Page 22 of 35
IM26.26-27 | Fungal Infections: Candidiasis and Aspergillosis — SDL Guide
Learning Objectives
- Describe the common causes, etiopathogenesis, clinical features, diagnosis, and management of candidiasis including oropharyngeal, oesophageal, vulvovaginal, and invasive candidiasis
- Describe the etiopathogenesis, clinical features, diagnosis, and management of aspergillosis including allergic bronchopulmonary aspergillosis (ABPA), chronic pulmonary aspergillosis (CPA), and invasive pulmonary aspergillosis (IPA)
INSTRUCTIONS
Fungal infections are among the most important cause of morbidity and mortality in immunocompromised patients in India — their incidence has risen sharply with the expanding populations of HIV-positive patients, solid organ and haematopoietic stem cell transplant recipients, patients receiving prolonged corticosteroid or biological agent therapy, and critically ill ICU patients. The two organisms covered in this SDL — Candida and Aspergillus — are responsible for the vast majority of life-threatening fungal infections encountered in Indian general medicine and ICU practice. The COVID-19 pandemic introduced a new context for fungal disease in India: COVID-19-associated mucormycosis (CAM) became a national epidemic, underscoring the importance of immune risk factor recognition.
References
- Harrison's Principles of Internal Medicine, 21st ed., Ch. 211 — Candidiasis; Ch. 213 — Aspergillosis (textbook)
- API Textbook of Medicine, 10th ed., Section 7 — Infectious Diseases (Fungal Infections chapter) (textbook)
- ISHAM/ESCMID Guidelines for Invasive Candidiasis and Aspergillosis; IDSA Candidiasis Guidelines 2016 (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Three patients present in a single week to a general medicine ward. The first: a 28-year-old HIV-positive man with CD4 count of 45 cells/µL with white plaques coating his tongue and soft palate, dysphagia for solids and liquids, and odynophagia — he has lost 7 kg in 6 weeks. The second: a 58-year-old man with acute myeloid leukaemia (AML) post-induction chemotherapy, now on day 14 of profound neutropenia (ANC <100/µL), developing new fever despite 5 days of broad-spectrum antibiotics (piperacillin-tazobactam + vancomycin); HRCT chest shows a 3.2 cm right upper lobe nodule with a surrounding halo of ground-glass opacity. The third: a 34-year-old asthmatic with worsening wheeze, eosinophilia (1,800/µL), total IgE 1,800 IU/mL, and a CXR showing bilateral fleeting migratory infiltrates with central bronchiectasis. These three patients illustrate the three faces of Aspergillus/Candida: mucocutaneous candidiasis in advanced HIV, invasive pulmonary aspergillosis in haematological malignancy, and allergic bronchopulmonary aspergillosis in an immunocompetent asthmatic. Three different immune contexts, three different diseases, three different management strategies — all caused by ubiquitous fungi that are harmless in the healthy host but lethal or severely morbid in the compromised host.
WHY THIS MATTERS
Fungal infections present a growing challenge in Indian clinical practice for several interconnected reasons. The population at risk for invasive fungal disease has expanded dramatically: India has the world's third-largest HIV-positive population; transplant programmes at major centres have grown rapidly; broad-spectrum antibiotic usage in ICUs creates the ecological vacuum that allows Candida to proliferate; and long-term corticosteroid use — for asthma, autoimmune disease, and post-COVID inflammatory syndrome — predisposes to both Aspergillus and Candida infections. The COVID-19 pandemic exposed a new population at risk: COVID-19-associated pulmonary aspergillosis (CAPA) and COVID-19-associated mucormycosis (CAM) became epidemic in India in 2021, with over 40,000 cases of mucormycosis (the 'black fungus') reported nationally in the second wave. Distinguishing fungal infection from bacterial infection or malignancy — and recognising the correct risk factor profile — is the core clinical skill that drives the diagnostic and therapeutic decisions covered in this SDL.
RECALL
Recall the relevant mycology before proceeding. Candida is a dimorphic fungus — existing as yeast (blastoconidia) in culture and blood, but forming pseudohyphae and true hyphae in tissues when it invades (the morphological switch from yeast to hyphae correlates with pathogenicity). C. albicans is the most common species (~50% of invasive candidiasis), but non-albicans Candida species — C. glabrata, C. krusei, C. tropicalis, C. parapsilosis — are increasingly common, clinically important because several are intrinsically resistant to fluconazole. Aspergillus is a ubiquitous mould (filamentous fungus) found in soil, decaying organic matter, and building construction dust; A. fumigatus is the most common pathogenic species, producing small airborne conidia (2–3 µm) that are continuously inhaled but efficiently cleared by normal mucociliary and phagocytic defences. Disease occurs when immune defences fail (neutropenia, corticosteroid use), when the organism triggers an exaggerated immune response (ABPA), or when it colonises pre-existing lung cavities (CPA).
