Page 4 of 32
IM25.{3,5-7} | Geriatric Neuropsychiatric Syndromes — SDL Guide
Learning Objectives
- Define delirium using DSM-5 criteria and apply the Confusion Assessment Method (CAM) to diagnose its three motor subtypes
- Enumerate common precipitants of delirium and describe non-pharmacological and pharmacological management principles
- Classify the major types of dementia and describe the distinguishing clinical and neuroimaging features of Alzheimer, vascular, Lewy body, and frontotemporal dementia
- Describe the pharmacological management of Alzheimer dementia and the management of behavioural and psychiatric symptoms, including the neuroleptic sensitivity warning in Lewy body dementia
- Screen for geriatric depression using the GDS and differentiate pseudodementia from true dementia
- Prescribe first-line antidepressant therapy and recognise when ECT is appropriate in elderly depression
INSTRUCTIONS
This module covers the four major geriatric neuropsychiatric syndromes: delirium, dementia, depression, and personality change. The critical skill is accurate differential diagnosis — delirium and dementia can coexist, depression can mimic dementia, and Lewy body dementia requires specific management modification. Apply the diagnostic frameworks presented here to every clinical encounter with a confused or cognitively impaired elderly patient.
References
- Harrison's Principles of Internal Medicine, 21st ed., Chs 31, 423 — Delirium and Dementia (textbook)
- API Textbook of Medicine, 11th ed., Chapter on Geriatric Neuropsychiatric Disorders (textbook)
- DSM-5 American Psychiatric Association 2013 — Neurocognitive Disorders (guideline)
- National Institute for Health and Care Excellence (NICE) Guideline: Dementia — Assessment, Management and Support (NG97), 2018 (guideline)
- NICE Clinical Guideline: Delirium — Prevention, Diagnosis and Management (CG103), 2019 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
The night nurse calls the medicine ward at 02:00 hours: 'Mr Nair, 78 years old, admitted yesterday for a hip fracture, is pulling out his intravenous line, shouting that strangers are trying to poison him, and refuses to stay in bed.' When you arrive, he is agitated, disoriented to time and place, and cannot recall his own name. Three days later, after correcting his medications, treating a silent urinary infection, and improving his sleep environment, he is calm, oriented, and remembers the whole admission as 'a terrible nightmare.' Six months later the same Mr Nair presents to the neurology outpatient with his wife, who reports a gradual one-year decline in memory — he forgets conversations, gets lost driving familiar routes, and has become socially withdrawn. Neuropsychological testing confirms dementia. These two encounters illustrate the critical distinction that defines geriatric neuropsychiatry: delirium is acute and reversible; dementia is chronic and progressive. Yet they can coexist, one can trigger the other, and both can mask or mimic each other. Accurate diagnosis determines management — and this module gives you the framework to do it correctly.
WHY THIS MATTERS
Neuropsychiatric syndromes — delirium, dementia, depression, and personality change — are among the most prevalent and most consequential conditions in geriatric medicine. Delirium occurs in 14–24% of hospitalised elderly patients and is independently associated with increased mortality, prolonged hospitalisation, accelerated cognitive decline, and new institutionalisation. Dementia affects approximately 4 million Indians (Alzheimer's and Related Disorders Society of India) and is the leading cause of acquired cognitive disability in the elderly worldwide. Depression in the elderly is under-diagnosed and undertreated, despite being the most treatable major psychiatric disorder, with high rates of response to appropriate therapy. NMC competencies IM25.3 (delirium/acute confusional state), IM25.5 (depression), IM25.6 (dementia), and IM25.7 (personality change in the elderly) require KH-level competency across these four conditions — you must not only know their pathophysiology but be able to diagnose, acutely manage, and plan rehabilitation for each.
