Page 8 of 27
IM22.4 | Drug Overdose — SDL Guide (Part 2)
Management of Drug Overdose: Antidotes and Supportive Care
Management of drug overdose is built on the same platform as all acute poisoning — ABC stabilisation first, then toxin-specific therapy. What distinguishes drug overdose management from general poisoning is the availability of specific antidotes for several of the most common agents, and the well-validated, evidence-based protocols that govern their use. The clinician who knows the specific management protocol for each agent — including the precise antidote, dose, monitoring parameters, and pitfalls — can convert a potentially fatal overdose into a survivable emergency.
Provided image
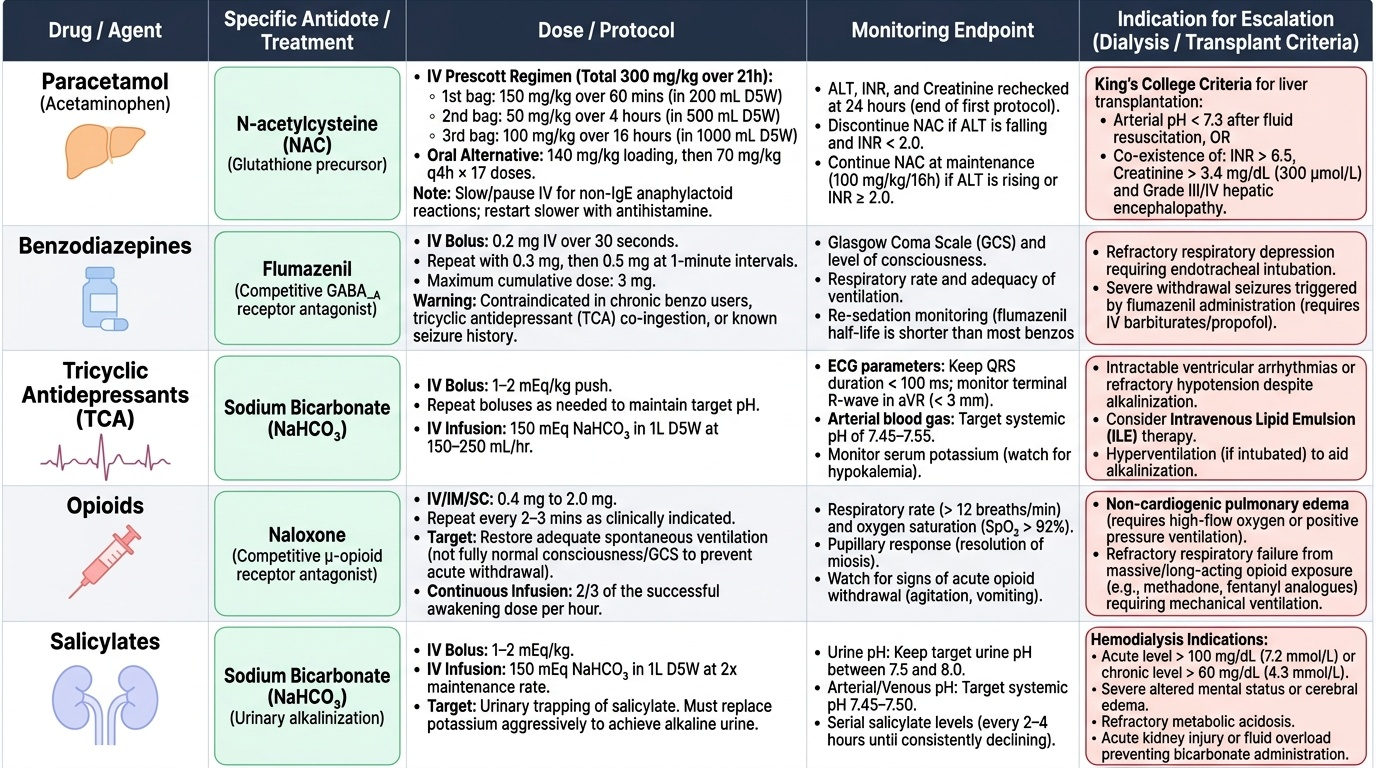
Paracetamol overdose — N-acetylcysteine (NAC):
NAC is a glutathione precursor (and directly substitutes for glutathione) that neutralises NAPQI. It is dramatically effective if started within 8 hours of ingestion (near-complete prevention of hepatic failure in those treated within 8 hours); moderately effective up to 24 hours (reduces severity even after hepatic injury is established); and may still have benefit even in established acute liver failure (by mechanisms beyond glutathione replenishment — including improving hepatic microcirculation and mitochondrial function). There is therefore no strict upper time limit for NAC initiation in paracetamol overdose — start it whenever the nomogram indicates treatment or when staggered/uncertain ingestion is clinically concerning.