Candidiasis: Mucocutaneous and Invasive Forms
Candidiasis is infection caused by Candida species, with a spectrum ranging from superficial mucocutaneous disease (oropharyngeal thrush, vulvovaginal candidiasis) to life-threatening invasive candidiasis (candidaemia and disseminated candidiasis). The clinical form depends entirely on the host immune status: in immunocompetent individuals, Candida causes only mucocutaneous disease, typically in localised settings of disrupted epithelial barrier (antibiotic-associated oral thrush, moisture-associated intertrigo) or hormonal change (vulvovaginal candidiasis during pregnancy or with antibiotic use). In immunocompromised hosts, Candida becomes an invasive, life-threatening pathogen. Understanding which patients are at risk for progression from mucocutaneous colonisation to invasive disease is the key clinical decision that determines whether antifungal treatment needs to be topical or systemic, empirical or targeted, and outpatient or inpatient in intensity.
Risk factors for invasive candidiasis:
- Neutropenia (absolute neutrophil count <500/µL), particularly in haematological malignancy
- Prolonged broad-spectrum antibiotic therapy (>5 days) — eliminates bacterial flora, allowing Candida overgrowth
- Central venous catheter (CVC) — Candida forms robust biofilm on catheter surfaces; CVC removal is essential in treating candidaemia
- ICU admission, particularly post-abdominal surgery (especially GI perforation or anastomotic leak — disrupts gut barrier, allows Candida translocation)
- Total parenteral nutrition (TPN) — glucose-rich substrate promotes Candida growth
- Prolonged corticosteroid or immunosuppressive therapy
- HIV with CD4 <200 cells/µL
Clinical forms of candidiasis:
1. Oropharyngeal candidiasis (OPC / thrush): white curd-like plaques on the buccal mucosa, tongue, palate, and pharynx — easily scraped off, leaving an erythematous, sometimes bleeding base (distinguishing from oral leukoplakia which cannot be scraped off). Associated with burning and altered taste. Common in HIV (CD4 <200), neonates, patients on inhaled corticosteroids (improper technique — not rinsing mouth after use), patients on antibiotics, denture wearers. Treat: clotrimazole troches 10 mg 5×/day × 7–14 days (topical, first-line for mild disease) or oral fluconazole 200 mg loading, then 100 mg daily × 7 days (systemic, for moderate-severe or refractory disease).
2. Oesophageal candidiasis: extension of OPC into the oesophagus; signifies significant immune compromise — in HIV, defines AIDS (CD4 typically <50–100 cells/µL). Classic presentation: odynophagia (pain on swallowing — more severe than dysphagia) and dysphagia. White plaques or erosions on oesophagoscopy (confirming diagnosis); distinguished from CMV oesophagitis (large shallow ulcers) and HSV oesophagitis (vesicles/small ulcers). Treat: systemic fluconazole 400 mg loading then 200 mg daily × 14–21 days; not curable with topical agents (not reaching oesophageal mucosa adequately). Fluconazole resistance: switch to voriconazole or IV echinocandin (caspofungin, micafungin).
3. Vulvovaginal candidiasis (VVC): 75% of women experience at least one episode; most common cause of vaginitis after bacterial vaginosis. Symptoms: intense pruritus, white 'cottage cheese' discharge, dysuria, erythema. Diagnosis: wet mount KOH preparation showing pseudohyphae + spores (yeast forms). Predisposing factors: pregnancy, diabetes, antibiotics, oral contraceptives, immunosuppression. Treat: topical clotrimazole cream × 3–7 days (first-line uncomplicated) or oral fluconazole 150 mg single dose. Recurrent VVC (≥4 episodes/year): weekly fluconazole 150 mg maintenance for 6 months.
