Page 5 of 32
IM25.{3,5-7} | Geriatric Neuropsychiatric Syndromes — SDL Guide (Part 2)
Dementia: Investigation, Management and Rehabilitation
The investigation of a patient with suspected dementia serves three purposes: to exclude reversible causes of cognitive impairment (which account for approximately 10% of cases), to characterise the dementia type, and to assess comorbidities that influence management. The workup begins with cognitive assessment using MMSE and MoCA (as described in the geriatric assessment module). The reversible causes of cognitive impairment — sometimes recalled as the '3 Ds + 3 Ts' — must be systematically excluded before attributing cognitive decline to irreversible dementia: Depression (pseudodementia — severe depression can produce apparent cognitive impairment that fully resolves with treatment); Drugs (especially benzodiazepines, opioids, anticholinergics, antiepileptics); Delirium superimposed on any cause. The metabolic and structural causes: Thyroid disease (hypothyroidism is a fully reversible cause of cognitive impairment — TSH is mandatory); Tertiary syphilis/neurosyphilis (rare but treatable — RPR/VDRL if clinically suspected); B12/folate deficiency (cobalamin deficiency causes subacute combined degeneration — peripheral neuropathy, posterior/lateral column signs, and cognitive impairment; fully reversible if treated early); additionally subdural haematoma, normal pressure hydrocephalus (NPH) (the triad: wet — urinary incontinence; wacky — cognitive impairment; wobbly — magnetic gait; treated by VP shunting); intracranial tumour; HIV dementia.
The standard investigation panel for dementia: FBC, metabolic panel, TFT, serum B12, folate, fasting glucose, syphilis serology (where clinically indicated), neuroimaging — CT brain (excludes structural causes: SDH, tumour, NPH — identifiable by periventricular lucency and grossly enlarged ventricles out of proportion to atrophy) or MRI brain (superior for characterising atrophy pattern, white matter changes, and hippocampal volume loss in AD). Neuropsychological testing is the gold standard for characterising the cognitive profile. CSF biomarkers (amyloid-β42, tau, p-tau) and PET imaging (amyloid-PET, FDG-PET) are research/specialist tools not routinely available in Indian clinical practice.
Pharmacological management of AD: The only disease-specific pharmacological treatments approved are acetylcholinesterase inhibitors (AChEIs) for mild-to-moderate AD: donepezil (5–10 mg/day, once daily), rivastigmine (1.5–6 mg twice daily; also available as a skin patch), and galantamine (8–24 mg/day). These provide modest but clinically meaningful improvement in cognition and function over 6–12 months. Side effects: nausea, vomiting, diarrhoea, bradycardia (caution in sick sinus syndrome, conduction disease). Memantine (an NMDA receptor antagonist) is approved for moderate-to-severe AD (MMSE <20); it can be combined with an AChEI. There are no disease-modifying therapies available in routine clinical practice. New monoclonal antibodies targeting amyloid (lecanemab, donanemab) have regulatory approval in the US but are not yet available in India.
Management of BPSD (behavioural and psychiatric symptoms of dementia): Non-pharmacological first-line: environmental modification (consistent routine, structured activities, appropriate stimulation), caregiver education, and music/reminiscence therapy. Pharmacological: depression in dementia — SSRI preferred (sertraline, escitalopram; avoid TCAs — anticholinergic burden worsens cognition); psychosis and agitation — atypical antipsychotics (risperidone 0.25–1 mg; quetiapine) at minimal effective dose for the shortest necessary duration; all antipsychotics carry a black box warning for increased mortality in elderly with dementia (approximately 1.6-fold increase in all-cause mortality) and should be used only when BPSD causes significant risk to patient or caregiver. Avoid antipsychotics in DLB (neuroleptic sensitivity — severe adverse reactions).