Standard IV NAC protocol (Prescott regimen):
- 150 mg/kg over 60 minutes (loading dose in 200 mL 5% dextrose)
- 50 mg/kg over 4 hours (second bag in 500 mL 5% dextrose)
- 100 mg/kg over 16 hours (third bag in 1000 mL 5% dextrose)
Total dose = 300 mg/kg over 21 hours. Oral NAC (140 mg/kg loading dose, then 70 mg/kg every 4 hours × 17 doses) is an alternative when IV access is unavailable. The most common adverse reaction to IV NAC is anaphylactoid reaction (flushing, urticaria, bronchospasm) — managed by slowing or temporarily stopping the infusion and giving antihistamine; this is NOT a true allergy (not IgE-mediated) and NAC can be restarted at a slower rate.
Monitoring after NAC completion: Recheck ALT, INR, creatinine at 24 hours after completing the 21-hour course. If ALT is falling and INR < 2 — NAC is not required further. If ALT is rising or INR > 2 after the first course — continue NAC at the maintenance dose (100 mg/kg/16 hours) and reassess. King's College Criteria for liver transplant referral in paracetamol-induced ALF: pH < 7.3 (after resuscitation) OR the combination of INR > 6.5, creatinine > 300 mcmol/L (3.4 mg/dL), AND Grade 3–4 encephalopathy — all three must be present simultaneously.
TCA overdose — Sodium bicarbonate:
IV sodium bicarbonate 1–2 mEq/kg (50–100 mEq) bolus is indicated for: QRS > 100 ms, ventricular arrhythmias, hypotension not responding to fluids. Target serum pH 7.45–7.55 (mild alkalosis). The mechanism is: alkalinisation increases the proportion of TCA in the ionised (positively charged) form, which cannot enter the sodium channel; and the elevated extracellular sodium competes with TCA for channel binding. Repeat boluses every 5–15 minutes as needed. Continuous bicarbonate infusion (3 × 50 mEq ampules in 1 L of 5% dextrose at twice maintenance rate) for persistent QRS widening. Benzodiazepines (diazepam or lorazepam) for seizures; physostigmine is contraindicated. Intubation if GCS falling.
BZD overdose — Flumazenil:
Flumazenil 0.2 mg IV, repeatable up to 1 mg total. Half-life 1 hour (shorter than most BZDs) — re-sedation is common, so observation and repeated doses or infusion may be required. Absolute contraindications: BZD dependence (acute withdrawal), co-ingested proconvulsants (TCA, cocaine — reversal of BZD sedation unmasks the seizure risk).
Opioid overdose — Naloxone:
Naloxone 0.4–2 mg IV/IM/intranasal; repeat every 2–3 minutes to a maximum of 10 mg. Titrate to restore adequate ventilation and protective airway reflexes — not to full wakefulness (risks acute opioid withdrawal in dependent patients: vomiting, agitation, acute lung injury). Infusion: 2/3 of the effective bolus per hour IV infusion — required for long-acting opioids (methadone, extended-release morphine) or tramadol.
