Page 11 of 27
IM22.6 | Insecticide Poisoning — SDL Guide (Part 2)
Management: Atropine Protocol and Pralidoxime
The management of organophosphate poisoning is built on three concurrent pillars: (1) cardiorespiratory stabilisation and decontamination; (2) atropine titration to reverse the life-threatening muscarinic features; and (3) pralidoxime administration to prevent irreversible ageing and preserve neuromuscular function. The single most important determinant of survival is adequate and timely atropinisation. Undertreated muscarinic features — persistent bronchorrhoea and bronchospasm — kill the patient through asphyxiation; appropriately dosed atropine prevents this. There is no other lesson in OP poisoning management as important as understanding what the correct atropine endpoint is and how to reach it. The failure to achieve adequate atropinisation is responsible for the majority of preventable deaths in Indian district hospitals. This failure is almost always a dosing failure — not a diagnostic failure or a drug unavailability problem. Atropine is cheap, widely available, and fully effective when dosed correctly: it is the clinical knowledge of the correct endpoint and the confidence to escalate the dose that saves lives. The sections below give the step-by-step management protocol with exact doses, endpoints, and decision criteria.
Step 1 — Stabilisation and Decontamination:
- Protect healthcare staff: wear gloves and gown before touching the patient (OP can be absorbed through skin — secondary contamination is a real hazard).
- Remove all clothing; wash skin thoroughly with soap and water (dermal decontamination — reduces ongoing absorption significantly).
- Establish IV access; apply cardiac monitor and pulse oximeter.
- High-flow oxygen; bag-valve-mask ventilation if respiratory rate is inadequate.
- Activated charcoal 50 g via NGT if oral ingestion, within 1 hour, and airway is protected — but airway stabilisation and atropine must come first.