Rehabilitation in dementia: Cognitive rehabilitation (structured strategies to help patients compensate for memory loss — use of calendars, lists, routines), physical activity programmes (reduce fall risk, improve mood and sleep), social engagement (day care centres, memory cafes), and caregiver education and support (caregiver burden in dementia is exceptionally high — the '36-hour day'; carer support groups, respite services, and depression screening for carers are components of comprehensive dementia management).
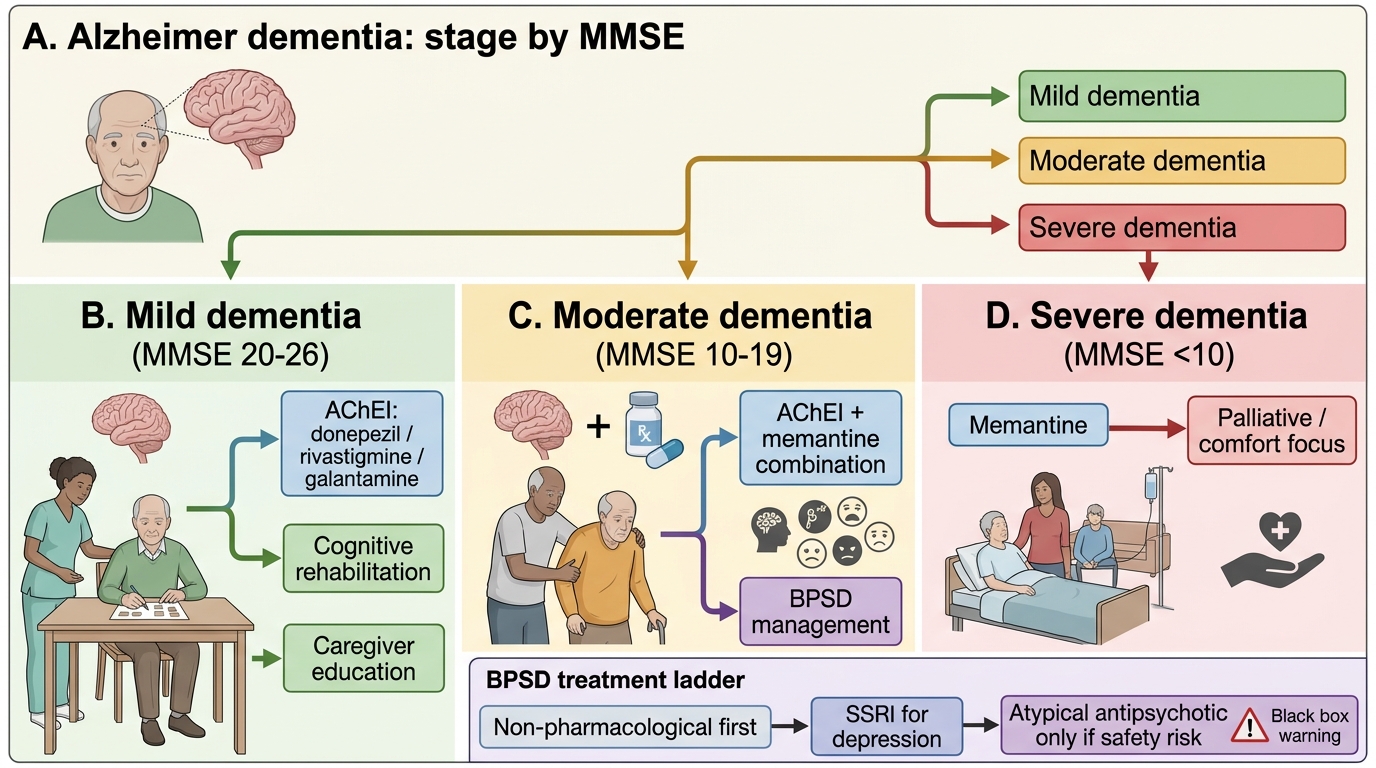
Management Algorithm for Alzheimer Dementia
SELF-CHECK
A 70-year-old man with a 2-year history of progressive cognitive decline (memory, word-finding) and mild parkinsonism develops vivid visual hallucinations (seeing animals in the room) and day-to-day fluctuations in alertness. His MMSE is 19/30. The medical registrar proposes haloperidol to control the hallucinations. What is the most critical concern with this plan?