Salicylate overdose — Urinary alkalinisation and haemodialysis:
Urinary alkalinisation: IV sodium bicarbonate to maintain urine pH 7.5–8.5 — ion trapping of ionised salicylate in the tubular lumen prevents renal reabsorption, dramatically increasing salicylate clearance. Maintain adequate hydration (IV fluids). Monitor serum potassium carefully — alkalinisation drives K into cells (hypokalaemia impairs urinary alkalinisation). Indications for haemodialysis: serum salicylate > 100 mg/dL; acute kidney injury; severe acidosis (pH < 7.2); CNS dysfunction (altered consciousness, seizures); pulmonary oedema. Activated charcoal 50 g if within 2 hours of ingestion; MDAC (multiple dose AC) for sustained-release aspirin preparations.
SELF-CHECK
A 35-year-old man is brought in unconscious after a deliberate overdose of amitriptyline (TCA). BP 70/40 mmHg, pulse 130 bpm. ECG shows sinus tachycardia with QRS duration of 140 ms. ABG: pH 7.28, HCO3 16 mEq/L (metabolic acidosis). What is the MOST appropriate immediate pharmacological intervention for his ECG findings?
A. IV flumazenil 0.2 mg
B. IV sodium bicarbonate 1-2 mEq/kg bolus
C. IV naloxone 0.4 mg
D. IV amiodarone 300 mg
Reveal Answer
Answer: B. IV sodium bicarbonate 1-2 mEq/kg bolus
QRS duration of 140 ms in TCA overdose indicates significant sodium channel blockade with high risk of ventricular arrhythmia and VF. The correct treatment is IV sodium bicarbonate (1-2 mEq/kg bolus), which alkalinises the blood (increasing the ionised fraction of TCA that cannot bind sodium channels) and provides extra sodium to compete for channel binding. The co-existing metabolic acidosis (pH 7.28) worsens sodium channel blockade, making bicarbonate doubly indicated. Flumazenil reverses benzodiazepines, not TCAs. Naloxone reverses opioids. Amiodarone is not first-line for TCA arrhythmia and may worsen QTc prolongation.
Self-Assessment: Drug Overdose Case Scenarios
The following scenarios test your ability to integrate drug overdose toxicology, clinical recognition, investigation interpretation, and specific treatment decisions. Work through each before reading the analysis, as this mirrors the KH-level skill required by NMC competency IM22.4 — applying overdose knowledge to patient care decisions.
Scenario A: A 16-year-old girl presents to casualty at 2 am, drowsy with slurred speech. Her parents found her in her room after a party, with an empty vodka bottle and an empty blister pack of diazepam 5 mg tablets (14 tablets = 70 mg total). GCS 11, RR 8/min, SpO₂ 92%, BP 100/60. Pupils 3 mm bilaterally, reactive. No TCA history. What is the toxidrome, immediate treatment, and should flumazenil be given?
Analysis: Sedative-hypnotic toxidrome — alcohol + benzodiazepine co-ingestion. RR 8, SpO₂ 92% indicate clinically significant respiratory depression. Immediate treatment: (1) Airway — place in recovery position; prepare for BVM ventilation; if GCS drops or SpO₂ worsens, intubate. (2) High-flow oxygen. (3) IV access; blood glucose (always). Flumazenil: CAUTION — co-ingestion with alcohol is common; flumazenil reverses BZD component but not alcohol. Given no evidence of TCA co-ingestion, flumazenil 0.2 mg IV can be given cautiously with monitoring; re-sedation will occur (flumazenil half-life 60 min vs diazepam 20–100 hours). Admit for observation. Psychiatric assessment when sober.
Scenario B: A 28-year-old man is brought in agitated, with tinnitus and confusion. His wife says he took a large number of aspirin tablets for a headache earlier in the day. Temperature 38.9°C, HR 118, RR 28/min. ABG: pH 7.48, PaCO₂ 26 mmHg, HCO₃ 18 mEq/L. Serum salicylate level: 75 mg/dL. Identify the acid-base status and outline management.
