Page 2 of 20
IM21.1-3 | Snake Bite Foundations and Field Care — SDL Guide (Part 2)
Hospital Stabilisation of the Snakebite Patient
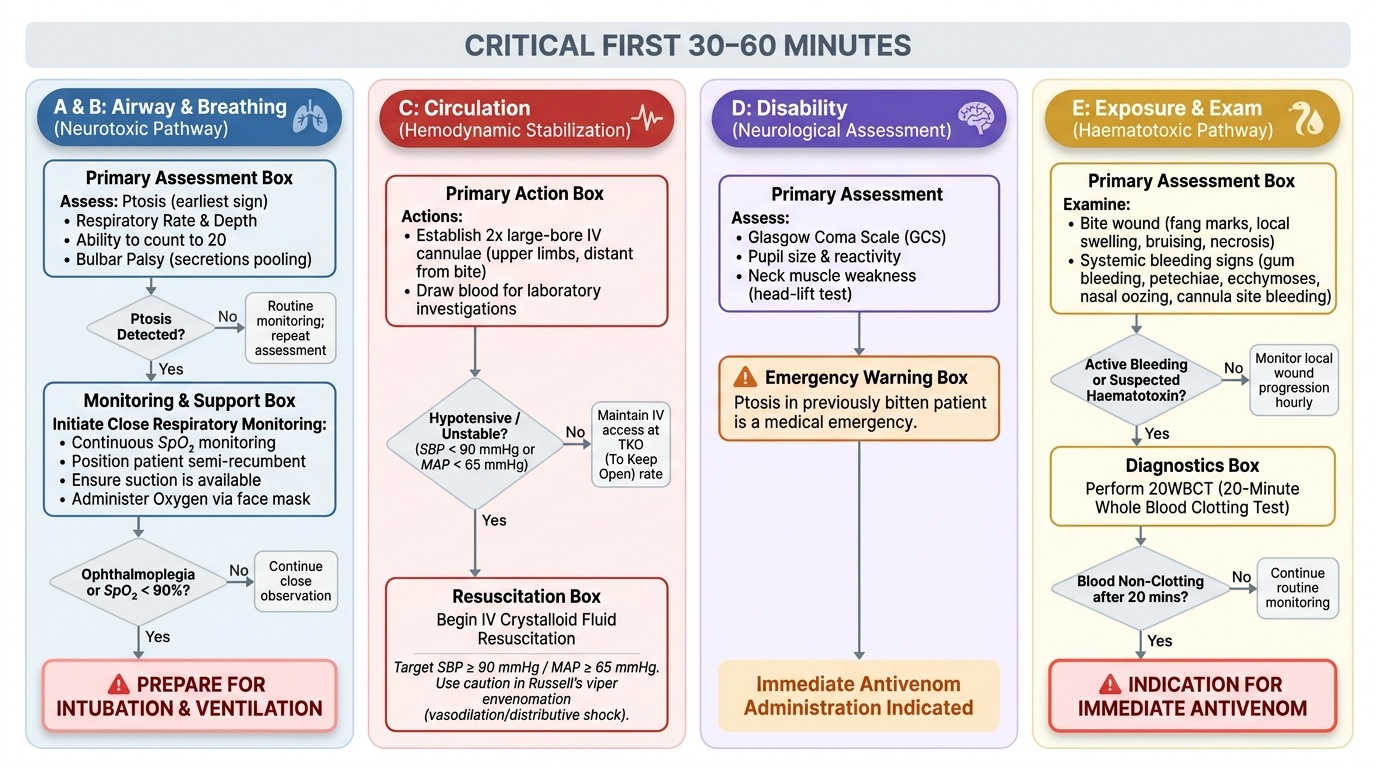
On arrival at hospital, the snakebite patient requires a rapid, structured approach that simultaneously assesses the severity of envenomation, addresses immediate life threats, and prepares for antivenom administration. The clinical approach mirrors the ABCDE primary survey, with specific additions for envenomation syndromes. The first 30–60 minutes are critical: systemic envenomation can evolve rapidly, and delays in antivenom administration worsen outcome.