Step 2 — Atropine: Loading and titration:
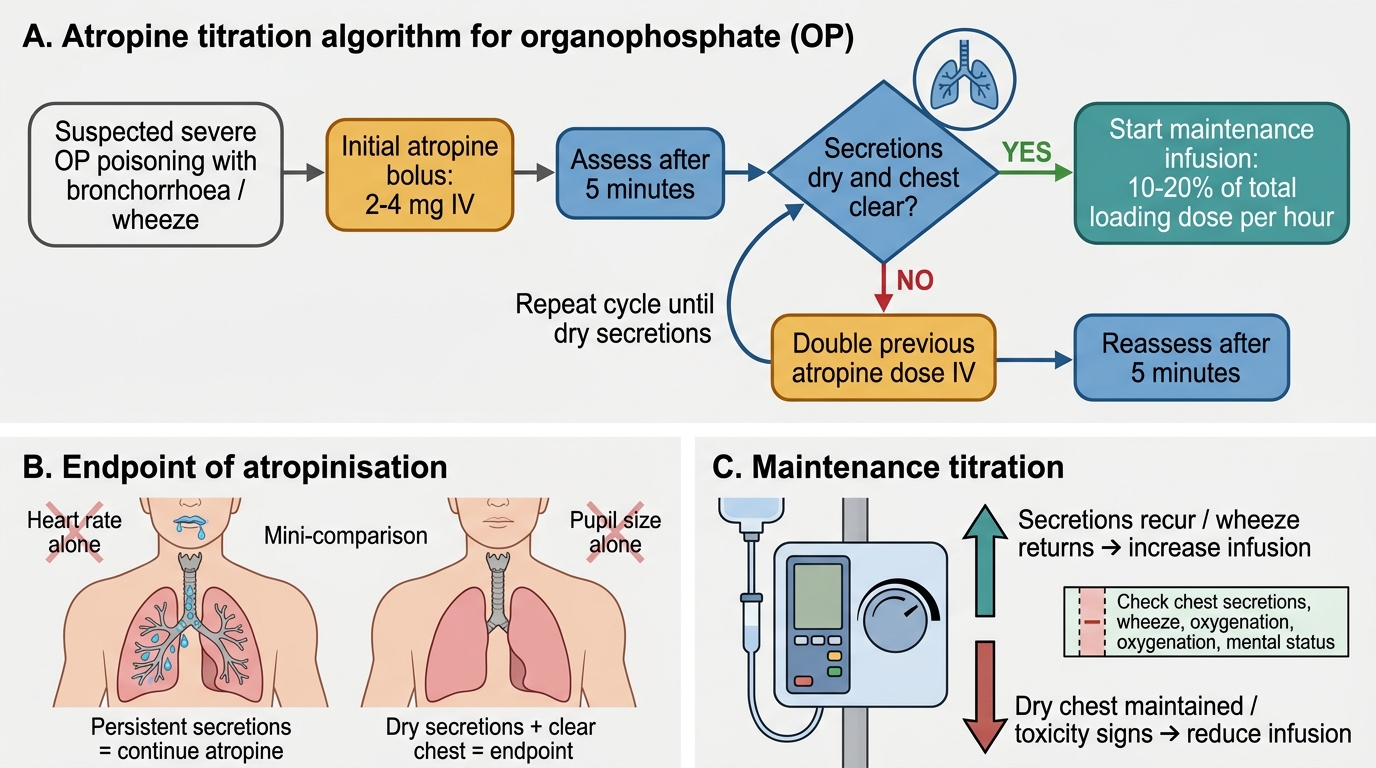
Atropine competitively blocks muscarinic receptors, reversing bronchorrhoea, bradycardia, and bronchospasm. It has NO effect on nicotinic features (fasciculations, paralysis). The dose required in severe OP poisoning is vast compared to routine clinical use — starting at 2–4 mg IV (not 0.6 mg) and doubling every 5–10 minutes until the atropinisation endpoint is reached.
The correct endpoint for atropine titration is: drying of secretions and clearing of pulmonary wheeze. Specifically: dry oropharynx, absent or minimal bronchial secretions on auscultation (clear lung fields), and resolved wheeze. This is NOT pupil dilation (the pupils in severe OP poisoning may never fully dilate even with adequate atropinisation because the nicotinic component at the iris also plays a role) and NOT heart rate (the goal is secretion control — if secretions are dry at HR 100, that is adequate; if secretions continue at HR 140, more atropine is needed). A common and fatal error is targeting heart rate or pupil dilation.
Practical protocol:
- Loading: Atropine 2–4 mg IV bolus; if no drying of secretions in 5 minutes, double to 4–8 mg; continue doubling every 5 minutes until secretions dry.
- Maintenance: Once the endpoint is reached, start an atropine infusion at 10–20% of the loading dose per hour; titrate up or down based on recurrence of secretions.
- Total atropine doses in severe OP poisoning are typically 20–100 mg in the first 24 hours; individual case reports document hundreds of milligrams. There is NO upper dose limit in cholinergic crisis — the endpoint determines when to stop, not a dose ceiling.
- Oral atropine (tablet or injection given orally) is used for maintenance once the acute phase is controlled.
Step 3 — Pralidoxime (2-PAM):