RECALL
Before proceeding, recall your foundations. The neurotransmitter systems most relevant to geriatric neuropsychiatry: acetylcholine (ACh) — central role in attention and memory; ACh deficiency is the core neurochemical basis of Alzheimer dementia and is exploited by anticholinergic drugs that worsen cognition. Dopamine — the target of antipsychotics (D2 blockade) used in delirium management; imbalance between dopamine and ACh is central to delirium pathophysiology. Serotonin — reduced in depression; target of SSRIs. The limbic system (hippocampus, amygdala, entorhinal cortex) mediates memory consolidation and emotional regulation — the primary site of Alzheimer pathology. Recall the DSM-5 diagnostic criteria concept — psychiatric diagnoses require specific symptom criteria, duration, and functional impairment. You will apply DSM-5 criteria for delirium, major neurocognitive disorder (dementia), and major depressive disorder in this module.
Delirium: Clinical Presentation and Pathophysiology
Delirium (acute confusional state) is a neuropsychiatric syndrome characterised by acute onset and fluctuating course, inattention, and either disorganised thinking or altered level of consciousness. The DSM-5 diagnostic criteria for delirium require: (A) disturbance in attention and awareness; (B) the disturbance develops acutely (hours to days), represents a change from baseline, and tends to fluctuate during the day; (C) additional cognitive disturbance (memory, disorientation, language, visuospatial, or perception); (D) the disturbances are not better explained by pre-existing neurocognitive disorder; (E) evidence from history, examination, or investigation that the disturbance is caused by a medical condition, substance intoxication or withdrawal, or medication. The critical features distinguishing delirium from dementia are onset (acute vs insidious) and fluctuation (fluctuating vs stable-progressive course).
Provided image
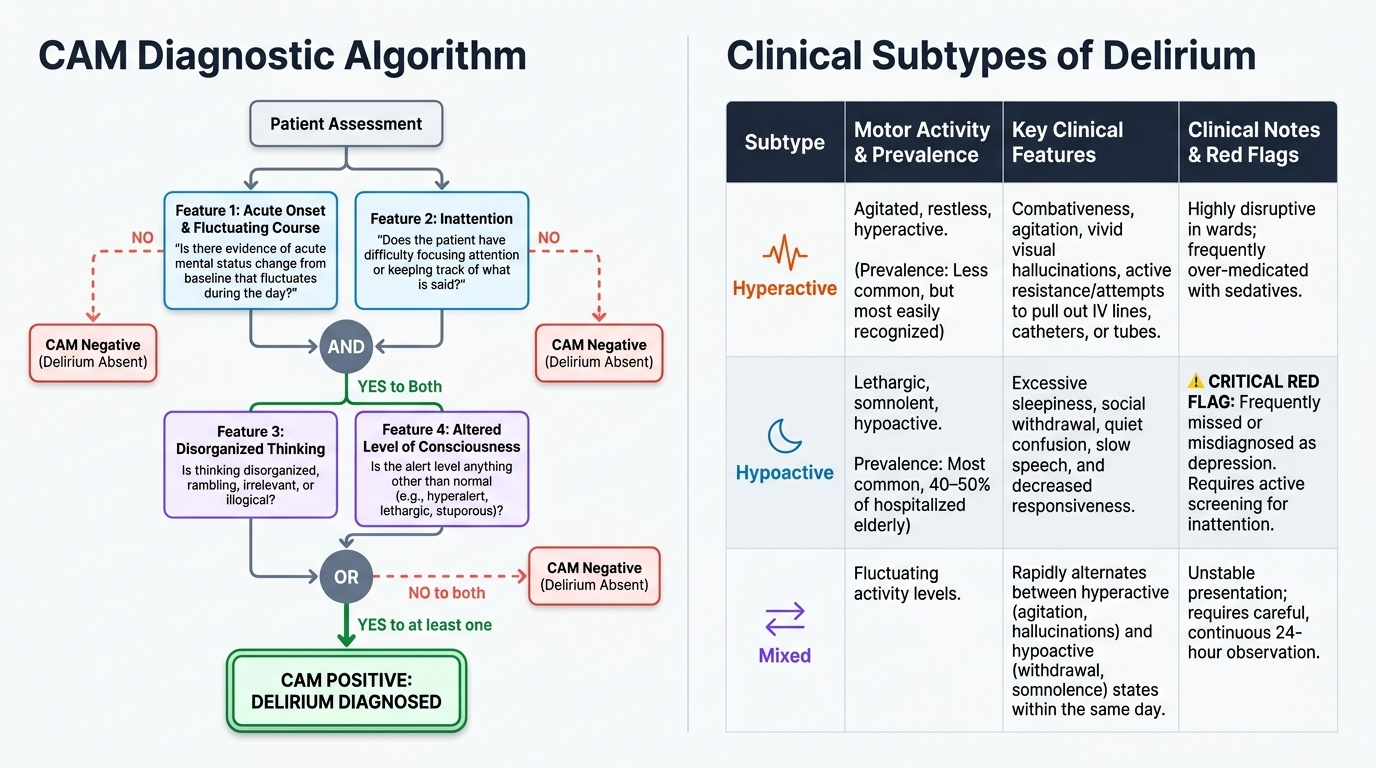
