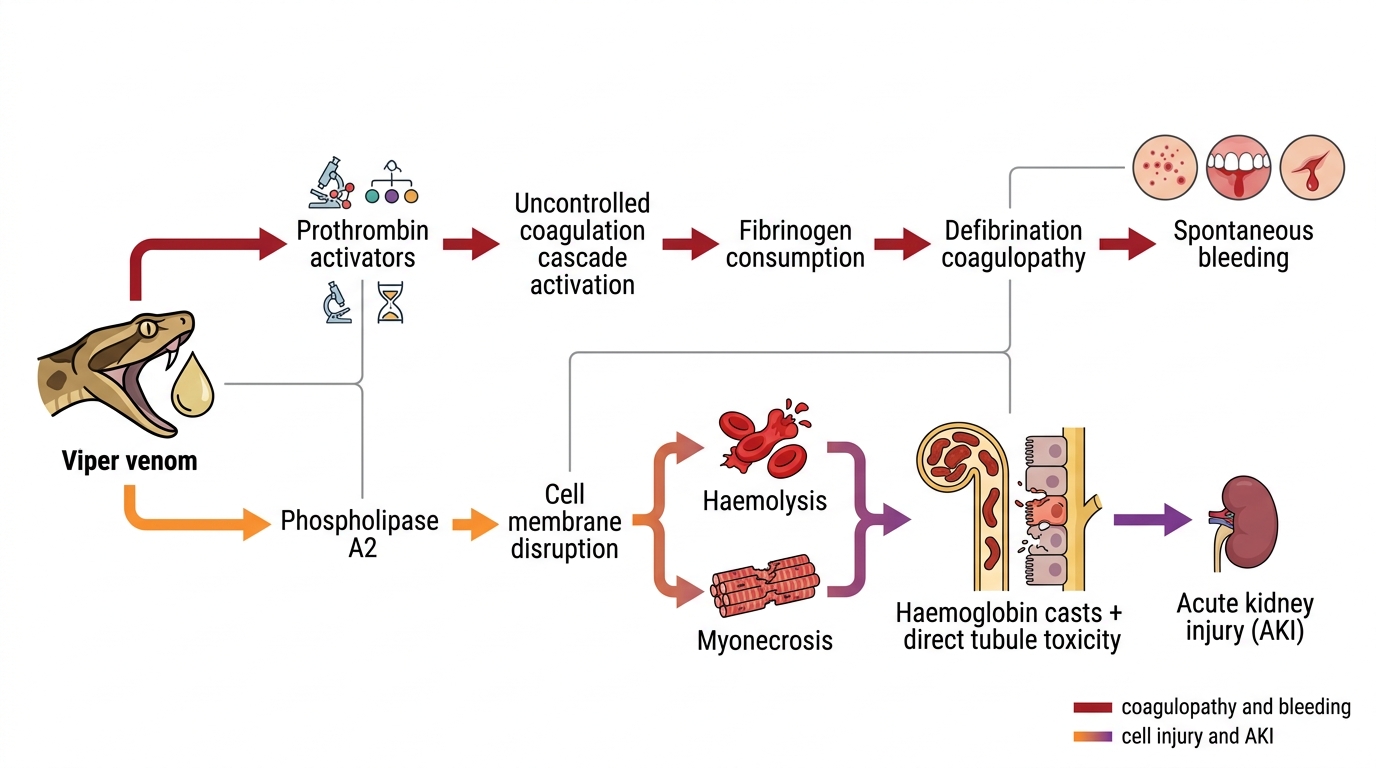
Mechanism of Haematotoxic Viper Envenomation
In neurotoxic envenomation from cobra and krait, the mechanism targets the neuromuscular junction (NMJ). The cobra's post-synaptic alpha-neurotoxins bind with very high affinity to the nicotinic acetylcholine receptor (nAChR) on the muscle end-plate, competitively blocking acetylcholine binding and preventing muscle depolarisation. Because the block is at the post-synaptic receptor, some residual response to acetylcholine accumulation (via anticholinesterase drugs) is theoretically possible. In contrast, the krait's pre-synaptic beta-bungarotoxin irreversibly destroys the presynaptic terminal vesicle-docking apparatus, preventing acetylcholine release entirely — this block cannot be reversed pharmacologically and paralysis persists until new presynaptic terminals regenerate, which may take weeks. Clinically, both produce a descending flaccid paralysis beginning with ptosis (the most sensitive early sign), then ophthalmoplegia, bulbar palsy (nasal voice, difficulty swallowing, pooling of secretions), and finally respiratory muscle paralysis that is fatal without ventilatory support.