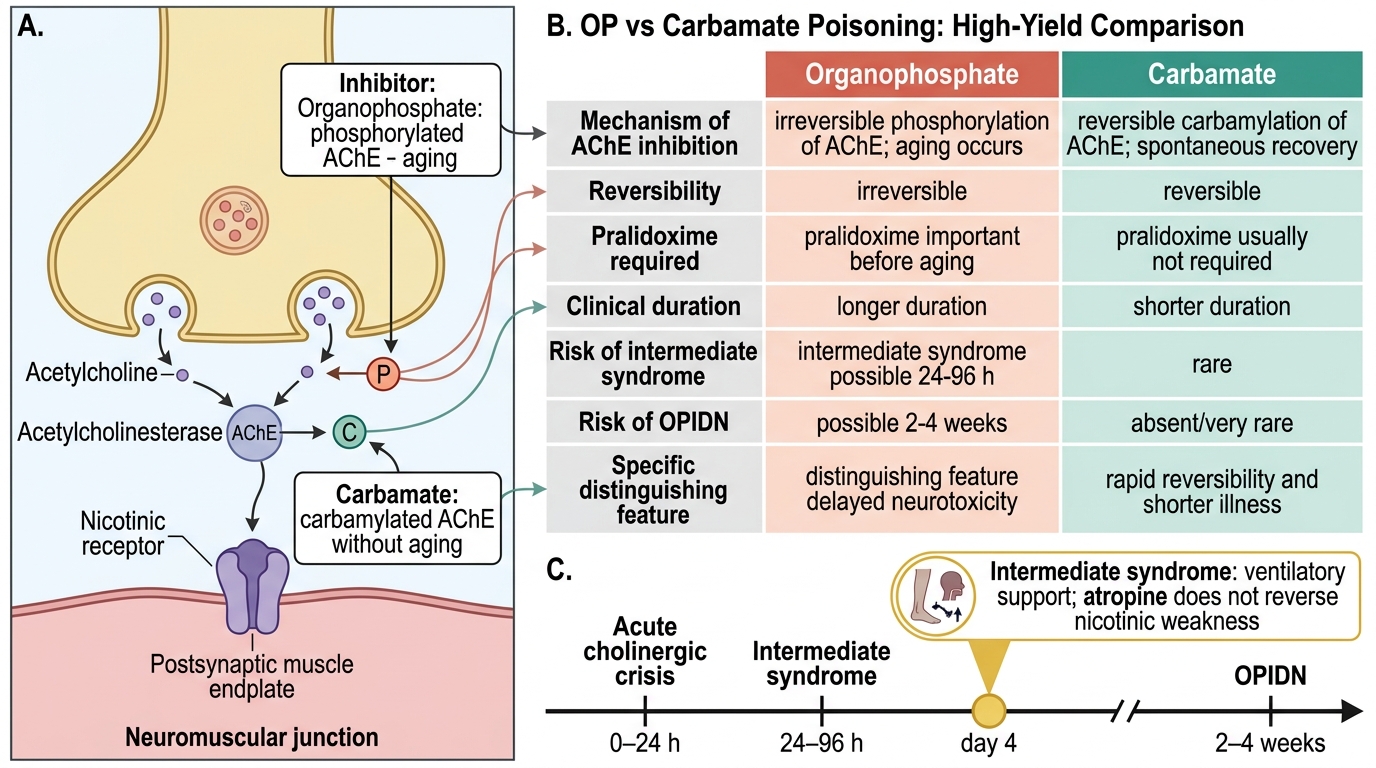
Pralidoxime reactivates AChE by displacing the phosphate group before ageing renders the bond irreversible. The time window for efficacy is critical: most agricultural OPs allow a 24–48 hour window for pralidoxime to be effective, though initiation within 6 hours is optimal.
- Dose: 1–2 g IV (diluted in 100 mL normal saline) over 15–30 minutes as loading dose; then 500 mg/hour infusion or repeat doses every 4–6 hours.
- Duration: Continue until atropine requirements reduce, cholinesterase activity recovers, or clinical improvement is sustained.
- NOT required for carbamate poisoning (carbamylation is self-reversing).
- Pralidoxime is INEFFECTIVE after irreversible ageing — it cannot break the aged (irreversible) phosphorylated enzyme bond.
Step 4 — Seizure management:
Benzodiazepines (diazepam 5–10 mg IV or lorazepam 2–4 mg IV) are the treatment of choice for OP-induced seizures. Phenytoin is NOT effective for seizures driven by muscarinic/cholinergic mechanisms. Phenobarbital can be used as a second-line agent.
Step 5 — Mechanical ventilation:
Indications: persistent hypoxia (SpO₂ < 90% despite oxygen and atropinisation), respiratory rate > 30 or < 10, GCS ≤ 8, or evidence of respiratory muscle paralysis (weak respiratory effort, paradoxical chest wall movement, impending exhaustion). Many patients in India die because ventilator availability at district hospitals is limited — early recognition of the need for ventilation and timely referral to a facility with ICU capability is critical.
Atropine Titration Protocol in Organophosphate Poisoning
SELF-CHECK
A 55-year-old farmer with severe OP poisoning has received 12 mg of atropine over 30 minutes in escalating doses. His heart rate is now 110 bpm and pupils are 4 mm. However, auscultation of the chest still reveals bilateral wheeze and bronchial secretions are visible at the lips. What is the correct next step?