4. Invasive candidiasis (IC) / Candidaemia: the most serious form — bloodstream infection with multi-organ dissemination. Candidaemia (Candida in blood cultures) is associated with 30-day mortality of 30–50% in ICU patients, even with appropriate antifungal therapy. Clinical presentation: fever + fungaemia in an at-risk patient — no specific clinical features, making the diagnosis dependent on blood cultures. Complications of disseminated candidiasis: Candida endophthalmitis (retinal lesions — every patient with candidaemia should have a dilated fundal examination; affects 5–10% of candidaemia patients; requires extended antifungal therapy and sometimes intravitreal treatment); Candida endocarditis (high vegetation rate on prosthetic valves; most common fungal endocarditis — mortality >50%); hepatosplenic candidiasis (in neutropenic patients recovering from chemotherapy — fever + elevated ALP + multiple microabscesses on imaging).
Treatment of invasive candidiasis: echinocandins are the preferred first-line agents — caspofungin, micafungin, or anidulafungin (fungicidal against Candida, excellent biofilm activity, minimal nephrotoxicity); fluconazole acceptable in stable, non-critically ill patients with confirmed fluconazole-susceptible Candida (NOT for initial empirical therapy in ICU-acquired candidaemia). CVC removal is mandated in all cases of candidaemia — significantly reduces mortality and time to clearance. Duration: at least 14 days from the first negative blood culture.
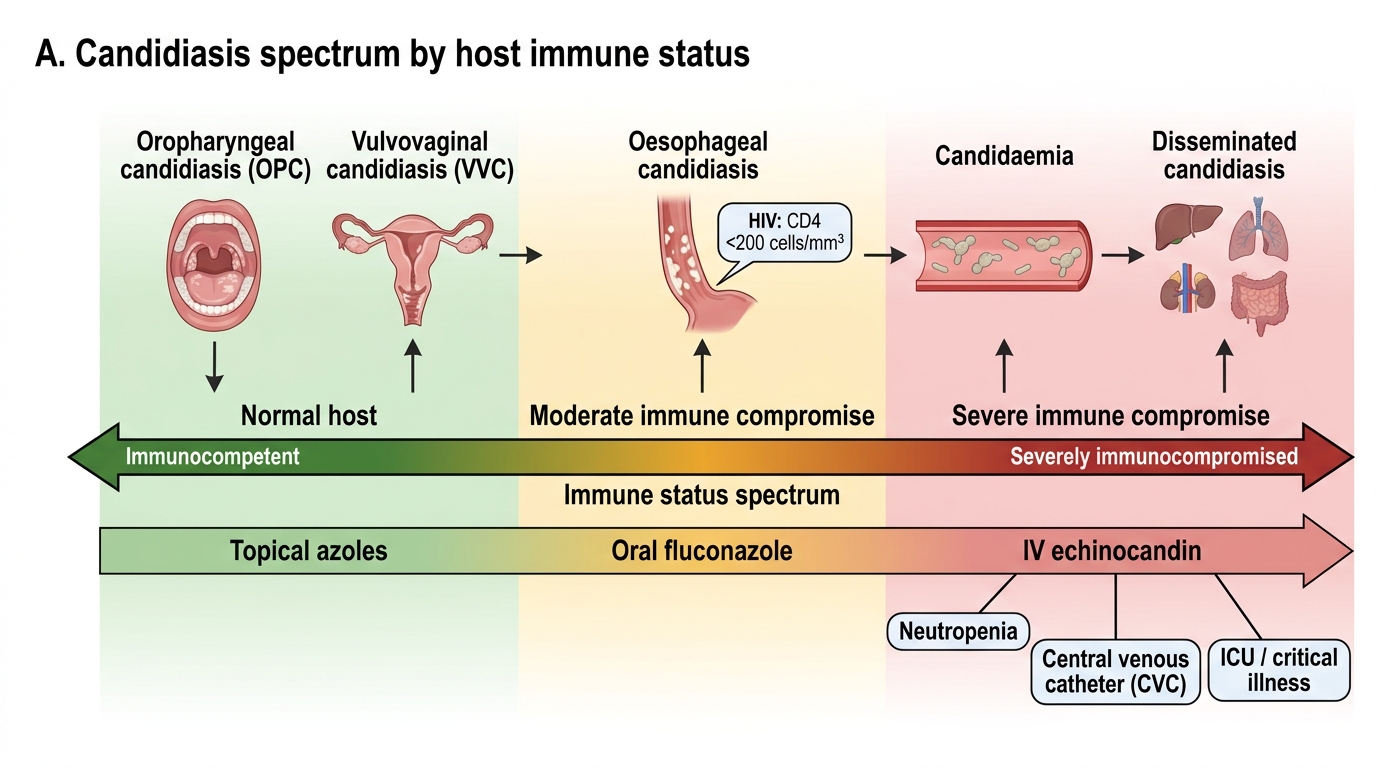
Candidiasis Spectrum by Immune Status
SELF-CHECK
A 45-year-old ICU patient post-bowel resection for perforated sigmoid diverticulitis has been on meropenem + metronidazole for 8 days when he develops new fever (39.2°C). Blood cultures drawn at 48 hours grow Candida albicans. He has a central venous catheter (CVC) in place. What is the MOST critical immediate step in management alongside starting antifungal therapy?