Analysis: The ABG shows mixed acid-base disorder — low PaCO₂ (respiratory alkalosis from salicylate-stimulated hyperventilation) + low bicarbonate (metabolic acidosis from uncoupled oxidative phosphorylation) with net pH 7.48 (alkalosis dominating at this stage). Salicylate level 75 mg/dL = moderate-severe toxicity. Management: (1) IV fluids (correct dehydration). (2) Urinary alkalinisation — IV sodium bicarbonate infusion targeting urine pH 7.5–8.5 with serum K monitoring. (3) Activated charcoal if within 2 hours; MDAC for sustained-release aspirin. (4) Monitor for deterioration — if pH falls below 7.2, consciousness deteriorates, or renal function worsens, haemodialysis is indicated (level 75 mg/dL is approaching the threshold for dialysis consideration in symptomatic patients). (5) Glucose monitoring and correction.
Scenario C: A 45-year-old man with a known history of HIV (on antiretrovirals including rifampicin for TB co-infection) is brought in after taking 10 paracetamol 500 mg tablets (5 g total). He is asymptomatic. His 4-hour paracetamol level is 80 mg/L, which plots BELOW the standard treatment line. Should NAC be withheld?
Analysis: NO — despite the level plotting below the standard treatment line, this patient has two major risk factors that dramatically lower the toxic threshold: (1) Rifampicin is a potent CYP2E1/CYP3A4 inducer — it greatly increases NAPQI generation relative to a non-induced individual, making a standard nomogram level unreliable. (2) HIV/TB co-infection with poor nutritional status is associated with depleted glutathione stores. In patients with enzyme-inducing drugs (rifampicin, carbamazepine, phenytoin, isoniazid), chronic alcohol use, or malnutrition, the nomogram treatment line should be adjusted downward — many guidelines recommend treating at 50% of the standard nomogram line. Start NAC regardless of the apparent level.
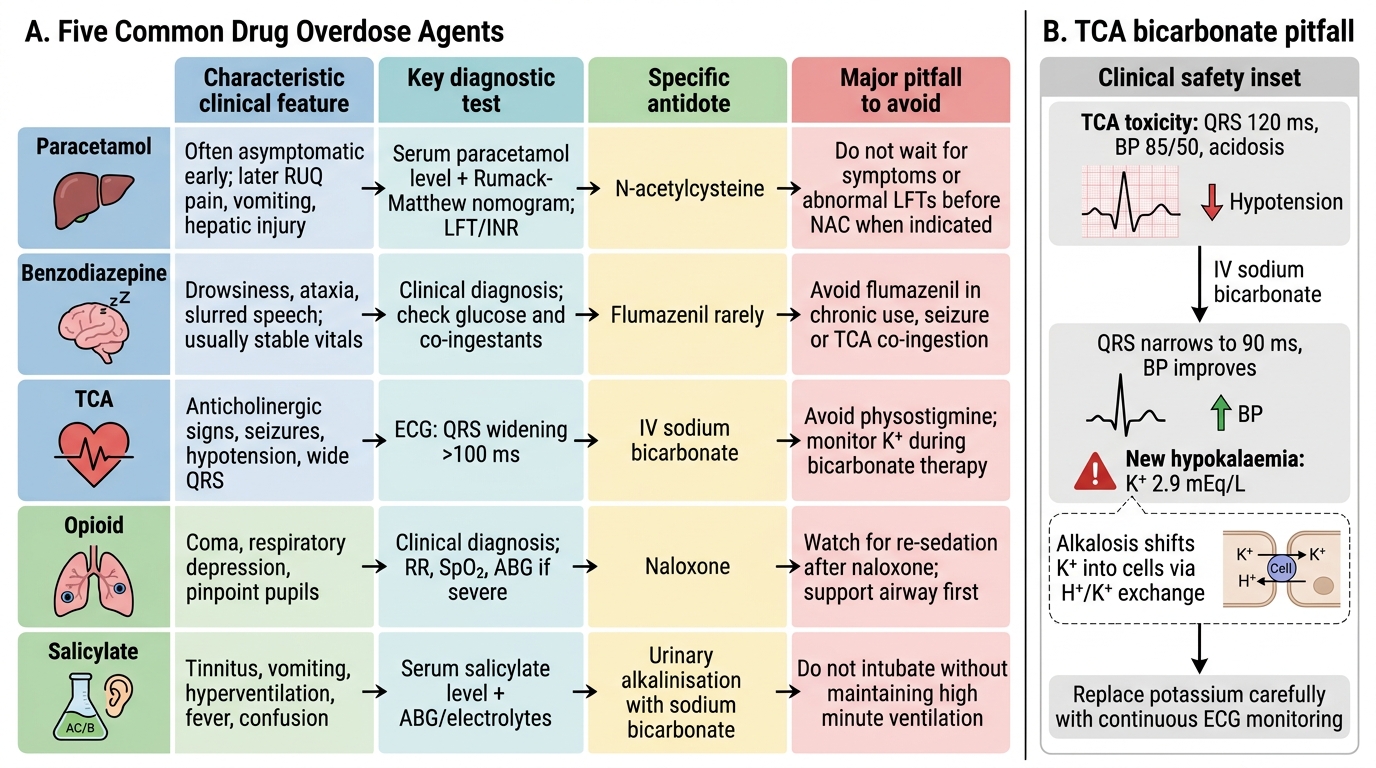
Five Overdose Agents: Features, Tests, Antidotes, Pitfalls
SELF-CHECK
A 50-year-old woman on chronic imipramine (TCA) for depression presents drowsy after taking extra tablets. ECG: QRS 120 ms. BP 85/50. ABG pH 7.30 (acidosis). She is given IV sodium bicarbonate. Thirty minutes later, ECG shows QRS 90 ms and BP improves to 100/70. Her serum potassium is now 2.9 mEq/L. What is the most likely cause of the hypokalaemia and what must be done?