A. Stop atropine — heart rate 110 indicates atropinisation is adequate
B. Continue atropine titration — the endpoint is dry secretions, not heart rate or pupil size
C. Switch to glycopyrrolate as atropine has reached its maximum effective dose
D. Give pralidoxime 2 g IV as additional atropine will cause anticholinergic toxicity
Reveal Answer
Answer: B. Continue atropine titration — the endpoint is dry secretions, not heart rate or pupil size
The endpoint for atropine titration in OP poisoning is DRYING OF SECRETIONS and clearing of bronchial wheeze — not heart rate normalisation, not pupil dilation, and not a specific dose ceiling. At HR 110 with persistent bronchorrhoea and wheeze, the patient is NOT adequately atropinised. The muscarinic effect on airways is still dominant and the patient remains at risk of asphyxiation. More atropine is required. There is no upper dose limit in cholinergic crisis. Glycopyrrolate is an alternative/adjunct but does not replace further atropine titration at this stage. Pralidoxime should already be running and addresses nicotinic (NMJ) effects, not muscarinic secretions.
Complications: Intermediate Syndrome and Delayed Neuropathy
Organophosphate poisoning produces two important delayed complications that occur after the acute cholinergic crisis has been apparently controlled — intermediate syndrome and organophosphate-induced delayed polyneuropathy. Both are unique to organophosphate poisoning (not carbamate) and recognition of their clinical patterns is essential for appropriate monitoring and management during the recovery phase.
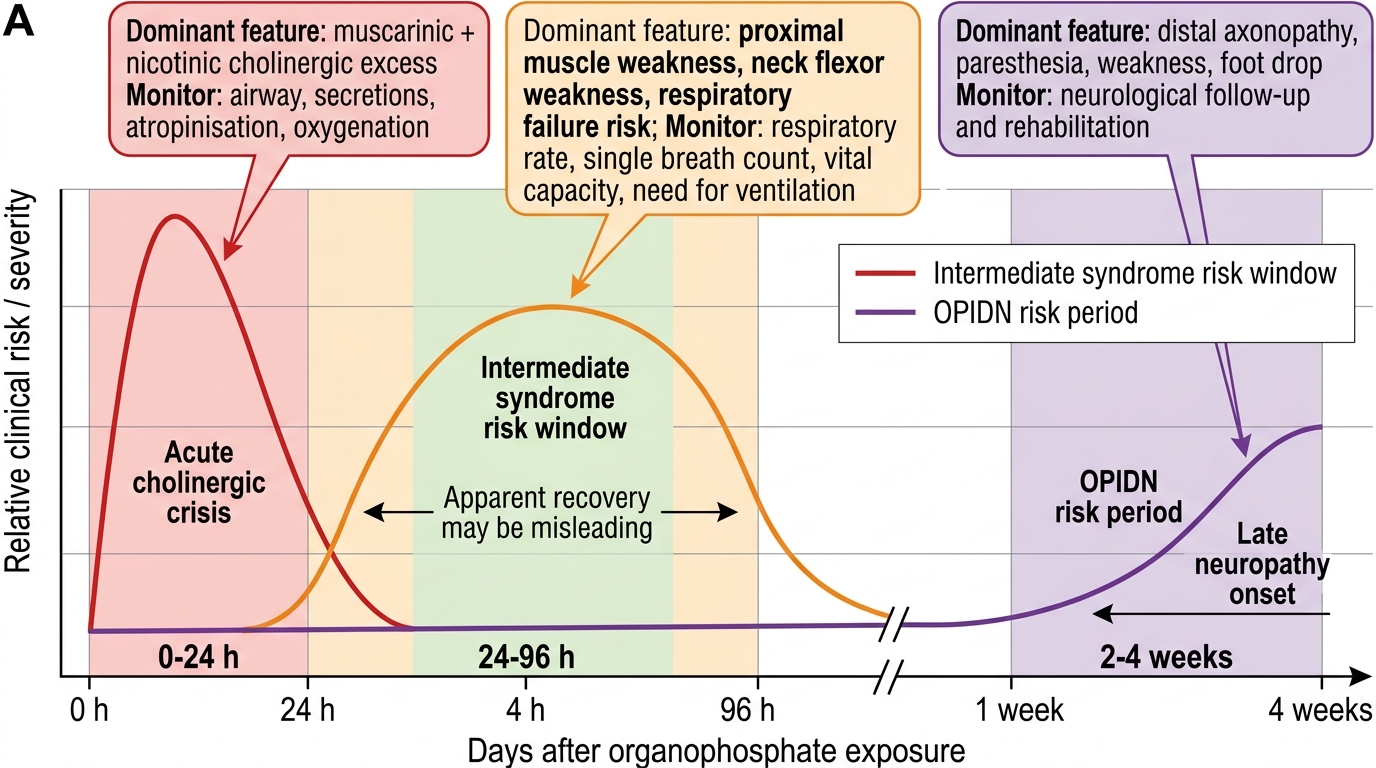
Intermediate syndrome (IMS) is a syndrome of acute muscular weakness and paralysis that occurs 24–96 hours after the acute cholinergic crisis, during what appears to be a period of clinical recovery when the acute secretion crisis has been controlled and atropine requirements are decreasing. It is caused by sustained accumulation of ACh at nicotinic receptors at the NMJ — persistent NMJ dysfunction leads to a depolarisation block that manifests as proximal limb weakness, neck flexor weakness, and — most critically — respiratory muscle paralysis (including diaphragmatic paralysis). IMS accounts for a significant proportion of late deaths from OP poisoning, occurring after patients have survived the acute phase and are apparently improving. Clinical features: proximal limb weakness (difficulty raising arms), difficulty swallowing, neck weakness, shallow breathing, and rapidly developing respiratory failure — often without any antecedent warning. Regular monitoring of respiratory function (serial assessment of respiratory rate, tidal volume, and ability to count out loud to 20 in one breath) is mandatory during the first 96 hours. Pralidoxime is thought to reduce the incidence of IMS when given early; treatment is mechanical ventilatory support until NMJ function recovers (days to weeks). Serum cholinesterase levels are typically very low during IMS.