A. Continue the CVC and add amphotericin B — the CVC is needed for continued antibiotic administration
B. Remove the CVC immediately — Candida biofilm on the catheter is the likely source and continued candidaemia with CVC in place significantly worsens mortality
C. Switch antibiotics to broaden bacterial coverage before starting antifungal therapy
D. Start oral fluconazole — it is adequate for C. albicans candidaemia in ICU patients
Reveal Answer
Answer: B. Remove the CVC immediately — Candida biofilm on the catheter is the likely source and continued candidaemia with CVC in place significantly worsens mortality
CVC removal is the single most critical intervention in candidaemia — Candida forms robust biofilm on catheter surfaces that antifungal drugs penetrate poorly; the catheter is both the source and the sanctuary of the infection. Continued candidaemia with a CVC in place is a major predictor of mortality and failure to clear the bloodstream. A new CVC should be inserted at a different site if IV access is needed. Start IV echinocandin (caspofungin, micafungin, or anidulafungin) as first-line in ICU candidaemia — NOT oral fluconazole (inadequate in critically ill patients, not first-line for empirical therapy where fluconazole susceptibility is unknown). Amphotericin B is reserved for refractory/resistant cases due to nephrotoxicity.
Aspergillosis: ABPA, Chronic Pulmonary Aspergillosis, and Invasive Aspergillosis
Aspergillosis encompasses a spectrum of pulmonary and disseminated diseases caused by Aspergillus species — most commonly A. fumigatus. Unlike Candida (which causes disease across a spectrum of immune states), Aspergillus disease presentation is almost entirely determined by the immune context of the host: hypersensitivity/allergic disease (ABPA) in patients with atopic asthma or cystic fibrosis who have exaggerated immune responses to Aspergillus antigens; chronic low-grade infection (CPA) in patients with prior lung cavities (post-TB, COPD) who are mildly immunocompromised; and acute, angio-invasive infection (IPA) in severely immunocompromised patients (neutropenia, high-dose corticosteroids, transplant).
1. Allergic Bronchopulmonary Aspergillosis (ABPA):
ABPA is a hypersensitivity reaction to inhaled Aspergillus antigens (predominantly A. fumigatus) occurring in patients with asthma or cystic fibrosis — not an infection per se, but an exaggerated immune response. The pathological sequence: sensitisation to Aspergillus antigens → massive IgE production (total IgE markedly elevated, typically >1,000 IU/mL) + Aspergillus-specific IgE/IgG → type I (immediate) and type III (immune complex) hypersensitivity reactions → airway inflammation, mucous plugging, and eventually bronchiectasis and pulmonary fibrosis if untreated.
Clinical features of ABPA: wheezing and asthma (difficult to control), expectoration of brownish mucous plugs (containing Aspergillus hyphae — pathognomonic if present), recurrent fleeting pulmonary infiltrates (migratory, bilateral), haemoptysis, low-grade fever. A key radiological feature: central bronchiectasis (dilated bronchi in the central lung fields — the opposite of usual peripheral post-infectious bronchiectasis) caused by chronic mucous plugging and wall damage. Eosinophilia (blood eosinophils >500/µL, often much higher) is characteristic. ABPA in cystic fibrosis is an important complication that accelerates pulmonary decline.
Diagnosis (ISHAM 2013 criteria — any patient with asthma/CF + 2 or more of): total IgE >1,000 IU/mL; positive Aspergillus skin prick test or elevated Aspergillus-specific serum IgE; elevated Aspergillus-specific precipitating IgG; CT features of ABPA (central bronchiectasis, mucoid impaction, high-attenuation mucus plugs — pathognomonic).
Treatment of ABPA: oral prednisolone (0.5 mg/kg/day × 2 weeks, then taper) is the primary treatment — reduces the inflammatory response and prevents progressive bronchiectasis. Itraconazole (200 mg twice daily × 4–6 months) is added as adjunctive antifungal therapy — reduces Aspergillus antigen load in the airway, reduces corticosteroid requirement, reduces exacerbations (randomised trial evidence). Voriconazole is an alternative azole where itraconazole is not tolerated.