A. TCA cardiac toxicity is causing K loss — give digoxin-specific Fab
B. Bicarbonate infusion drives K into cells — replace potassium carefully with ECG monitoring
C. Opioid co-ingestion causing adrenal suppression — give hydrocortisone
D. Salicylate co-ingestion is present — start urinary alkalinisation
Reveal Answer
Answer: B. Bicarbonate infusion drives K into cells — replace potassium carefully with ECG monitoring
Sodium bicarbonate infusion creates an alkalotic environment, which drives potassium from the extracellular to intracellular compartment via the H+/K+ exchanger — producing hypokalaemia. This is the most common metabolic complication of bicarbonate therapy. Hypokalaemia is dangerous because it prolongs the QTc and increases risk of torsades de pointes, which would worsen the already-compromised cardiac situation. Careful IV potassium replacement (with continuous ECG monitoring) is mandatory. Digoxin Fab is for cardiac glycoside toxicity. Hydrocortisone and urinary alkalinisation are not relevant here.
CLINICAL PEARL
The silent period of paracetamol toxicity is its most dangerous feature and the most common cause of missed treatment. A patient who feels completely well at 2 hours post-ingestion can develop fulminant hepatic failure by day 3 if not treated. The 4-hour level is non-negotiable: even if the patient appears entirely normal, the level must be checked at 4 hours and plotted on the Rumack-Matthew nomogram before any decision to discharge.
For TCA overdose, remember that acid makes things worse: metabolic acidosis dramatically increases TCA-mediated sodium channel blockade (more TCA in the non-ionised form at lower pH). This means that anything that worsens acidosis — hypoxia, hypoventilation, seizures — makes TCA toxicity more lethal. The therapeutic logic of sodium bicarbonate is therefore not just chemical antidote action but also prevention of the acidosis-toxicity spiral. Treat hypoxia and ventilation first; give bicarbonate for QRS widening; never give flumazenil or physostigmine in suspected TCA overdose.