A. Haloperidol is only licensed for schizophrenia and cannot be used off-label in dementia
B. This clinical picture is most consistent with Lewy body dementia, in which typical antipsychotics including haloperidol can cause severe neuroleptic sensitivity reactions including acute parkinsonism, profound sedation, and neuroleptic malignant syndrome
C. Haloperidol will cause irreversible worsening of the memory impairment through its anticholinergic mechanism
D. The hallucinations are most likely caused by undiagnosed psychosis requiring psychiatric admission
Reveal Answer
Answer: B. This clinical picture is most consistent with Lewy body dementia, in which typical antipsychotics including haloperidol can cause severe neuroleptic sensitivity reactions including acute parkinsonism, profound sedation, and neuroleptic malignant syndrome
The triad of fluctuating cognition, recurrent well-formed visual hallucinations, and parkinsonism within 12 months of cognitive onset is the clinical picture of Lewy body dementia (DLB). Neuroleptic sensitivity is a defining feature of DLB — typical antipsychotics (haloperidol, chlorpromazine) and some atypical agents (risperidone) can precipitate acute severe parkinsonism, profound and irreversible sedation, and neuroleptic malignant syndrome with potentially fatal outcome. Cholinesterase inhibitors (rivastigmine) are first-line for hallucinations in DLB. If an antipsychotic is unavoidable, quetiapine at the lowest dose is the least contraindicated. Haloperidol is not primarily anticholinergic; its problem in DLB is dopamine D2 blockade in an already dopamine-deficient system.
Depression and Personality Change in the Elderly
Depression in the elderly (geriatric depression) is the most prevalent psychiatric disorder in older adults and the most potentially treatable, yet it remains significantly under-recognised and undertreated. The prevalence is approximately 8–15% in community-dwelling elderly and up to 25–35% in hospitalised elderly. Several factors contribute to under-recognition: clinicians (and patients themselves) may attribute depressive symptoms to 'normal ageing' or to the expected consequences of chronic illness; elderly patients more commonly present with somatic symptoms (fatigue, pain, appetite loss, sleep disturbance) than with the classical mood complaint of sadness or tearfulness; and the co-occurrence of dementia or delirium can mask depressive symptoms. The clinical entity of pseudodementia — where severe depression produces apparent cognitive impairment including memory loss, slowed information processing, and poor concentration — can be challenging to distinguish from early dementia; however, the key features pointing to depression are: mood change preceding cognitive symptoms; the patient complaining of memory problems (whereas in early dementia, the patient often minimises deficits while the family reports them); improvement in cognition with antidepressant treatment.
The Geriatric Depression Scale (GDS) — validated specifically for the elderly by avoiding somatic items that overlap with physical illness — is the recommended screening instrument. The 15-item short version uses yes/no responses for ease in elderly patients with mild cognitive impairment. A score ≥5/15 indicates probable depression; ≥10/15 indicates severe depression. Assessment must include enquiry about suicide risk — elderly males are at highest risk of completed suicide among all demographic groups; suicide in elderly often follows a first and only attempt after detailed planning, unlike the impulsive polyattempts more common in younger patients. A direct question about suicidal ideation is not contraindicated and should always be asked.
The DSM-5 criteria for major depressive episode require ≥5 of the following for ≥2 weeks, with at least one of the first two present: (1) depressed mood most of the day, nearly every day; (2) markedly diminished interest/pleasure in activities (anhedonia); (3) significant weight loss or gain / change in appetite; (4) insomnia or hypersomnia; (5) psychomotor agitation or retardation; (6) fatigue or loss of energy; (7) feelings of worthlessness or excessive guilt; (8) difficulty concentrating; (9) recurrent thoughts of death or suicidal ideation. In the elderly, criteria (3) and (4) are common as somatic symptoms of concurrent physical illness, requiring clinical judgement about attributing them to depression versus physical disease.