Delirium presents in three motor subtypes. Hyperactive delirium — the type most easily recognised and causing most ward disturbance — involves agitation, restlessness, combativeness, hallucinations (typically visual), and attempts to remove lines and tubes. Hypoactive delirium — paradoxically the most common subtype in hospitalised elderly (40–50% of cases) and the most frequently missed — presents as excessive somnolence, withdrawal, and quiet confusion that is often erroneously labelled 'depression' or attributed to the underlying illness. Mixed subtype alternates between hyperactive and hypoactive features within the same day. Missing hypoactive delirium is a common error; a patient who is 'very quiet and not eating' in the medical ward must be assessed for inattention (the cardinal delirium symptom) using a validated screen.
The Confusion Assessment Method (CAM) is the most widely validated and clinically practical delirium screening tool (sensitivity 94%, specificity 89%). It requires four features: (1) acute onset and fluctuating course (yes/no: is there evidence of acute mental status change that fluctuates during the day?); (2) inattention (yes/no: does the patient have difficulty focusing attention, e.g., is easily distracted?); (3) disorganised thinking (yes/no: is the patient's thinking disorganised or incoherent — rambling conversation, unclear or illogical flow of ideas?); (4) altered level of consciousness (anything other than alert). CAM is positive (delirium present) if features 1 AND 2 are present, plus EITHER feature 3 OR 4.
The pathophysiology of delirium is incompletely understood but involves a final common pathway of diffuse brain dysfunction resulting from widespread neuroinflammation and neurotransmitter dysregulation. The prevailing hypothesis is that predisposing vulnerabilities (older age, pre-existing cognitive impairment, sensory impairment, dehydration, immobility) combine with precipitating insults (infection, surgery, drugs, metabolic disturbance) to overwhelm the brain's capacity to maintain coherent consciousness and attention. The central neurochemical imbalance is reduced cholinergic activity (the acetylcholine system is critical for attention and arousal) combined with increased dopaminergic activity — this combination produces the attentional failure and perceptual disturbances of delirium. Drugs with anticholinergic properties (antihistamines, tricyclics, bladder antimuscarinics, some antipsychotics) are major precipitants and must be identified and stopped.
