Page 23 of 35
IM26.26-27 | Fungal Infections: Candidiasis and Aspergillosis — SDL Guide (Part 2)
Self-Assessment: Fungal Infections
You have now covered the clinical spectrum of candidiasis and aspergillosis, from mucocutaneous disease through invasive life-threatening infection. The following scenarios apply the diagnostic and management principles across different immune contexts. Work through each before reading the analysis.
Provided image
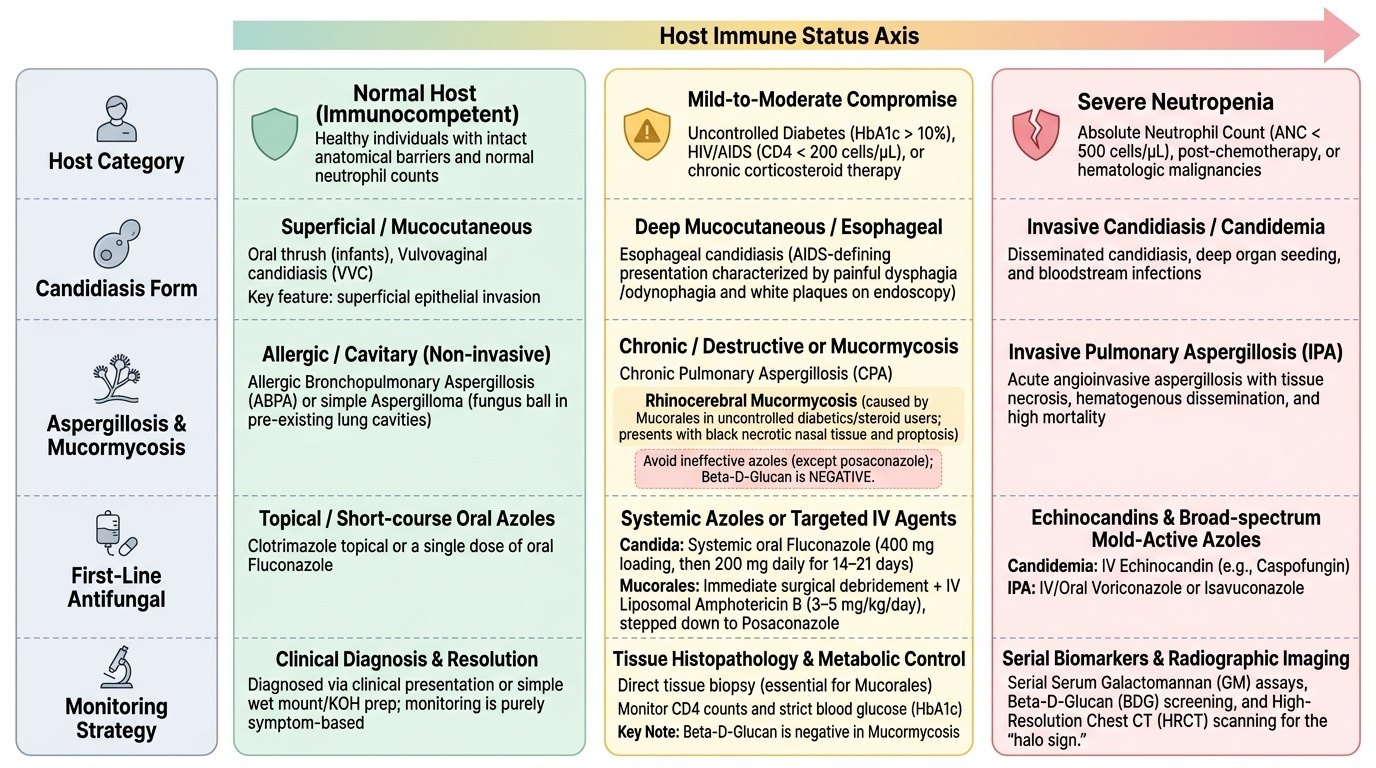
Scenario A: A 48-year-old male with T2DM on metformin, poorly controlled (HbA1c 10.8%), presents with a 5-day history of right-sided facial pain, nasal stuffiness, and progressive blurring of right vision. Examination reveals right-sided periorbital swelling, proptosis, and black necrotic tissue visible on rhinoscopy. Nasal biopsy pending.
Analysis: Black necrotic tissue in the nasal cavity/palate + periorbital involvement + poorly controlled diabetes = rhinocerebral mucormycosis (not candidasis or aspergillosis, but included here to contextualise the differential in severe fungal infection). Mucormycosis is caused by Mucorales — Rhizopus, Mucor, Lichtheimia — not Aspergillus. Treatment: immediate surgical debridement (extensive resection of necrotic tissue) + IV liposomal amphotericin B (3–5 mg/kg/day). Posaconazole is added after stabilisation. Mortality >50% without rapid surgical intervention. In India, mucormycosis disproportionately affects uncontrolled diabetics. The COVID-19 pandemic 2021 wave drove an epidemic of CAM — COVID-associated mucormycosis — principally from indiscriminate corticosteroid use causing hyperglycaemia and immune suppression. This scenario illustrates the critical importance of recognising mucormycosis as a distinct entity from candidiasis/aspergillosis — beta-D-glucan is NEGATIVE in mucormycosis (no beta-glucan in Mucorales cell walls), and azoles (other than posaconazole) are ineffective.