Management of geriatric depression: First-line pharmacological treatment is an SSRI — sertraline (25–50 mg/day start, maximum 100 mg/day) or escitalopram (5–10 mg/day start, maximum 20 mg/day) are preferred in the elderly because of favourable side-effect profiles and minimal anticholinergic, sedative, and cardiac effects. SNRIs (venlafaxine, duloxetine) are second-line. Avoid tricyclic antidepressants (TCAs) in the elderly: anticholinergic burden (constipation, urinary retention, dry mouth, cognitive impairment, delirium), orthostatic hypotension (fall risk), and cardiac conduction effects (QTc prolongation) — TCAs are listed in both STOPP and Beers criteria as potentially inappropriate in the elderly. Psychotherapy — cognitive behavioural therapy (CBT) and problem-solving therapy — have strong evidence in geriatric depression and are equally effective to pharmacotherapy for mild-to-moderate depression, with longer-lasting effects and no drug side effects. Electroconvulsive therapy (ECT) has the highest response rates of any treatment for severe, psychotic, or treatment-resistant depression in the elderly and should not be withheld based on age alone.
Personality changes in the elderly: Clinically significant personality change in the elderly is usually organic (secondary to neurological disease) rather than true primary personality disorder, which typically develops in young adulthood and does not de novo appear in old age. The most important causes are: frontal lobe degeneration (frontotemporal dementia — disinhibition, loss of empathy, stereotyped behaviour, as described in the dementia section); vascular lesions in the prefrontal cortex (following frontal lobe infarcts); Parkinson disease (apathy and social withdrawal as neuropsychiatric features); and subcortical dementia (Huntington disease, progressive supranuclear palsy). Management focuses on identifying and treating the underlying cause, supporting caregivers, and using non-pharmacological behavioural strategies; pharmacological intervention (SSRIs for affective features, low-dose antipsychotics for disinhibited or aggressive behaviour) is adjunctive.
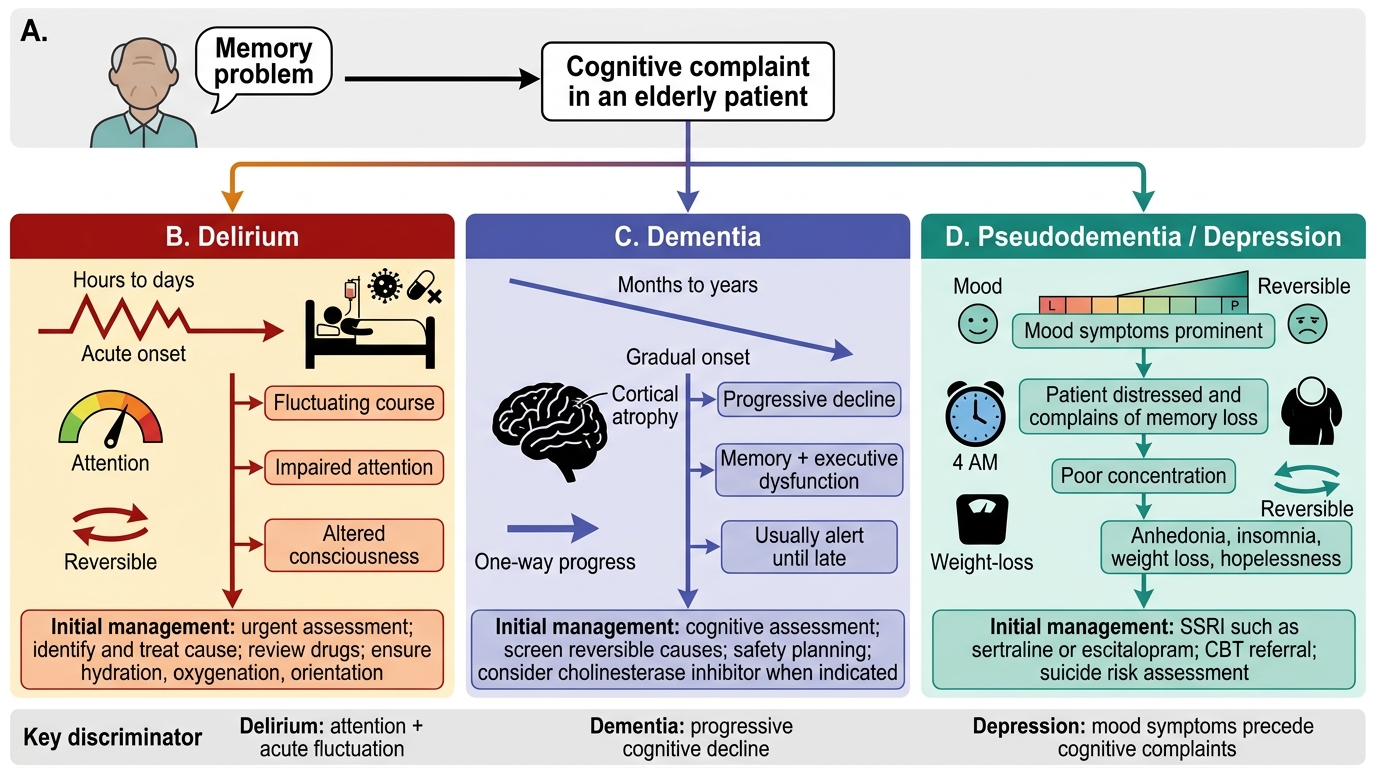