Organophosphate-induced delayed polyneuropathy (OPIDN) is a rare but severe late complication occurring 2–4 weeks after exposure to certain OP compounds (particularly triorthocresyl phosphate — TOCP; also trichlorfon and some others). It is caused by inhibition of neuropathy target esterase (NTE) — a distinct enzyme from AChE — leading to axonal degeneration of long peripheral nerve fibres and corticospinal tracts. Clinical features: ascending distal weakness and sensory loss beginning in the lower limbs, progressing to a predominantly motor peripheral neuropathy. In severe cases, spasticity and upper motor neurone signs (due to corticospinal tract involvement) develop later. There is no treatment — recovery is incomplete in many patients. OPIDN is not caused by the acute cholinergic toxicity but by a separate biochemical mechanism, explaining why it occurs in patients who seemed to have fully recovered from the acute poisoning.
QTc prolongation and cardiac arrhythmias: OP compounds have direct cardiac effects independent of their muscarinic effects — QTc prolongation from direct myocardial ion channel effects, ventricular tachycardia, and torsades de pointes. Continuous ECG monitoring is mandatory throughout the acute phase and during the intermediate syndrome risk period.
Timeline of Organophosphate Poisoning Complications
Prognosis and Self-Assessment
The prognosis of organophosphate poisoning is primarily determined by three factors: the severity of the initial cholinergic crisis (reflected in the degree of AChE inhibition and the speed of presentation), the adequacy and timeliness of atropinisation, and the availability of mechanical ventilation. In India, case fatality rates in district hospital settings range from 10–30%, largely reflecting inadequate atropine dosing and limited ICU capacity rather than the inherent lethality of the toxin. In well-resourced centres with appropriate atropinisation and ventilatory support, mortality drops dramatically. Carbamate poisoning, in contrast, has a better prognosis because AChE inhibition is reversible and the clinical course is shorter.
Factors associated with poor prognosis include: delay in presentation to hospital (> 4 hours), highly toxic OP compounds (mevinphos, parathion), oral ingestion of large volume, severe initial AChE suppression (< 10% of normal), need for mechanical ventilation, development of intermediate syndrome, and refractory QTc prolongation/ventricular arrhythmia.
The following scenarios test your application of OP poisoning knowledge:
Scenario A: A 28-year-old man is brought in 2 hours after drinking an unknown agricultural chemical. GCS 12, pulse 32 bpm, copious salivation, bilateral wheeze, fasciculations. You have atropine ampoules of 0.6 mg and 1 mg available. Outline the first 30 minutes of management.