2. Chronic Pulmonary Aspergillosis (CPA):
CPA occurs in patients with pre-existing pulmonary cavities (most commonly post-TB cavities in India — CPA complicates 15–20% of healed TB cavities), often with mild immune compromise (COPD, malnutrition, mild corticosteroid use, diabetes). Aspergillus colonises the cavity and may form an aspergilloma — a fungus ball (mass of tangled Aspergillus hyphae, mucus, and inflammatory debris) sitting freely within a cavity. The fungal ball moves within the cavity (demonstrated by positional CT scanning). Clinical features: chronic cough, recurrent haemoptysis (sometimes massive), weight loss, fatigue — the presentation closely mimics active TB or lung malignancy. Diagnosis: CT chest (cavity + aspergilloma — 'bell sign' of meniscus of air above the fungal ball); Aspergillus IgG antibodies (elevated — useful serum marker); sputum culture for Aspergillus (positive in ~50%). Massive haemoptysis is the most dangerous complication — managed urgently with bronchial artery embolisation; surgical resection of the cavity is the definitive treatment (if feasible).
Treatment: for simple aspergilloma (single cavity, stable) — observation; antifungals do not penetrate the aspergilloma effectively. For CPA with progressive disease or recurrent haemoptysis: long-term voriconazole (200 mg twice daily) or itraconazole (200 mg twice daily) — extended courses (months to years); surgical resection when feasible.
3. Invasive Pulmonary Aspergillosis (IPA):
IPA is the most feared form — angio-invasive infection in severely immunocompromised hosts where Aspergillus hyphae invade blood vessel walls, causing thrombosis, infarction, and haematogenous dissemination. The highest risk groups: haematological malignancy post-induction chemotherapy (prolonged neutropenia — ANC <100/µL for >10 days); allogeneic haematopoietic stem cell transplant (HSCT) recipients; solid organ transplant on intense immunosuppression; patients on prolonged high-dose corticosteroids (≥3 mg/kg prednisolone equivalent for >3 weeks); and — critically — patients with severe COVID-19 (COVID-19-associated pulmonary aspergillosis, CAPA — an increasingly recognised entity that markedly worsens prognosis).
Clinical features of IPA: new fever despite broad-spectrum antibiotics in a neutropenic patient; new pulmonary infiltrates on CT (the CT pattern is highly specific — see below); pleuritic chest pain (from infarction); haemoptysis (from vascular invasion). Characteristic CT signs of IPA: (a) 'halo sign' — a nodule surrounded by a halo of ground-glass opacity (represents the zone of haemorrhage around the infarcted nodule — pathognomonic of angio-invasive fungal infection, though not entirely specific for Aspergillus); (b) 'air-crescent sign' — a crescent of air within a nodule or cavity, appearing during immune reconstitution (neutrophil recovery) as the necrotic centre liquefies — indicates disease response.
Diagnosis of IPA: HRCT chest is the primary diagnostic tool in high-risk patients (halo sign + clinical context is highly predictive). Serum galactomannan (a polysaccharide component of the Aspergillus cell wall) — ELISA; sensitivity 70–80% in neutropenic patients, lower in solid organ transplant or corticosteroid-treated patients; false positives with piperacillin-tazobactam (important in ICU patients). BAL galactomannan (higher sensitivity than serum in non-neutropenic patients). Beta-D-glucan (serum) — a pan-fungal biomarker (positive in Candida and Aspergillus but not mucormycosis). Culture of BAL or tissue biopsy — gold standard but often not feasible in neutropenic patients (thrombocytopenia).
Treatment of IPA: voriconazole (IV/oral, dose: 6 mg/kg 12-hourly day 1 loading, then 4 mg/kg 12-hourly) is the gold standard first-line agent — superior to amphotericin B in landmark RCT (IDSA). Alternative: isavuconazole (fewer drug interactions, better tolerated). Combination therapy (voriconazole + echinocandin) for salvage. Duration: minimum 6–12 weeks; until immunosuppression resolves. Mortality: 50–90% in neutropenic hosts with IPA despite treatment — emphasising the importance of early antifungal prophylaxis in high-risk haematology patients (posaconazole 300 mg daily is standard prophylaxis in AML patients during remission-induction chemotherapy).