Provided image
A — Airway and B — Breathing: The primary concern in neurotoxic envenomation is respiratory muscle paralysis. Ptosis is the earliest and most sensitive sign; its appearance mandates close respiratory monitoring. Assess respiratory rate, depth, and ability to sustain phonation (ask the patient to count aloud to 20; inability to complete without shortness of breath suggests impending respiratory failure). Bulbar palsy causes pooling of secretions and risk of aspiration. Position the patient semi-recumbent, have suction available, and prepare for intubation if ptosis progresses to ophthalmoplegia or oxygen saturation falls. Oxygen via face mask should be started in any patient with neurotoxic signs.
C — Circulation: Establish two large-bore IV cannulae in both upper limbs (or sites distant from the bite). Draw blood at the time of cannulation for investigations (see below). Begin IV crystalloid fluid resuscitation if the patient is hypotensive or haemodynamically unstable — Russell's viper envenomation can cause profound hypotension through direct vasodilation, autonomic effects, and distributive shock. A target blood pressure of ≥90 mmHg systolic (or MAP ≥65 mmHg) should guide the rate of infusion.
D — Disability (Neurological Assessment): Assess consciousness (GCS), pupil size and reactivity, and presence of ptosis. Ptosis in a previously bitten patient is a medical emergency demanding immediate antivenom administration. Check for neck muscle weakness (ask the patient to lift their head off the pillow against resistance). Document the development of any symptoms since the bite — the timeline informs the rate of progression and urgency.
E — Exposure and Examination: Examine the bite wound (number of fang marks, local swelling, bruising, necrosis), and look for systemic bleeding signs: gum bleeding, petechiae, ecchymoses, nasal oozing, blood at cannula sites. The appearance of spontaneous systemic bleeding or failure of blood to clot at the venepuncture site is a haematotoxic envenomation emergency.
Investigations to order immediately:
1. 20-minute whole-blood clotting test (20WBCT) — the single most important bedside test in snakebite (detailed in the next module)
2. Complete blood count, peripheral blood smear (haemolysis, thrombocytopenia)
3. Coagulation studies: PT, aPTT, INR, fibrinogen, D-dimer
4. Renal function: serum creatinine, urea, electrolytes (for AKI monitoring)
5. Serum CK and urine for myoglobin (myonecrosis from viper venom)
6. Urine dipstick for blood (haematuria or myoglobinuria)
7. ECG (scorpion and some snake venoms affect cardiac conduction)
All patients with suspected venomous snakebite should be monitored for at least 24 hours even if initially asymptomatic — some envenomations, particularly krait bites, have a delayed onset of paralysis of 4–12 hours after a painless bite.
SELF-CHECK
A patient arrives 20 minutes after a snakebite with a constricting tourniquet applied above the bite on the right leg. On examination the foot is cold and cyanotic. The correct approach to the tourniquet is:
A. Remove it immediately in one step to restore circulation
B. Leave it in place until antivenom has been administered
C. Gradually release it over 5–10 minutes while monitoring vital signs and preparing for antivenom
D. Replace it with a pressure immobilisation bandage before releasing
Reveal Answer
Answer: C. Gradually release it over 5–10 minutes while monitoring vital signs and preparing for antivenom
Abrupt tourniquet release after prolonged application can cause a sudden flood of concentrated venom into the systemic circulation, precipitating cardiovascular collapse. The correct approach is to gradually loosen the tourniquet over 5–10 minutes while closely monitoring blood pressure and pulse, with IV access established and antivenom ready. Leaving the tourniquet in place causes progressive ischaemia and is not appropriate. Replacing it with a PIB is also incorrect — PIB is only recommended for neurotoxic elapid bites and should not substitute for removing a dangerous constricting tourniquet.