Analysis: (1) Wear gloves and remove patient's clothing. (2) High-flow oxygen; IV access; cardiac monitor. (3) Start atropine: give 0.6 mg + 0.6 mg + 0.6 mg + 0.6 mg = 2.4 mg immediately to approximate a 2–4 mg loading dose. Reassess in 5 minutes. If secretions persist and wheeze continues, double the dose — give another 2.4 mg. Repeat every 5 minutes until secretions dry. (4) Pralidoxime 1–2 g IV in 100 mL NS over 30 minutes (run concurrently with atropine). (5) Activated charcoal 50 g via NGT after airway is protected. (6) Benzodiazepines on standby for seizures.
Scenario B: A 42-year-old woman survived an acute OP poisoning crisis and was weaned off atropine on day 2. On day 3, the ward nurse calls you urgently: the patient is having difficulty breathing, her RR is 32/min, she cannot count past 10 in one breath, and her proximal arm muscles are weak. ECG shows QTc 510 ms. What complication has occurred and what is the treatment?
Analysis: This is intermediate syndrome — developing on day 3, after apparent recovery from the acute cholinergic crisis. The hallmarks are: proximal limb weakness + neck/respiratory muscle weakness + developing respiratory failure. Treatment: immediate ICU transfer; mechanical ventilation before complete respiratory arrest; monitor and correct QTc (withhold drugs that prolong QTc; correct hypokalaemia). Continue pralidoxime if still within its effective window. The patient will need ventilatory support for days to weeks until NMJ function recovers. Reassure family that this is a recognised complication and recovery is expected with appropriate support.
Organophosphate vs Carbamate Poisoning
SELF-CHECK
A 35-year-old woman is admitted with confirmed organophosphate poisoning. After receiving a total of 40 mg of atropine over 6 hours and 1 g pralidoxime, her acute cholinergic crisis has resolved. On day 4, she develops bilateral proximal arm weakness, difficulty swallowing, and her respiratory rate rises from 14 to 28 breaths per minute. She had not been on atropine for 48 hours. Which complication is MOST likely?
A. Recurrence of acute cholinergic crisis from residual OP absorption
B. Intermediate syndrome requiring ventilatory support
C. Organophosphate-induced delayed polyneuropathy (OPIDN)
D. Atropine toxicity causing muscular weakness
Reveal Answer
Answer: B. Intermediate syndrome requiring ventilatory support
Intermediate syndrome (IMS) typically occurs 24-96 hours after the acute cholinergic crisis has resolved — exactly the presentation described here on day 4. The hallmarks are: proximal limb weakness, neck flexor weakness, dysphagia, and respiratory muscle paralysis developing in a patient who had apparently recovered. IMS is caused by persistent nicotinic NMJ dysfunction (depolarisation block) rather than renewed muscarinic stimulation — it does not respond to atropine. Treatment is immediate ventilatory support. OPIDN occurs 2-4 weeks post-exposure with predominantly sensory and distal motor features. Acute cholinergic crisis recurrence would show SLUDGE features and bradycardia, which are absent here. Atropine toxicity causes anticholinergic features — the opposite of weakness.
CLINICAL PEARL
The atropine titration endpoint is the single most important pharmacological principle in all of emergency toxicology in India. Print it, memorise it, and teach it to every junior colleague: the endpoint is DRY SECRETIONS and CLEAR CHEST — not pupil dilation, not heart rate. Students and junior doctors reflexively look for pupil changes because they were taught to use atropine in bradycardia at 0.6 mg. OP poisoning requires a completely different paradigm — large doses, titrated to secretion control, with no dose ceiling. A patient who dies from OP poisoning in India almost always has the same story: inadequate atropine, given in 0.6 mg increments, stopped because the heart rate rose, while secretions continued to flood the airways.
A second pearl: intermediate syndrome is invisible if you are not looking for it. On day 2–3, when the patient appears to be recovering, assess respiratory function actively every 4–6 hours: count-to-20 test, check for proximal arm weakness, measure tidal volume. Do not be reassured by a normal resting respiratory rate — IMS can precipitate respiratory arrest with very little warning.