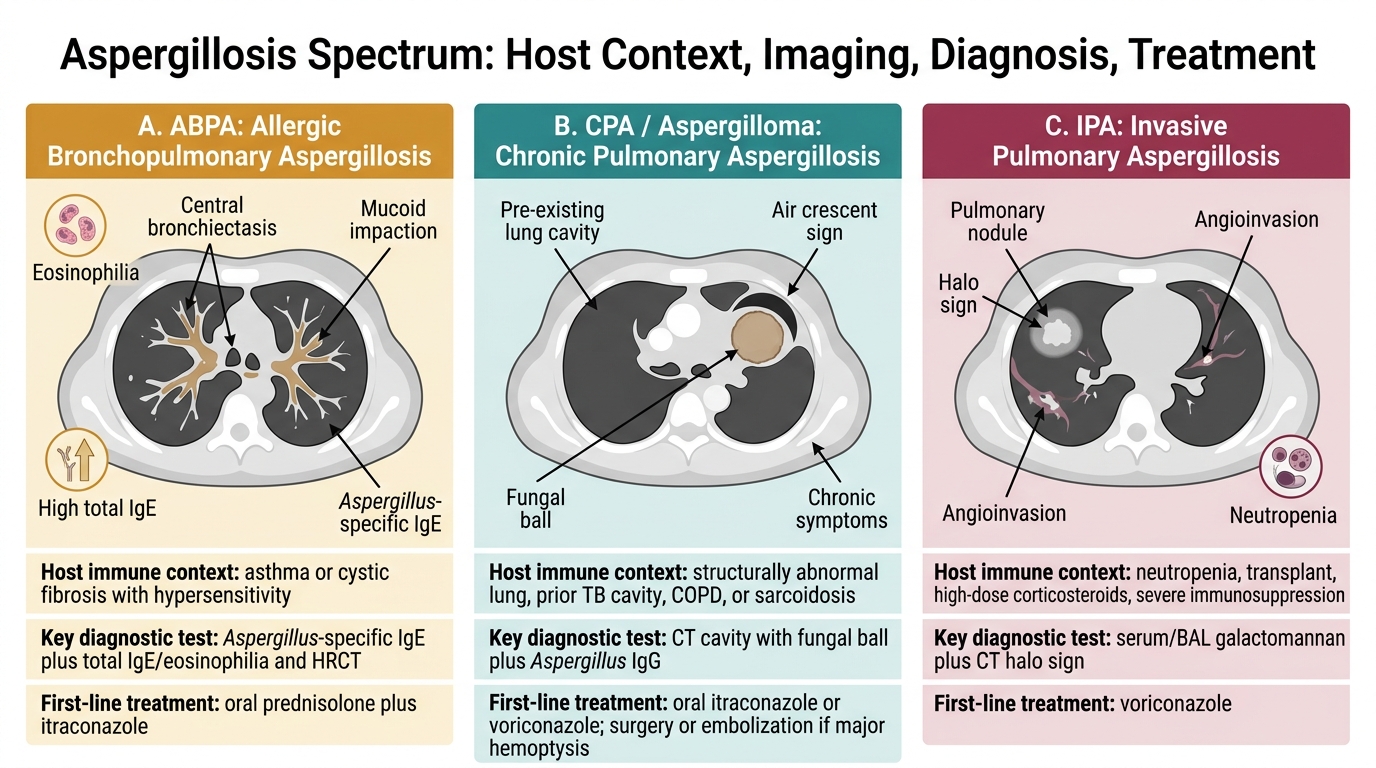
Aspergillosis Clinical Spectrum
SELF-CHECK
A 32-year-old asthmatic presents with 3 months of worsening wheeze, expectoration of brownish mucous plugs, and two episodes of pulmonary consolidation in the past year that cleared with antibiotics. Blood eosinophils: 1,600/µL. Total IgE: 2,200 IU/mL. HRCT chest: bilateral central bronchiectasis with mucoid impaction. Aspergillus-specific IgE is elevated. What is the correct treatment strategy?
A. IV amphotericin B — systemic fungicidal therapy is required because Aspergillus is invading the lungs
B. Oral prednisolone + itraconazole — ABPA requires corticosteroid to suppress hypersensitivity and adjunctive antifungal to reduce Aspergillus antigen load
C. Voriconazole monotherapy — oral antifungal is the primary treatment for ABPA
D. Surgical resection of the affected bronchial segments — mechanical removal of the bronchiectatic segments is the definitive treatment
Reveal Answer
Answer: B. Oral prednisolone + itraconazole — ABPA requires corticosteroid to suppress hypersensitivity and adjunctive antifungal to reduce Aspergillus antigen load
ABPA treatment is oral prednisolone (0.5 mg/kg/day × 2 weeks then taper) as the primary anti-inflammatory treatment, combined with adjunctive itraconazole (200 mg twice daily × 4–6 months). ABPA is a hypersensitivity disease, not an invasive fungal infection — it does not require IV amphotericin B (which is used for invasive/life-threatening fungal infections). Voriconazole is used for invasive aspergillosis; in ABPA, itraconazole is the preferred antifungal adjunct. Surgery is not indicated for ABPA; it is considered for CPA with aspergilloma or massive haemoptysis.