Cognitive Complaints in Older Adults: Three-Way Diagnostic Pathway
SELF-CHECK
An 81-year-old retired professor presents reporting that his memory has 'gone completely.' He is distressed, complains of poor concentration, wakes at 4 AM unable to return to sleep, has lost 5 kg, and reports no pleasure in his lifelong passion for books. His wife says he keeps saying 'there is no point anymore.' His MMSE is 22/30. What is the MOST LIKELY diagnosis and first-line treatment?
A. Alzheimer dementia — start donepezil 5 mg at bedtime
B. Delirium — investigate for acute precipitating cause
C. Geriatric depression with pseudodementia — start SSRI (sertraline or escitalopram) and refer for cognitive behavioural therapy
D. Lewy body dementia — start rivastigmine
Reveal Answer
Answer: C. Geriatric depression with pseudodementia — start SSRI (sertraline or escitalopram) and refer for cognitive behavioural therapy
This presentation is a classic pattern of pseudodementia (depression presenting as cognitive impairment): the patient himself is distressed and complains loudly about memory problems (unlike early Alzheimer, where patients often minimise deficits); mood symptoms (anhedonia, insomnia, weight loss, worthlessness) precede or co-dominate the picture; MMSE is mildly reduced but not severely impaired. The statement 'no point anymore' and weight loss signal significant depressive illness with possible suicidal ideation — enquire directly. First-line: SSRI (sertraline 25–50 mg) plus psychotherapy referral. If depression responds, cognition often improves substantially. Donepezil would be premature without excluding reversible causes. Delirium requires acute onset and inattention as cardinal features.
Self-Assessment: Applying Neuropsychiatric Diagnosis in Clinical Scenarios
The clinical scenarios below require you to apply the diagnostic frameworks from this module — delirium vs dementia vs depression; Alzheimer vs Lewy body vs vascular vs frontotemporal dementia — to arrive at a diagnosis and management priority. These reflect the NMC KH-level expectations: not just knowing the criteria but applying them to a patient encounter.