Delirium: Aetiology, Management and Rehabilitation
The aetiology of delirium is best remembered with the mnemonic PINCH ME (used in the UK geriatric curriculum) or the broader AEIOU-TIPS framework. The most common precipitants in hospitalised elderly are: infection (pneumonia, UTI — though asymptomatic bacteriuria should not be treated); drugs (opioids, benzodiazepines, anticholinergics, steroids, antibiotics, digoxin, polypharmacy); metabolic disturbances (hyponatraemia, hypernatraemia, hypoglycaemia, hyperglycaemia, uraemia, hepatic encephalopathy, thyroid dysfunction); hypoxia (pneumonia, pulmonary embolism, heart failure); pain (especially in cognitively impaired patients who cannot verbalise pain — inadequately treated pain causes hyperactive delirium); urinary retention and constipation (both are potent and reversible causes, especially in elderly men on anticholinergic medications); environmental disruption (ICU psychosis — sensory overload, sleep deprivation, continuous lighting); neurological causes (stroke, subdural haematoma, meningitis, encephalitis — must be excluded with CT brain/LP when delirium is new and lacks clear metabolic cause). Alcohol and drug withdrawal are important causes in any age group.
Investigation of new delirium should be systematic: full blood count (infection, anaemia), metabolic panel (electrolytes, glucose, urea, creatinine), liver function tests, thyroid function, blood cultures if fever, urinalysis (interpret with caution as described), chest X-ray, ECG, and arterial blood gas if hypoxia suspected. CT brain is indicated if there is new focal neurological deficit, head injury, or no clear alternative explanation. Lumbar puncture if meningitis or encephalitis suspected (fever + confusion + neck stiffness or rash).
Management of delirium follows the principle that treating the cause is the primary intervention. The single most effective approach is identifying and reversing the precipitating factor(s). Simultaneously, non-pharmacological management is the cornerstone: reorientation (clock, calendar, familiar photographs, staff introducing themselves at every contact), maintaining day-night cycle (natural light exposure during the day, minimising night-time interruptions), providing glasses and hearing aids, early mobilisation, facilitating family presence, minimising invasive lines and urinary catheters, ensuring adequate hydration and nutrition, and adequate pain control. These interventions are bundled in the evidence-based Hospital Elder Life Program (HELP) intervention, which reduces delirium incidence by 30% and delirium duration in hospitalised elderly.
Pharmacological management is second-line, reserved for patients who pose a risk to themselves or others despite optimal non-pharmacological care. Haloperidol (oral or IV, 0.25–0.5 mg every 4 hours as needed, maximum 3 mg/24 hours in elderly) remains the best-evidenced agent for hyperactive delirium — it targets the dopaminergic excess component. Risks include extrapyramidal side effects and QTc prolongation (check ECG; avoid if QTc >450 ms). Atypical antipsychotics (quetiapine, olanzapine) have less extrapyramidal risk and are used when haloperidol is not tolerated. Benzodiazepines should be used only for alcohol/sedative withdrawal delirium (CIWA-Ar protocol); in all other delirium subtypes they are contraindicated as they worsen confusion and fall risk. Melatonin has evidence for delirium prevention (not treatment) in medical ICU settings.
Rehabilitation post-delirium: Delirium is not simply 'resolved' when the acute episode clears. Many patients take weeks to return to cognitive baseline; some — particularly those with underlying pre-existing cognitive impairment — do not recover fully. Post-delirium rehabilitation focuses on: monitoring cognitive recovery (serial MMSE), identifying and addressing new-onset functional deficits (physiotherapy for mobility loss during the immobile delirium episode), reviewing and simplifying medications (deprescribing deliriogenic drugs), and educating family caregivers about the post-delirium recovery trajectory.