Self-Assessment: Species, Syndromes, and Field Care
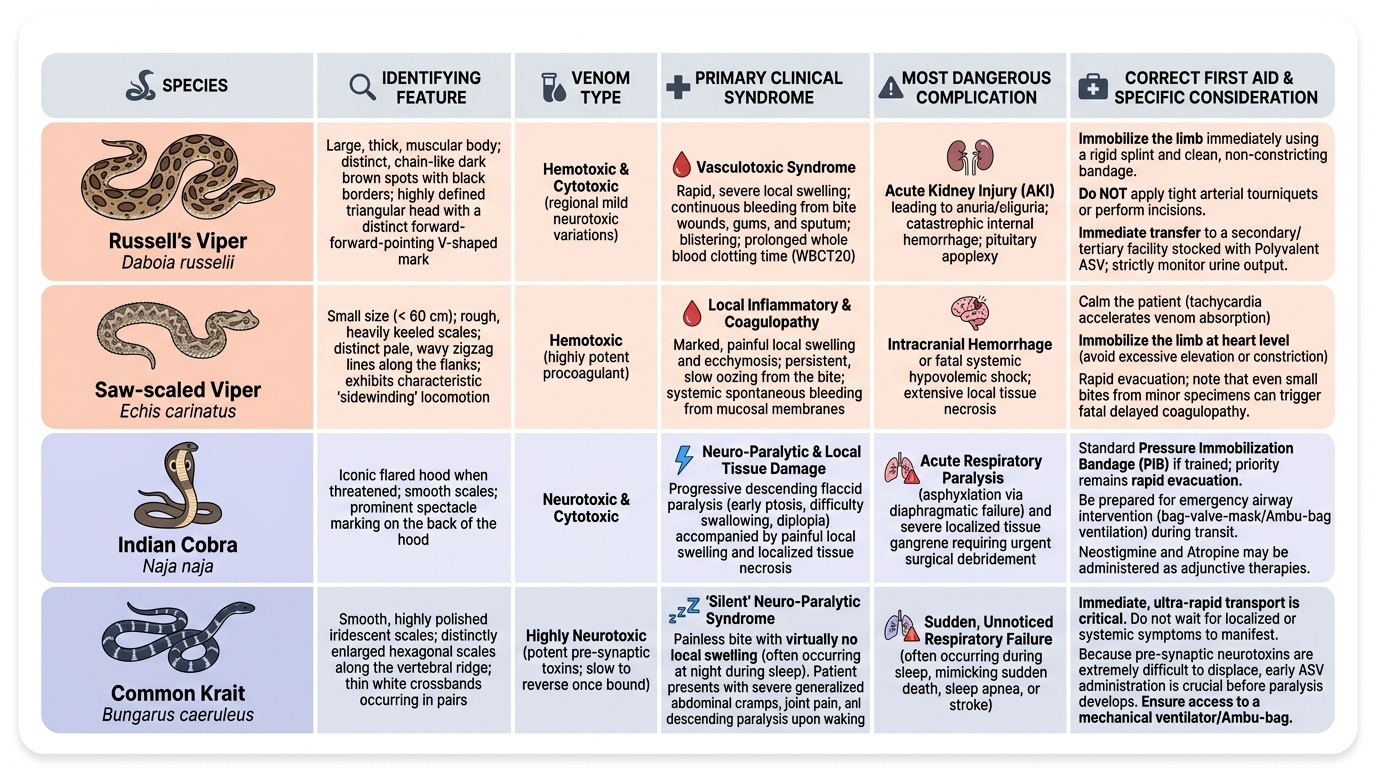
This self-assessment section consolidates your ability to link species identification features to the envenomation syndrome and to apply the correct first-aid principles in a field scenario. The competencies IM21.1–21.3 require you to enumerate local poisonous snakes, demonstrate correct initial management in a field setting, and describe the initial stabilisation approach at hospital — skills that are tested not only in the NMC examination but in the very first weeks of internship postings in rural India. Working through these clinical scenarios is the single most effective way to cement the pattern-recognition logic you need: species morphology → predicted syndrome → correct triage action. For each scenario below, resist the urge to read the analysis first — form your own clinical impression, name the species, predict the syndrome, and decide the immediate priority before confirming your answer. This mimics the real clinical encounter where there is no answer key and the patient's life depends on rapid correct reasoning. The reference table below anchors your self-check.