Scenario A: Mr Krishnan, 79 years old, is brought to the emergency department by his wife who says: 'For the past 24 hours he has been seeing things — small animals on the bedsheets — and is very restless. Yesterday he was perfectly fine.' Past history: type 2 diabetes (on metformin and glibenclamide), hypertension, prostate enlargement (on tamsulosin and solifenacin). Blood glucose on arrival: 2.1 mmol/L (38 mg/dL). What is the most likely diagnosis and what was the likely precipitant?
Analysis: Acute delirium (hyperactive subtype) — acute onset (24 hours), fluctuating course, visual hallucinations, agitation. CAM would be positive. The precipitant: hypoglycaemia from the long-acting sulphonylurea glibenclamide (a STOPP criterion — high risk in elderly diabetics). Secondary note: solifenacin (bladder antimuscarinic) is anticholinergic and should be reviewed as a contributing factor to delirium risk. Management: correct hypoglycaemia immediately (IV dextrose), switch from glibenclamide to a safer anti-diabetic agent, review solifenacin, non-pharmacological delirium care bundle.
Scenario B: Mr Sundarajan, 72 years old, presents with a 3-year history of gradual memory decline. He gets lost in familiar streets, has stopped managing his bank account (IADL impaired), and has begun accusing his wife of stealing (paranoid ideation). He does not recognise his granddaughter's new husband. His wife says he is 'the same person emotionally — still kind and gentle.' Neurological examination is normal (no parkinsonism, no focal signs). MRI brain shows generalised cerebral atrophy with hippocampal predominance. MMSE 18/30. What is the diagnosis and pharmacological management?
Analysis: Alzheimer dementia (moderate severity) — insidious onset, memory-first progression, hippocampal atrophy on MRI, intact personality (personality preservation is typical of AD in distinction to FTD), MMSE 18 = moderate. Management: AChEI (donepezil 10 mg/day or rivastigmine) plus memantine (appropriate for moderate AD, MMSE <20). BPSD (paranoid ideation): non-pharmacological first (reassurance, structured routine); if distressing, low-dose atypical antipsychotic (risperidone 0.25 mg) with explicit caregiver consent regarding black-box mortality risk.
Scenario C: Mrs Leela, 84 years old, has been residing in an old age home for 2 years since her husband died. Staff report she has 'given up' — she stays in bed most of the day, refuses meals, does not participate in activities she previously enjoyed (reading, chess), and has told another resident 'I don't want to live anymore.' Staff assumed this was normal grief. Her MMSE is 26/30. What is the most important action?
Analysis: Geriatric depression with active suicidal ideation — GDS should be administered (would likely score ≥10); the statement 'I don't want to live anymore' requires direct assessment of suicide intent and plan. Social isolation (institutionalised, widowed, no family contact) is a major risk factor. The assumption that this is 'normal grief' two years after bereavement is incorrect — prolonged functional impairment and suicidal ideation are not normal. Immediate action: psychiatry or geriatric medicine referral for suicide risk assessment, SSRI initiation (escitalopram 5 mg, titrate slowly), CBT referral, social engagement programme within the care home, arrange family involvement.