Scenario B: A 26-year-old HIV-positive woman with CD4 count of 68 cells/µL on antiretroviral therapy (started 4 weeks ago) presents with 2 weeks of worsening painful dysphagia and odynophagia. She has white plaques on her tongue that scrape off easily. Upper endoscopy shows white plaques and erosions extending throughout the oesophagus.
Analysis: HIV with low CD4 + oropharyngeal candidiasis + oesophageal involvement = oesophageal candidiasis (AIDS-defining illness). Treat with systemic fluconazole 400 mg loading then 200 mg daily × 14–21 days. Topical antifungals do not reach the oesophagus. Caveat: consider whether she is having IRIS (immune reconstitution inflammatory syndrome) given she started ART 4 weeks ago; candida IRIS typically presents with worsening mucocutaneous disease. Her ART should be continued. Secondary prophylaxis with weekly fluconazole is recommended if CD4 remains <50 cells/µL after this episode.
Scenario C: A 67-year-old male with a 30-year history of treated pulmonary TB (healed left upper lobe cavities on old CT) presents with 4 months of weight loss, evening sweats, chronic productive cough, and two episodes of haemoptysis. Sputum AFB smear ×3 is negative. Sputum culture for Aspergillus: positive. CT chest shows an 'old' cavity containing a soft tissue density mass with an air crescent above it. Serum Aspergillus IgG: elevated.
Analysis: Post-TB cavity + aspergilloma (fungal ball with air crescent on CT) + positive Aspergillus culture + elevated IgG = chronic pulmonary aspergillosis (CPA) with aspergilloma — one of the most clinically significant complications of healed TB in India. Haemoptysis is the main danger — bronchial artery embolisation for acute haemoptysis control; long-term antifungal therapy with voriconazole 200 mg twice daily or itraconazole to slow progression; surgical resection of the cavities is definitive if the patient has adequate respiratory reserve. TB should be excluded with culture before diagnosing CPA (both can coexist).
Scenario D: A 55-year-old woman with relapsed AML on salvage chemotherapy develops fever on day 12 of neutropenia (ANC 80/µL) despite 6 days of piperacillin-tazobactam. HRCT chest shows a 2.5 cm right lower lobe nodule with a surrounding halo of ground-glass opacity. Serum galactomannan: 0.6 (positive — cut-off 0.5 for probable IPA in high-risk patients).
Analysis: Prolonged neutropenia + new pulmonary nodule with halo sign + positive galactomannan = probable invasive pulmonary aspergillosis (IPA) (EORTC/MSG criteria — host factor + CT criterion + mycological criterion). Start voriconazole immediately (IV loading 6 mg/kg 12-hourly × 2 doses, then 4 mg/kg 12-hourly, transitioning to oral when feasible). Note: galactomannan can be falsely positive with piperacillin-tazobactam — but the combination of clinical context + CT findings + positive galactomannan makes probable IPA the working diagnosis. Monitor voriconazole trough levels (target 1–5.5 µg/mL) — important for efficacy and toxicity monitoring.
Integrating the Clinical Picture: Recognising Fungal Infection in Practice
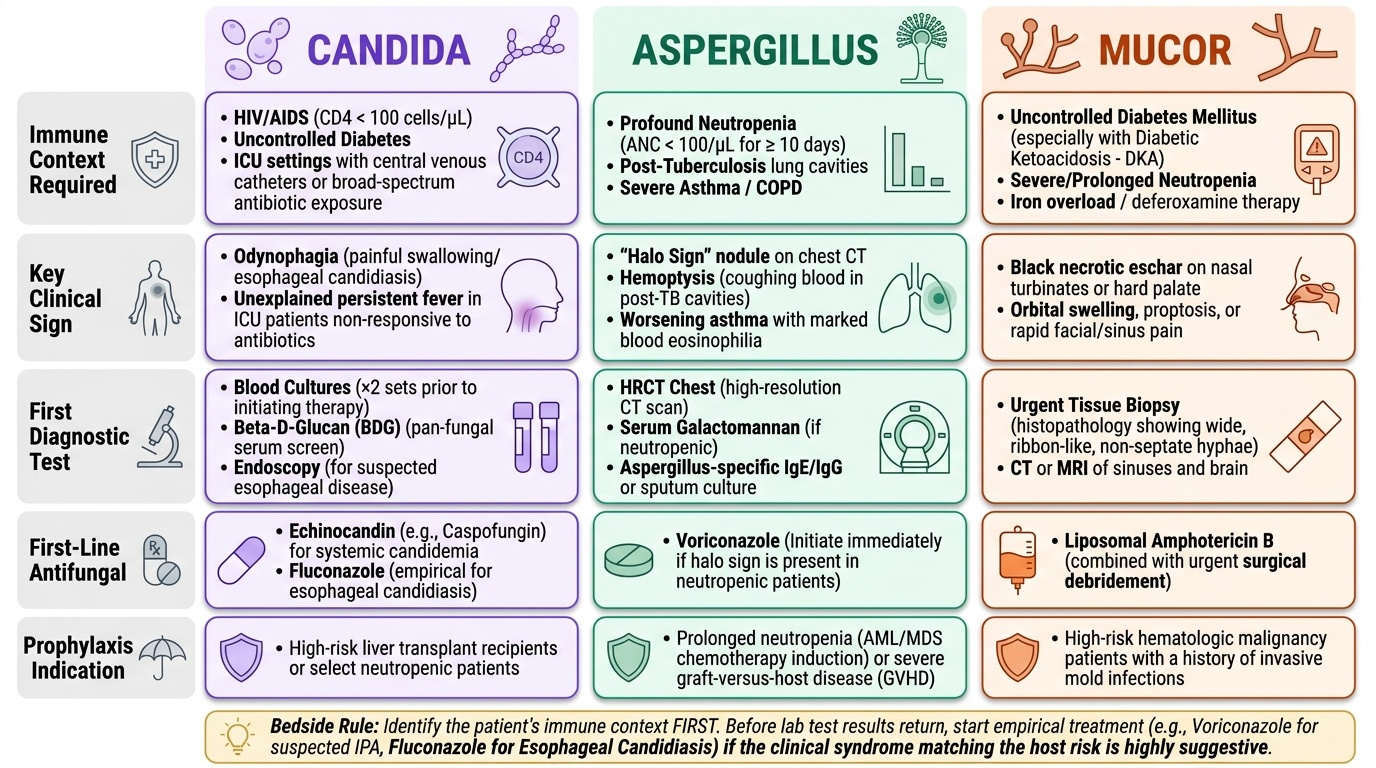