Provided image
Scenario A: A 22-year-old tribesman is brought by his family at 8 PM. He was working in a paddy field and was bitten an hour ago on the right calf. The snake was killed — it is about 45 cm, with rough keeled scales, a pear-shaped head, and brown-grey colouring with white dorsal blotches. He has two fang marks on his calf, swelling extending to the knee, and his gum margins are oozing blood. His relatives have applied a tight rope tourniquet above the knee. What species, what syndrome, and what is the priority first action?
Analysis: The small size, rough keeled scales, pear-shaped head, and dry habitat point to a saw-scaled viper. The gingival bleeding is consistent with haematotoxic envenomation. The priority is to gradually release the tourniquet over 5–10 minutes with IV access established, perform the 20WBCT to quantify coagulopathy, and administer polyvalent antivenom when the indication is confirmed.
Scenario B: A 50-year-old man is found at 6 AM by family members lying on his sleeping mat with drooping eyelids and difficulty speaking. He denies being bitten but shows a small wound on his foot consistent with a puncture mark. He cannot lift his head. Respiratory rate is 22/min. What is the likely diagnosis and immediate priority?
Analysis: Painless nocturnal bite, descending paralysis (ptosis, bulbar palsy, neck weakness), no local swelling — this is a common krait bite. Immediate priority: oxygen, IV access, prepare for intubation (progressive respiratory paralysis is expected), administer polyvalent antivenom. Ventilatory support will likely be required for days to weeks — warn the family and arrange ICU transfer.
SELF-CHECK
Which of the following field interventions is evidence-based and recommended for a suspected cobra bite (neurotoxic envenomation)?
A. Tight tourniquet above the bite to prevent venom spread
B. Incision and oral suction of the bite wound
C. Firm pressure immobilisation bandage covering the entire limb, combined with splinting and immediate transfer
D. Ice pack application to the bite site to slow venom absorption
Reveal Answer
Answer: C. Firm pressure immobilisation bandage covering the entire limb, combined with splinting and immediate transfer
Pressure immobilisation bandage (PIB) — a firm, even compression bandage applied from the bite distally upward — is recommended for neurotoxic elapid bites (cobra, krait) to slow lymphatic uptake of venom. It must be combined with splinting to minimise limb movement and followed by immediate transfer. PIB is NOT recommended for viper bites (haematotoxic) as it concentrates locally destructive venom and worsens tissue necrosis. Tourniquets, incision-suction, and ice are all contraindicated.
CLINICAL PEARL
The most dangerous misconception in snakebite first aid is that a tourniquet prevents envenomation. Venom enters the lymphatic system within seconds to minutes of injection — it has already disseminated into the lymphatics long before any tourniquet can be applied. The tourniquet adds zero protection against systemic envenomation but reliably causes ischaemia, compartment syndrome, and limb loss if left in place. In India, tourniquet-related limb amputations from snakebite are well-documented. Teach this clearly: the correct field treatment is immobilisation of the limb (not the blood supply), reassurance, and rapid transfer.
A second pearl: the common krait (Bungarus caeruleus) bites sleeping victims at night in rural homes, and the bite is painless. Patients may be brought in with progressive paralysis of unclear onset, no visible bite site (kraits have small fangs), and no clear history. Consider krait envenomation in any rural patient with unexplained descending flaccid paralysis, especially if the family reports the patient sleeping in a house with rodent activity.