Diagnosis and Management of Fungal Infections: Laboratory Approach and Antifungal Agents
A systematic laboratory and imaging approach is required to diagnose fungal infections, particularly because their clinical presentations overlap with bacterial infections and malignancy. The laboratory diagnosis of invasive fungal infections relies on a combination of culture (gold standard but slow), non-culture biomarkers (galactomannan, beta-D-glucan — faster), histopathology (definitive), and radiology. Selecting the right diagnostic test requires knowing the fungal organism being considered, the immune state of the patient, and the phase of illness — because the sensitivity of each test varies substantially across these variables. Antifungal drug selection follows directly from the diagnostic conclusion and the host risk profile, and the major antifungal drug classes — azoles, echinocandins, and polyenes — differ fundamentally in mechanism, spectrum, and toxicity.
Provided image
Laboratory diagnosis — key tests:
| Test | Fungus detected | Key use | Limitations |
|---|---|---|---|
| Blood culture (Sabouraud/BACTEC) | Candida | Candidaemia | Sensitivity 50–70%; Aspergillus rarely grows in blood |
| KOH preparation | Any fungus | Rapid morphology from clinical specimens | Species identification requires culture |
| Serum galactomannan ELISA | Aspergillus | IPA in neutropenic patients | False positive with pip-tazo; less sensitive in non-neutropenic |
| Serum/BAL beta-D-glucan | Candida, Aspergillus (NOT Mucor) | Pan-fungal screening | Non-specific; does not detect mucormycosis |
| CT chest (HRCT) | Aspergillus indirect | IPA — halo sign, air crescent | Halo sign not 100% specific |
| India ink (CSF) | Cryptococcus | Cryptococcal meningitis | Not a Candida/Aspergillus test — included for completeness |
| Histopathology (GMS/PAS) | All fungi | Tissue invasion (definitive diagnosis) | Requires biopsy; risk in neutropenic/thrombocytopenic patients |
| Bronchoalveolar lavage (BAL) | Aspergillus/Candida | Respiratory fungal infection | Galactomannan + culture from BAL |
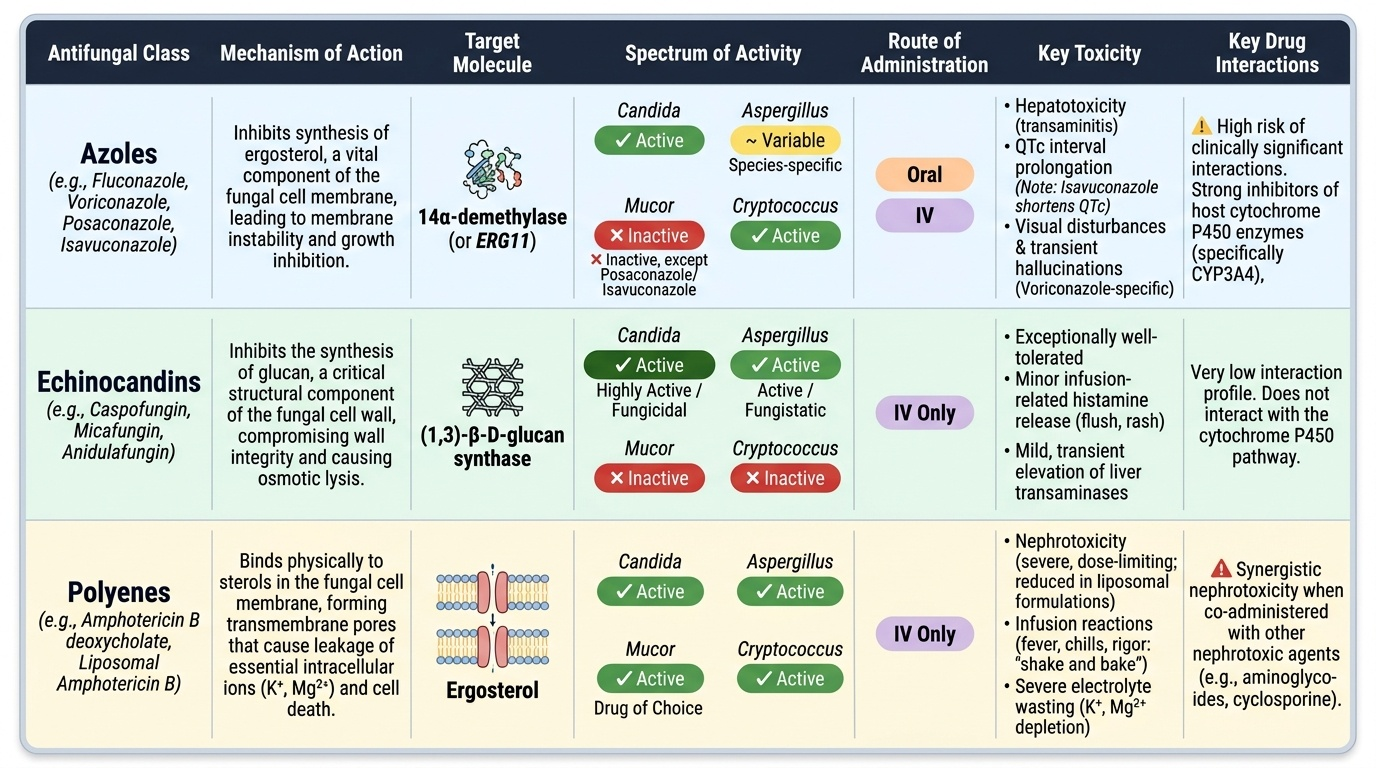
Antifungal drug classes — mechanism and spectrum:
Three major antifungal classes are used for invasive fungal infections:
1. Azoles (fluconazole, itraconazole, voriconazole, posaconazole, isavuconazole): mechanism = inhibition of ergosterol synthesis (target: lanosterol 14-α-demethylase, a cytochrome P450 enzyme); fungistatic against most organisms. Spectrum: fluconazole — Candida albicans but NOT C. krusei (intrinsically resistant) and often NOT C. glabrata (dose-dependent susceptibility); voriconazole — Aspergillus, fluconazole-resistant Candida; posaconazole — Aspergillus + Mucor (the only azole with Mucor activity). Key drug interactions: azoles are potent CYP3A4 inhibitors — significant interactions with immunosuppressants (ciclosporin, tacrolimus — levels increase 2–5-fold; dose reduction required), statins, warfarin, many antiretrovirals.
2. Echinocandins (caspofungin, micafungin, anidulafungin): mechanism = inhibition of (1,3)-beta-D-glucan synthase — disrupts the fungal cell wall (no human equivalent, hence minimal toxicity). Fungicidal against Candida; fungistatic against Aspergillus. First-line for invasive candidiasis; salvage for IPA. NOT effective against Cryptococcus or Mucor. IV only (no oral formulation). Excellent safety profile.
3. Polyenes (amphotericin B deoxycholate, liposomal amphotericin B — L-AmB): mechanism = binds ergosterol in the fungal cell membrane, forming pores → fungicidal. Broadest spectrum (Candida, Aspergillus, Mucor, Cryptococcus). Conventional amphotericin B: significant nephrotoxicity, infusion-related reactions; largely replaced by liposomal formulation (L-AmB). L-AmB: 3–5 mg/kg/day; much lower nephrotoxicity; drug of choice for mucormycosis in India (mucor is NOT covered by azoles other than posaconazole).
Treatment summary:
| Condition | First-line agent | Alternative |
|---|---|---|
| Oropharyngeal candidiasis | Clotrimazole troches / fluconazole 100 mg/day × 7d | Itraconazole |
| Oesophageal candidiasis | Fluconazole 200 mg/day × 14–21d | IV echinocandin |
| Invasive candidiasis/candidaemia | Echinocandin (caspofungin/micafungin) | Fluconazole (if susceptible, non-critically ill) |
| ABPA | Prednisolone 0.5 mg/kg/day + itraconazole × 4–6 mo | Voriconazole |
| CPA/aspergilloma (progressive) | Voriconazole 200 mg BD oral long-term | Itraconazole |
| IPA | Voriconazole IV/oral (loading 6 mg/kg BD, then 4 mg/kg BD) | Isavuconazole |
| Mucormycosis | Liposomal amphotericin B 3–5 mg/kg/day + debridement | Posaconazole (step-down) |