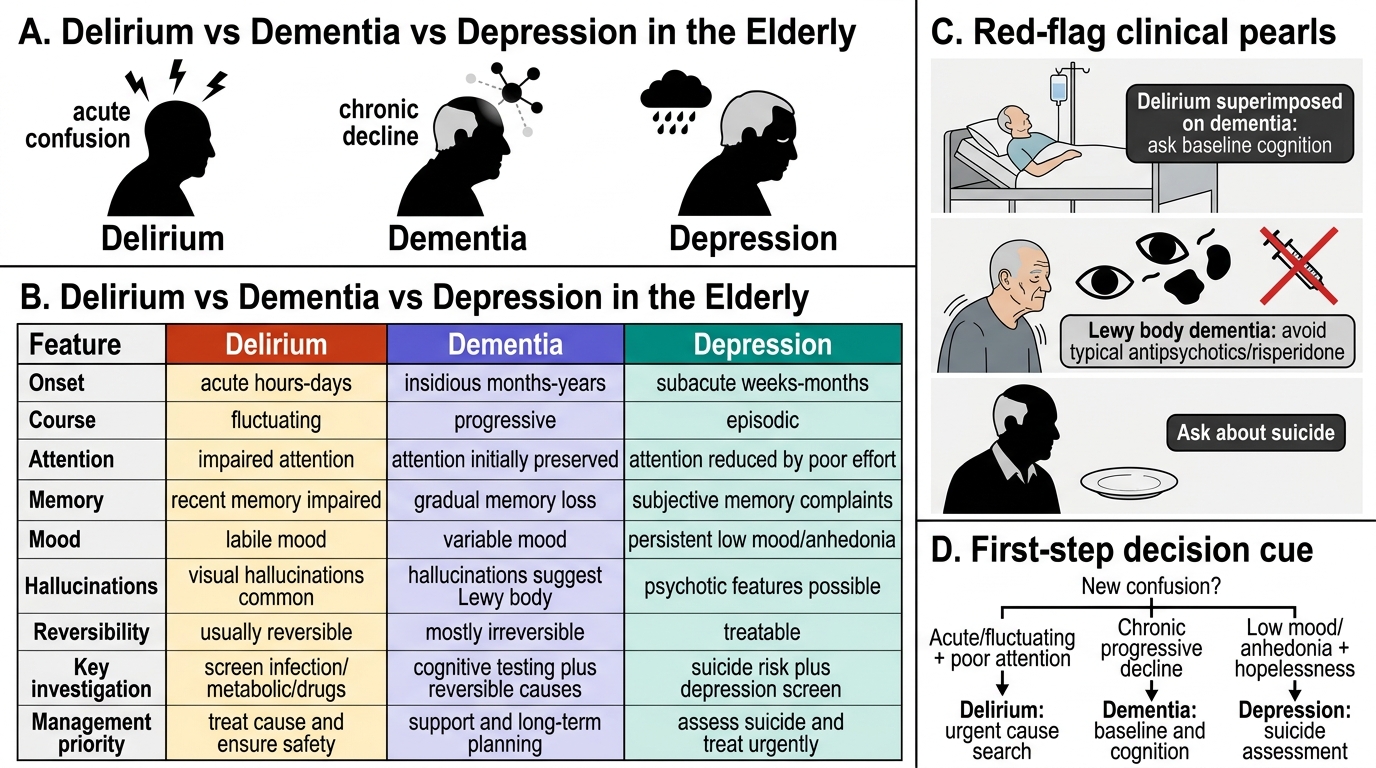
Delirium vs Dementia vs Depression in the Elderly
CLINICAL PEARL
Three pearls that prevent the most common geriatric neuropsychiatric errors: (1) The three Ds can coexist and mask each other. Delirium superimposed on dementia is the most common inpatient geriatric neuropsychiatric scenario; dementia is the single greatest risk factor for delirium. Resolving the delirium will not 'cure' the dementia, but it will restore the patient's baseline (which may itself be cognitively impaired). Always ask: 'What is this patient's cognitive baseline before this acute illness?' (2) Visual hallucinations in an elderly patient with parkinsonism = Lewy body dementia until proven otherwise — do NOT start a typical antipsychotic or risperidone. The neuroleptic sensitivity reaction can be fatal. Start rivastigmine, maintain orientation, and if absolutely necessary for safety use quetiapine at the lowest dose. (3) An 81-year-old man who suddenly loses interest in everything, stops eating, and says 'there is no point' has depression — not 'normal ageing' — until proven otherwise. Elderly males are the highest-risk demographic for completed suicide. Always ask directly, refer promptly, and treat effectively.