SELF-CHECK
A 28-year-old farmer is bitten on the hand at night while sleeping. He reports no pain at the bite site and no local swelling. Six hours later he develops ptosis and difficulty swallowing. Which snake is most likely responsible, and why is the paralysis particularly difficult to reverse?
A. Indian cobra — post-synaptic alpha-neurotoxin blocks nAChR; partially reversible with neostigmine
B. Russell's viper — phospholipase A2 destroys motor end-plates; irreversible
C. Common krait — pre-synaptic beta-bungarotoxin destroys presynaptic terminals; cannot be reversed pharmacologically
D. Saw-scaled viper — haemotoxin causes neuronal ischaemia; treatable with antivenom alone
Reveal Answer
Answer: C. Common krait — pre-synaptic beta-bungarotoxin destroys presynaptic terminals; cannot be reversed pharmacologically
The painless nocturnal bite with absent local reaction followed by descending paralysis is the classic presentation of common krait envenomation. Krait venom's beta-bungarotoxin acts pre-synaptically, destroying the vesicle release machinery — acetylcholine cannot be released regardless of how much anticholinesterase is given. This contrasts with cobra envenomation (post-synaptic block, some partial reversal with neostigmine + atropine may be tried). Krait paralysis requires prolonged ventilatory support until presynaptic regeneration occurs. Russell's viper causes haematotoxic envenomation, not primary neurotoxicity.
Initial Field Management and First Aid
Correct first aid in the field can prevent iatrogenic harm and buy time for transfer to a hospital with antivenom. The evidence base for snakebite first aid is clear: the commonly practised interventions of tourniquet application, incision-and-suction, and electric shock are all harmful and must be actively taught against. The WHO snakebite management guidelines and the Indian National Snakebite Protocol emphasise a 'do less, do it safely, move fast' approach in the field.
What TO do (evidence-based first aid):
The following five steps should be taught to every community health worker, ASHA, and rural schoolteacher in high-risk agricultural areas. They are simple, free, and require no equipment. Their purpose is to prevent iatrogenic harm, slow venom absorption, and get the patient to antivenom as rapidly as possible — the only proven life-saving intervention. Each step has a specific physiological rationale that makes it memorable and teachable. Carry this list mentally into every rural posting.
- Reassure the patient and keep them calm and still. Movement accelerates lymphatic spread of venom (venom travels primarily via lymphatics, not veins); immobilisation slows systemic absorption. Panic increases heart rate and cardiac output, which also accelerates distribution.
- Immobilise the bitten limb below the level of the heart. Apply a loose, supportive splint if possible — like a fracture splint, not a compression bandage. The limb should be positioned at or slightly below heart level to reduce lymphatic flow without obstructing arterial inflow.
- Pressure immobilisation bandage (PIB) is recommended ONLY for neurotoxic elapid bites (cobra, krait) where systemic effects are the primary risk. A firm crepe bandage is applied from the bite site distally upward, covering the entire limb like a pressure bandage for a sprain — firm enough to impede lymphatic flow but not so tight as to cut off arterial pulse. This technique, validated for Australian elapids, reduces systemic absorption but should NOT be used for viper bites (haematotoxic) because it concentrates the locally destructive venom and worsens tissue necrosis.
- Remove any constrictive items — rings, bracelets, watches, tight clothing — from the bitten extremity before swelling renders them impossible to remove and causes distal ischaemia.
- Transfer immediately to the nearest hospital with antivenom. Note the time of the bite, the snake description if possible, and document any symptoms that develop en route.