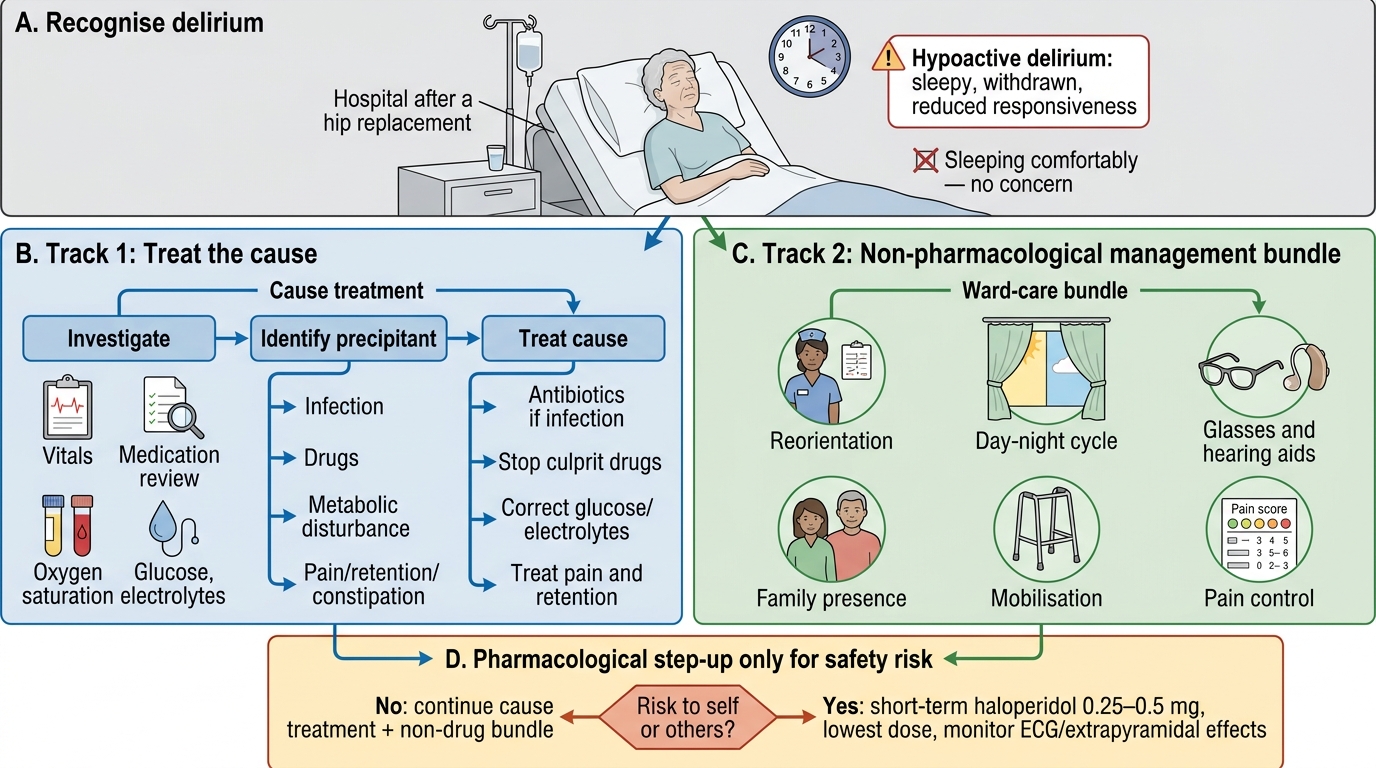
Management Algorithm for Delirium in a Hospitalised Elderly Patient
SELF-CHECK
A 72-year-old woman is admitted to the medical ward following an elective hip replacement. On day 2 she is noted by nurses to be excessively drowsy, barely responsive to verbal stimulation, and 'not herself.' Her night-time sleep has been disrupted. Vital signs are within normal limits. A house officer documents 'patient sleeping comfortably — no concern.' What is the most important diagnostic error in this assessment?
A. Failure to order a CT brain to exclude intracranial haemorrhage
B. Failure to recognise hypoactive delirium — the most common and most frequently missed subtype
C. Failure to obtain psychiatric consultation for possible severe depression
D. Failure to start haloperidol for possible delirium
Reveal Answer
Answer: B. Failure to recognise hypoactive delirium — the most common and most frequently missed subtype
Hypoactive delirium — characterised by excessive somnolence, withdrawal, and reduced responsiveness — is the most common subtype in hospitalised elderly (40–50%) and is the most frequently missed because it is mistaken for appropriate rest or depression. The CAM screen should be applied: acute change (yes — day 2 change from baseline), inattention (likely if tested), plus altered level of consciousness = CAM positive. Dismissing a drowsy post-operative elderly patient as 'sleeping comfortably' without a CAM screen is the most common and dangerous error. CT brain may be needed later if delirium is unexplained, but the immediate error is diagnostic failure. Haloperidol is not first-line — treat the cause first with non-pharmacological measures.