Recognising invasive fungal infection requires synthesising the host immune context, clinical syndrome, and laboratory findings into a unified diagnostic impression. The following framework consolidates the key decision points from this SDL into a practical bedside approach.
Provided image
The immune-context filter — ask first, test second: Before ordering any fungal test, identify the patient's immune risk category. A patient with profound neutropenia (ANC <100/µL for >10 days) who develops new fever and a halo-sign nodule on CT has probable IPA regardless of pending galactomannan results — start voriconazole now. A patient with HIV and CD4 <100 who develops odynophagia has oesophageal candidiasis until proven otherwise — start fluconazole empirically while arranging endoscopy. A patient with well-controlled diabetes who develops fever after a course of broad-spectrum antibiotics may have candidaemia — blood cultures are the next step, not empirical antifungals. The immune context narrows the probability of each fungal diagnosis before any test result is known.
The diagnostic testing hierarchy by setting:
- ICU / neutropenic patient: blood cultures (×2 before antifungals) + serum galactomannan (if neutropenic, for Aspergillus) + beta-D-glucan (pan-fungal screen) + HRCT chest (if respiratory symptoms)
- HIV patient with pulmonary infiltrates: serum cryptococcal antigen (CrAg) + sputum Aspergillus culture + LDH (PCP marker) + BAL if available
- Post-TB patient with haemoptysis: HRCT chest for aspergilloma + serum Aspergillus IgG + sputum culture (Aspergillus)
- Asthmatic with worsening control + eosinophilia: total IgE + Aspergillus-specific IgE/IgG + HRCT chest (central bronchiectasis) → ABPA protocol
Prevention of invasive fungal infections: In the highest-risk populations — AML patients during remission-induction chemotherapy — posaconazole 300 mg daily is the standard antifungal prophylaxis, reducing the incidence of IPA and improving survival. For HIV patients with CD4 <100 cells/µL, fluconazole secondary prophylaxis after oesophageal candidiasis reduces relapse. In solid organ transplant recipients, the prophylaxis regimen (fluconazole or voriconazole or micafungin) is institution- and organ-specific and covers the first 3–12 months post-transplant when immunosuppression is most intense. Prophylaxis decisions should always weigh the absolute risk of infection against the costs and adverse effects of long-term antifungal exposure.
CLINICAL PEARL
Three critical clinical pearls for fungal infections: (1) In candidaemia, CVC removal is as important as antifungal therapy — Candida biofilm on catheter surfaces is treatment-resistant, and the CVC must be removed and replaced at a new site immediately after candidaemia is diagnosed. (2) The halo sign on HRCT (nodule + surrounding ground-glass halo) in a neutropenic febrile patient is probable invasive pulmonary aspergillosis until proven otherwise — start voriconazole immediately and do not await confirmatory galactomannan results (treatment delay in IPA significantly increases mortality). (3) ABPA is a hypersensitivity disease, not an invasive fungal infection — its primary treatment is corticosteroids (prednisolone), with itraconazole as an adjunct to reduce fungal antigen load; amphotericin B has no role in ABPA.