⚑ AI image — pending faculty review (auto-QA score 7/10; best of 3 attempts)
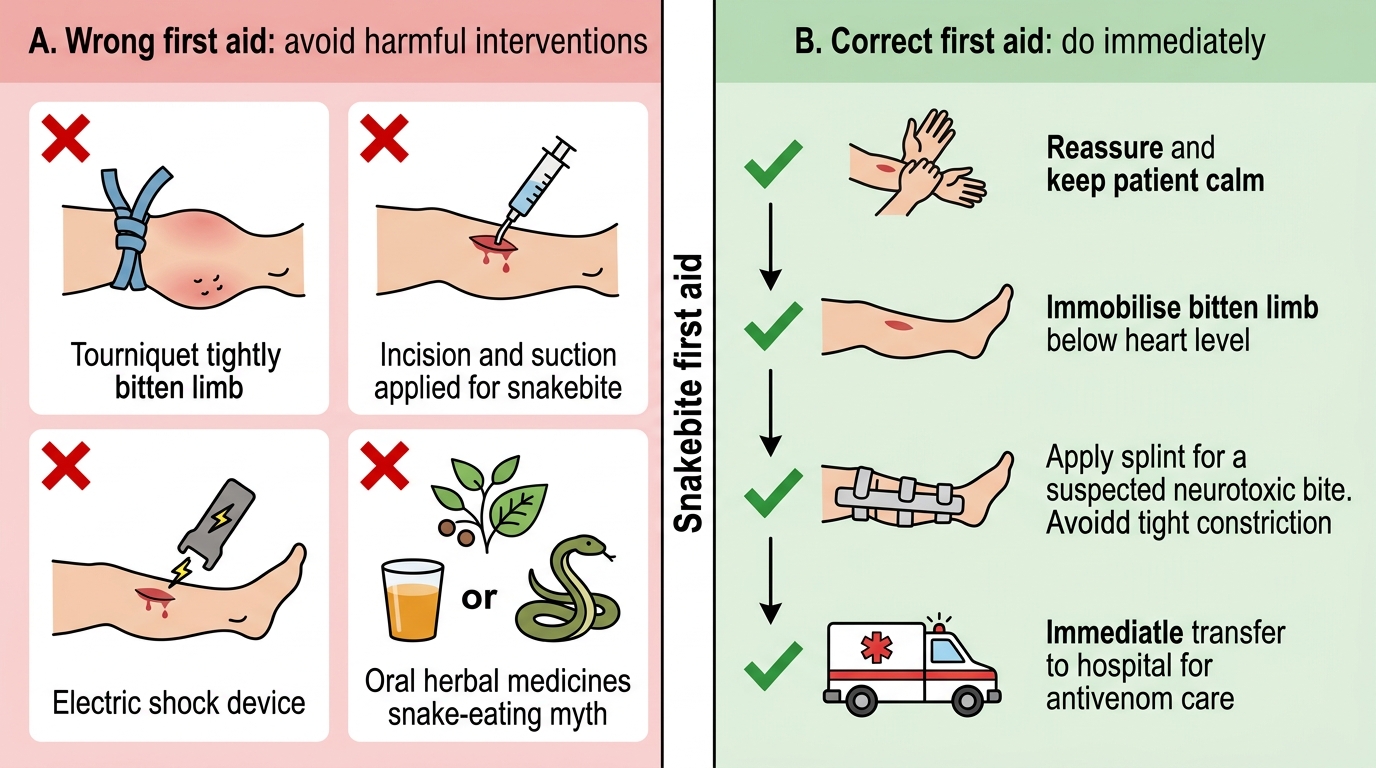
Snakebite First Aid: What to Avoid and What to Do
What NOT to do (harmful interventions to actively avoid):
- Tourniquets: A constricting tourniquet does not prevent systemic envenomation — venom enters the lymphatics rapidly and is already partially absorbed before a tourniquet can be applied. What a tourniquet does accomplish is to trap concentrated venom in a distal ischaemic limb, accelerating local tissue necrosis and causing compartment syndrome. Prolonged tourniquets (>30 minutes) cause irreversible ischaemic damage. If a tourniquet is already in place on arrival, do NOT release it abruptly — gradually release it over 5–10 minutes while monitoring for sudden cardiovascular decompensation from abrupt venom redistribution.
- Incision and suction: Making incisions over the bite wound and applying oral suction or mechanical suction devices does not remove meaningful amounts of venom (which is already in the tissue and lymphatics within seconds), and creates an open contaminated wound that worsens local infection risk and promotes secondary haemorrhage in coagulopathic patients.
- Oral herbal medicines, eating the snake, or drinking alcohol: All are ineffective and waste time better spent on transfer.
- Electric shock treatments: No evidence of benefit; risk of electrocution.