Dementia: Pathophysiology, Types and Clinical Presentation
Dementia is now termed major neurocognitive disorder (DSM-5) — a syndrome characterised by evidence of significant cognitive decline from a previous level of performance in one or more cognitive domains (complex attention, executive function, learning and memory, language, perceptual-motor, social cognition), based on concern from the patient, a knowledgeable informant, or a clinician, AND documented by standardised neuropsychological testing, AND significant interference with independence in everyday activities, AND the disturbance does not occur exclusively during the course of delirium. The key DSM-5 addition of functional impairment criterion (independence compromised) is critical — distinguishing major neurocognitive disorder from mild neurocognitive disorder (MCI) where there is cognitive decline without significant functional impairment.
Alzheimer's disease (AD) accounts for 60–70% of all dementia cases. The neuropathological hallmarks are amyloid-β plaques (extracellular deposits of insoluble amyloid-β peptide resulting from abnormal cleavage of amyloid precursor protein by β- and γ-secretase) and neurofibrillary tangles (intracellular aggregates of hyperphosphorylated tau protein, disrupting axonal transport). The primary neurochemical deficit is reduction in acetylcholine synthesis due to degeneration of the nucleus basalis of Meynert (the main cholinergic projection nucleus), providing the rationale for acetylcholinesterase inhibitor (AChEI) therapy (donepezil, rivastigmine, galantamine). The amyloid cascade hypothesis proposes that amyloid-β accumulation is the initiating event, driving tau hyperphosphorylation, neuronal dysfunction, and eventually neurodegeneration. Clinically, AD begins insidiously with episodic memory impairment (difficulty learning new information, forgetting recent conversations, repeating questions) — reflecting early hippocampal damage — followed by language difficulties (anomia, word-finding problems), visuospatial impairment, and executive dysfunction as neocortical involvement expands. Behavioural and psychiatric symptoms of dementia (BPSD) — including agitation, aggression, depression, apathy, wandering, and psychosis — emerge in 90% of AD patients over the course of the illness.
Vascular dementia (VaD) is the second most common type (15–20%), resulting from cerebrovascular disease causing cumulative ischaemic injury to the brain. The clinical pattern may be stepwise deterioration following strokes (multi-infarct dementia) or insidious progression from small-vessel disease (subcortical ischaemic vascular dementia, Binswanger disease). Cardinal features distinguishing VaD from AD: abrupt onset or stepwise progression; focal neurological signs (hemiparesis, dysarthria, gait abnormality); early executive dysfunction and gait disturbance relative to memory impairment; prominent neuroimaging evidence of ischaemic change (white matter lesions, lacunar infarcts). Risk factor management (hypertension, diabetes, dyslipidaemia, atrial fibrillation) is the cornerstone of VaD prevention and management.
Lewy body dementia (DLB) is characterised by the triad of: fluctuating cognition (hours-to-days fluctuation in attention and alertness — similar to delirium, making differential diagnosis challenging); recurrent well-formed vivid visual hallucinations; and spontaneous parkinsonism (bradykinesia, rigidity, tremor — developing within 12 months of cognitive onset). A critical management point: neuroleptic sensitivity — antipsychotics (especially typical antipsychotics and risperidone) can cause severe, potentially life-threatening adverse reactions in DLB (marked deterioration in cognition, acute parkinsonism, neuroleptic malignant syndrome); cholinesterase inhibitors are relatively more effective in DLB than in AD.
Frontotemporal dementia (FTD) presents at younger ages (50–65 years) with prominent behavioural changes (disinhibition, social inappropriateness, loss of empathy, compulsive/stereotyped behaviours, hyperorality) preceding or overshadowing memory impairment — distinguishing it from AD. The progressive language variants (primary progressive aphasia) present as isolated language disturbance. FTD lacks the amyloid/tau pathology of AD and AChEIs are not beneficial.
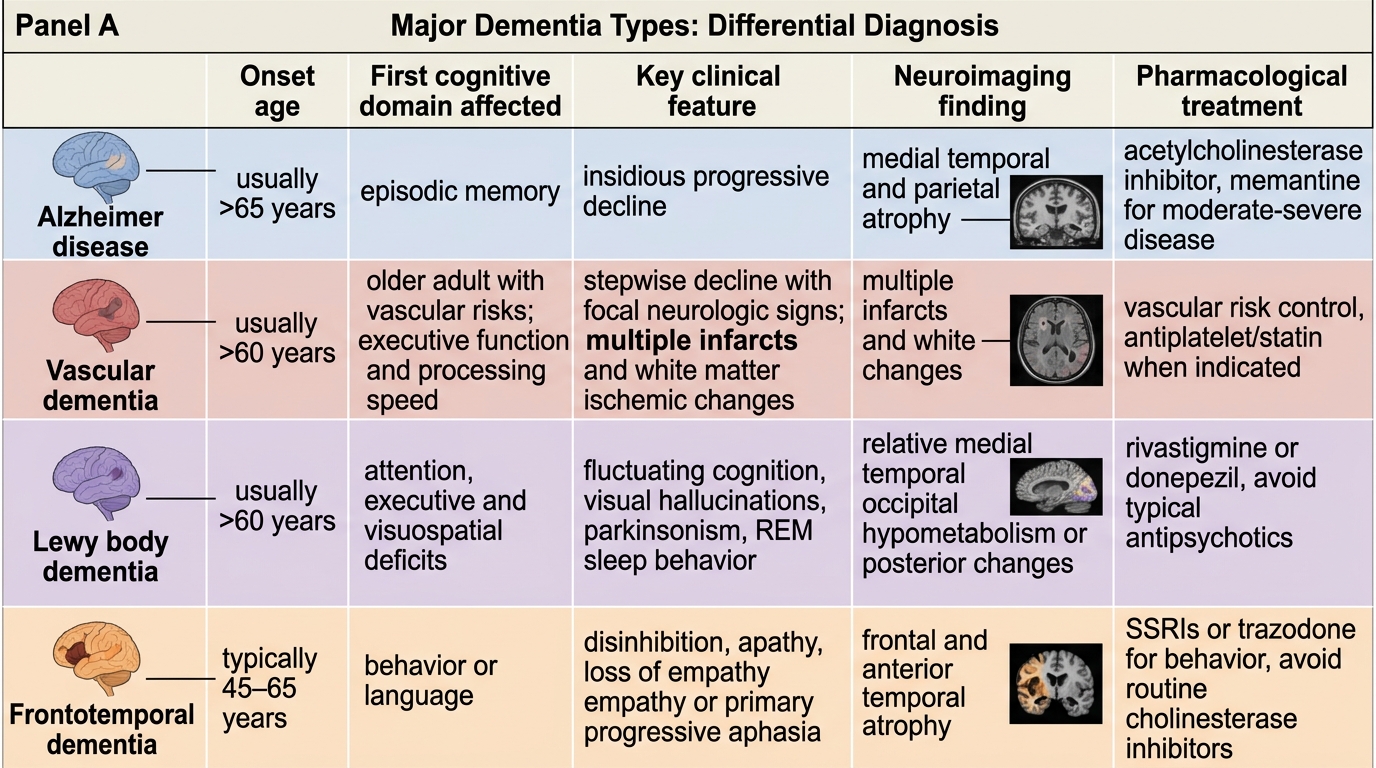
Major Dementia Types: Differential Diagnosis